Article Text

Abstract
The complement system is activated following acute myocardial infarction (AMI). Heart fatty acid binding protein (H-FABP) is a sensitive early biomarker of myocardial necrosis that can be used to confirm or exclude a diagnosis of AMI and to monitor recurrent infarction. This study was designed to detect changes in C3, C4 and H-FABP after AMI. Forty patients with AMI and a control group of 40 apparently healthy people were included. Selections were based on inclusion and exclusion criteria. The baseline characteristics were not significantly different between the groups. Patients’ blood samples were collected within 12 h of admission. Significant increases in C3 (AMI group 1.4260+0.04, healthy group 1.26040+0.04; p<0.05), C4 (AMI group 0.29305±0.013, healthy group 0.20860±0.012; p<0.05) and H-FABP (AMI group 12.3±1.69, healthy group 0.16±0.057; p<0.001) were seen in patients with AMI. The correlation between serum C3 and body mass index (BMI, r=0.33; p<0.05), serum C4 and BMI(r=0.313; p<0.05), serum C3 and total cholesterol high density lipoprotein (HDL, r=0.32; p<0.05), serum C4 and HbA1C (r=0.335; p<0.05) and serum C3 and troponin I (r= 0.325p<0.05) was found to be significant. But the correlation between serum C3 and waist:hip ratio (p=0.56), serum C4 and waist:hip ratio (p=0.83), serum C4 and total cholesterol HDL (p=0.993), serum C3 and HbA1C (p=0.440), serum C3 and random blood sugar (p=0.563), serum C4 and random blood sugar (p=0.828) and serum C4 and troponin I (p=0.373) was not significant. The significant complement activation detected in the plasma of patients with AMI indicated that complement plays a part in the pathogenesis of myocardial infarction. A significant increase of H-FABP improves the diagnosis of AMI.
- Myocardial Ischaemia And Infarction (IHD)
- Imaging And Diagnostics
Statistics from Altmetric.com
Introduction
The complement system is thought to have an important role in the pathogenesis of ischaemia-induced myocardial damage. A variety of factors may mediate the neutrophilic infiltration following tissue damage, one of which is the complement system of serum proteins.
Activated components of complement are potent chemotactic and stimulatory agents for neutrophils and hence initiate infiltration into the extravascular myocardial tissue. It has been reported that substances present in the mitochondria-rich subcellular fractions of heart muscle can activate both the classical and alternative pathways.1–9 The complement-derived anaphylatoxins, C3a and C5a, may themselves contribute to the cardiac dysfunction accompanying myocardial ischaemia. C3a, apart from eliciting chemotaxis, enhances vascular permeability and provokes the release of mediators such as histamine, leukotriene, prostaglandins and platelet activating factor and also produces coronary constriction.8,10 Therefore, therapeutic agents targeted at inhibition of inflammatory processes are likely to be beneficial. Treatment which targets complement requires detailed knowledge of the activation mechanisms and mediators responsible for the inflammation, to enable optimal inhibitory treatment.11 Increased levels of complement activation products in plasma samples indicate that complement has been activated. Thus this study was designed to test the hypothesis that the serum levels of complements (C3, C4) in patients with acute myocardial infarction (AMI) are higher than those in healthy subjects without AMI.
If an acute coronary syndrome (ACS) is undetected, this may lead to excess morbidity and mortality that might have been prevented with treatment. An initial ECG of a patient with AMI does not always disclose ST-segment elevation or Q-wave changes, indicative of infarction.12 ,13 Of those people who have a heart attack and later die, 1–10% have major damage to the heart muscle initially or additional damage at a later time. So it is essential that a heart attack is detected well before the onset of irreversible damage. Biomarkers of cardiac ischaemia are raised in blood plasma after a delay of several hours and therefore cannot be used to detect ACS at an early stage.14 General practitioners, however, often see patients suspected of ACS shortly after the onset of complaints. In AMI, heart fatty acid binding protein (H-FABP) is rapidly released from damaged cardiomyocytes into the circulation owing to its small size. H-FABP levels are significantly raised above their threshold level within 1–3 h after AMI and subsequently return to normal values in 12–24 h.15 ,16 H-FABP is 10-fold lower in skeletal muscle than in heart muscle, and the amounts in the kidney, liver and small intestine are even lower,17 so, H-FABP is a sensitive biomarker of myocardial necrosis that could be used to confirm or exclude a diagnosis of AMI and to monitor recurrent infarction.18 Therefore, the aim of this study was to test the hypothesis that serum levels of H-FABP in patients with AMI are higher than those in healthy subjects without AMI.
Methods
Study population and study design
The protocol was approved by the ethical review committee of the Diabetic Association of Bangladesh, Dhaka, Bangladesh. The study was carried out at the department of immunology of Bangladesh Institute of Research and Rehabilitation in Diabetes, Endocrine and Metabolic Disorders (BIRDEM) between January 2011 and December 2011. It was a case–control study and a non-randomised sampling technique was used. Forty patients presenting with an AMI and admitted to the Ibrahim Cardiac Hospital and Research Institute and coronary care unit of BIRDEM hospital were included in the study. Diagnosis was confirmed by typical ECG patterns and cardiac enzyme elevation. Exclusion criteria included autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis and vasculitis, recurrent bacterial infections, hereditary and acquired angio-oedema, various types of kidney diseases, including glomerulonephritis, lupus nephritis and membranous nephritis, liver diseases, serum sickness, any kind of acute inflammatory diseases. At admission, patients’ demographic data, clinical characteristics and current drug treatment were recorded. Forty apparently healthy people served as control subjects.
All participants provided informed consent.
Laboratory data collection
Aseptic precautions were taken and 5 ml blood samples were collected. The blood was allowed to clot at room temperature and serum was separated from the clot as soon as possible by centrifugation (2000 rpm for 15 min). Samples were kept at −70°C until tested. C3 and C4 were determined in serum by immunonephelometry on BN* Systems (Dade Behring, Marburg, Germany; made in the USA). Normal serum or plasma levels in healthy individuals of C3 are 80–170 mg/dl and of C4 20–50 mg/dl. Quantitative measurement of human H-FABP in serum was by an ELISA—a sandwich enzyme immunoassay. Normal serum/plasma in healthy individuals of H-FABP are about 1.6 ng/ml.
Statistical analysis
All results or continuous variables were expressed as mean±SEM. Comparison between groups was carried out by the Student t test for continuous variables, where appropriate. Categorical data were analysed by χ2 test. A p value of <0.05 was considered significant. Calculations were performed with SPSS for Windows (V.17.0).
Results
The AMI and control groups each comprised 40 subjects. Data obtained are summarised in table 1. There was no difference in baseline clinical variables between the groups.
Baseline clinical characteristics of the two groups
Mean serum C3 in patients with AMI was 1.43±0.04 g/l and in the control group 1.26±0.04 g/l. A statistically significant difference was seen between the two means (p<0.05; by t test) as described in table 2 and shown in figure 1. Serum C3 correlated with body mass index (BMI; r=0.33, p<0.05); serum total cholesterol high-density lipoprotein (HDL; r=0.32, p<0.05; by t test); troponin I (r=0.325, p<0.05; by t test). The correlation was also analysed between serum C3 and waist:hip ratio, serum C3 and HbA1C, serum C3 and random blood sugar. The relations between them were found to be statistically non-significant.
Comparison of the mean serum level of C3 in patients with acute myocardial infarction (AMI) and controls

The mean serum C3 (g/l) level was 1.43±0.04 in the patients with acute myocardial infarction (AMI) and 1.26040±0.04 in the control group. A statistically significant difference was found between the two means (p<0.05; by t test), indicating that the complement system is activated after AMI.
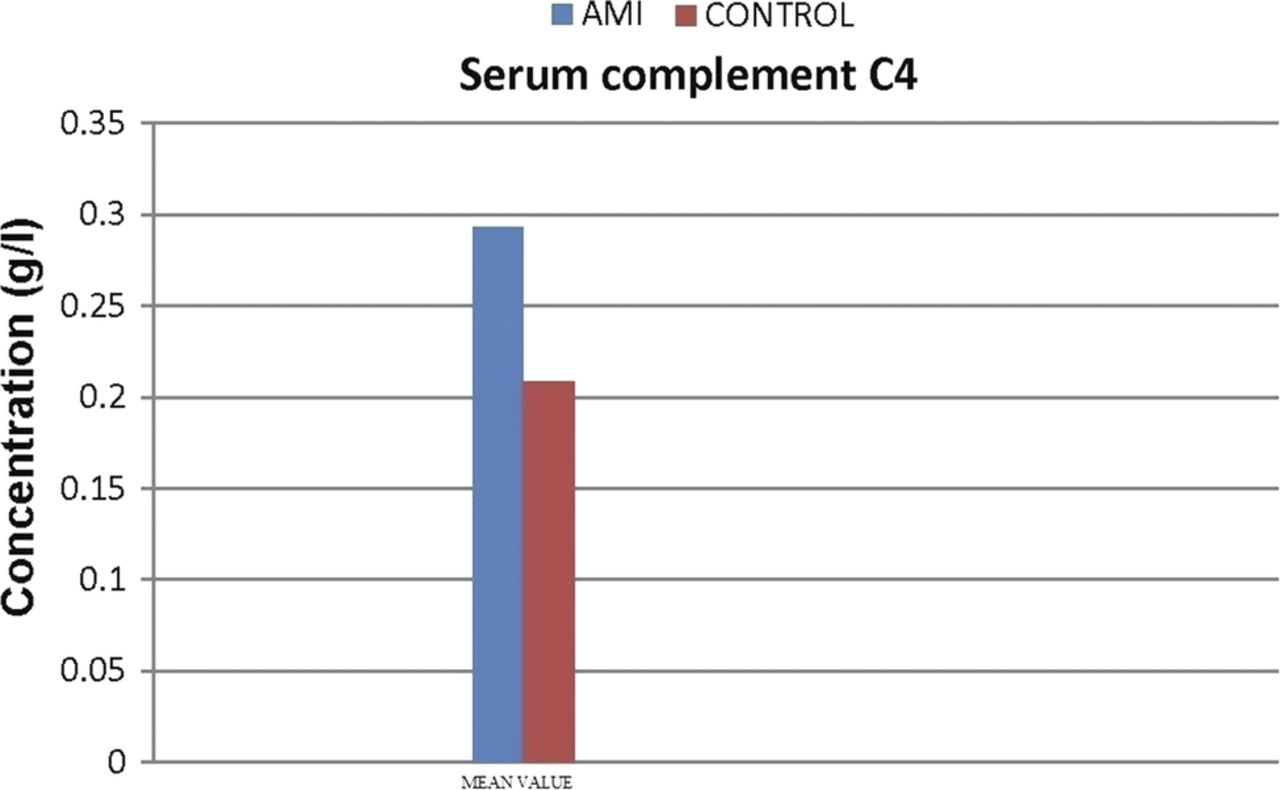
Mean serum C4 in patients with AMI was 0.29±0.013 g/l and in the control group 0.21±0.012 g/l. A statistically significant difference was seen between the two means (p<0.05; by t test) as described in table 3 and shown in figure 2. Serum C4 correlated with BMI (r=0.313, p<0.05) and with serum HbA1C (r=0.335, p<0.05; by t test). The correlations between serum C4 and waist:hip ratio, serum C4 and total cholesterol HDL, serum C4 and random blood sugar and serum C4 and troponin I were analysed and found to be statistically non-significant.
Comparison of the mean serum level of C4 between patients with acute myocardial infarction (AMI) and controls

The mean serum C4 (g/l) level was 0.29±0.013 in the patients with acute myocardial infarction (AMI) and 0.21±0.012 in the control group. A statistically significant difference was found between the two means (p<0.05; by t test). The mean higher level in the AMI group shows that the classical complement system is involved in the pathogenesis of ischaemia-induced myocardial damage.
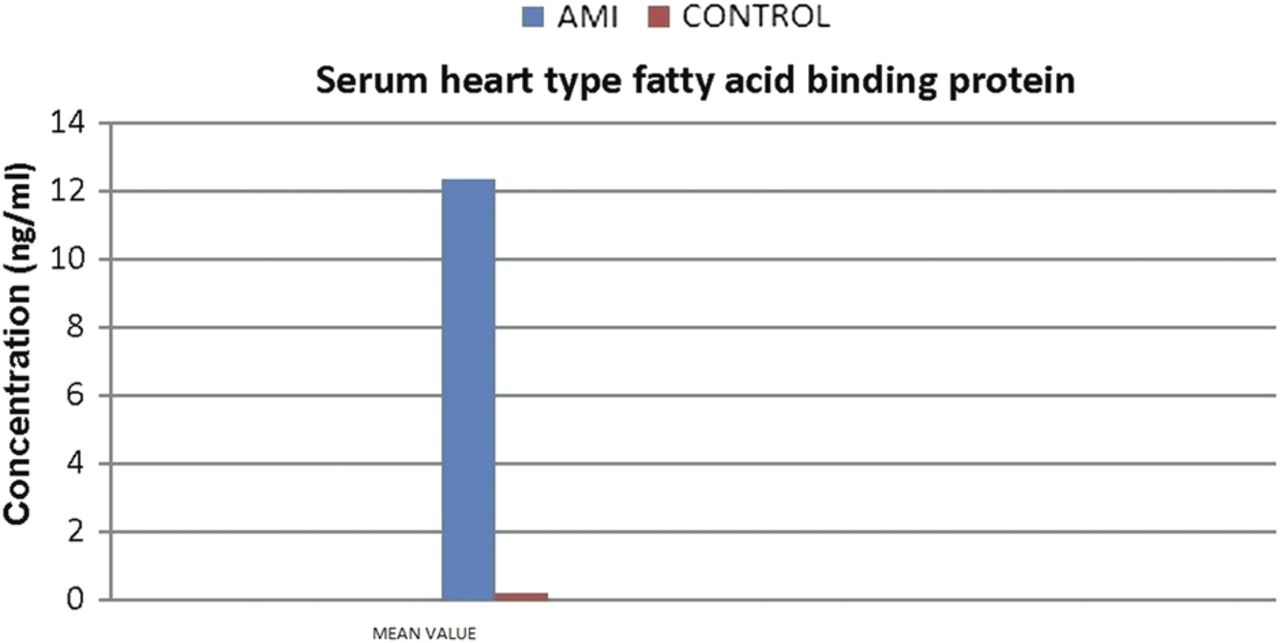
Mean serum H-FABP in patients with AMI was 12.3±1.69 ng/ml and in the control group 0.16±0.057 ng/ml. A statistically significant difference was seen between the two means (p<0.05; by t test) as described in table 4 and shown in figure 3. Currently used biomarkers for cardiac ischaemia are raised in blood plasma after a delay of several hours and therefore cannot detect ACS at an early stage. H-FABP levels are significantly raised above their threshold level within 1–3 h after AMI and subsequently return to normal values in 12–24 h. So, H-FABP is a sensitive biomarker of myocardial necrosis that can be used to confirm or exclude a diagnosis of AMI. This enables appropriate treatment to be given to limit the extent of myocardial cell necrosis.
Comparison of the mean serum level of heart-type fatty acid-binding protein between patients with acute myocardial infarction (AMI) and controls
{kind=link}
{kind=link}
{kind=link}
The mean heart fatty acid binding protein (H-FABP) (ng/ml) was higher in the group with acute myocardial infarction (AMI; 12.3±1.69) than in the healthy control group (0.16±0.057). The difference between the two means was statistically significant (p<0.001). This provides evidence that H-FABP is a sensitive biomarker of myocardial necrosis that can be used to confirm or exclude a diagnosis of AMI.
Discussion
In this study we examined whether changes occur in the serum complements (C3, C4) and H-FABP during AMI. C3 and C4 also correlate with the risk factors of myocardial infarction and troponin I. Levels of C4 and C3 (g/l) were significantly raised in the AMI group in comparison with those in the healthy control group. Several previous studies in experimental models and in humans have shown that the complement system is activated after AMI.1–9 We established that plasma C3 and C4 peak levels were significantly higher in patients with AMI than in the control subjects. The higher level of C4 in the AMI group shows that the classical complement is involved in the pathogenesis of ischaemia-induced myocardial damage. The classical complement pathway can be activated by certain sensitising antibodies, cardiac mitochondrial particles, cardiolipin, or by the fibrinolytic system by directly binding with C1q.9 ,19–21 This activates the C1r and C1s esterase subcomponents of C1 and promotes cleavage of C4 by C1s and subsequently C2 to form C4b2a (C3 convertase), which cleaves C3 to C3a and C3b.22 Subsequent formation of C5 convertase activates the common pathway of the complement cascade leading to the formation of C5b-9, known as the membrane attack complex.
The correlations between serum C3 and BMI, serum C3 and total cholesterol HDL, serum C4 and BMI and serum C4 and HbA1C were found to be significant. These correlations have been examined to determine whether plasma levels of C3 and C4 are risk factors for the incidence of AMI. Engstrom et al (2007)23 showed that C3 and C4 have substantial correlations with cardiovascular risk factors. It has been suggested that the complement system may also be involved in the pathogenesis of atherosclerosis. In a prospective study, increased levels of C3 were found to be predictive for ACS.24 The correlation between serum C3 and troponin I was significant (r=0.325, p<0.05). In another study, plasma C3 and C4 levels in ACS showed a relationship with peak creatine kinase (CK)-MB and troponin I levels. The relationship of C3, C4 levels with peak CK-MB and troponin I levels further suggests that complement activation is related to necrosis within the myocardium.7 Lack of significance between some correlations may be due to the small sample size, which was a limitation of this study. In biological studies the values of these serum markers fluctuate making it difficult to achieve the required level of significance. It was not possible to overcome these limitations owing to a lack of time and money.
Mean H-FABP (ng/ml) was higher in the AMI group than in the healthy control group. The difference between the two means was statistically significant (p<0.001). In AMI, H-FABP is rapidly released from damaged cardiomyocytes into the circulation owing to its small size.16 H-FABP levels are significantly raised above their threshold level within 1–3 h after AMI and subsequently return to normal values in 12–24 h.15 ,16 So, H-FABP is a sensitive biomarker of myocardial necrosis that can be used to confirm or exclude a diagnosis of AMI.18
In summary:
(1) AMI causes activation of the complement system, detectable in the blood stream.
(2) Abrupt complement activation occurs through the classical pathway.
(3) The study explored whether plasma levels of C3 and C4 are associated with increased cardiovascular risk in patients with AMI. The role of complement activation in the progression of atherosclerosis needs prospective clinical studies. The correlation between serum C3 and troponin I suggests that complement activation is related to necrosis within the myocardium.
(4) Determination of H-FABP may improve the diagnosis of AMI, resulting in appropriate treatment to limit the degree of myocardial cell necrosis.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethical review committee of the Diabetic Association of Bangladesh (BADAS), Dhaka, Bangladesh.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.