Article Text

Abstract
Background According to projected estimates, India will bear 60% of the world's cardiovascular disease (CVD) burden by the year 2020. CVD mortality rates are high in South India compared with the rest of India.
Objective The objective of this study was to examine the prevalence of behavioural, biological and metabolic risk factors in different age groups of rural South Indians undergoing coronary interventions under a governmental health insurance scheme.
Methods This study includes 1294 patients who underwent coronary interventions. Age, gender and anthropometric measurements were recorded. History of hypertension, diabetes, smoking and family history of ischaemic heart disease was obtained from every subject. Physical activity was assessed using a General Practise physical activity questionnaire. Investigations like haemogram, blood urea, serum creatinine, fasting and postprandial blood glucose, lipid profile and echocardiography were carried out for all patients.
Results Hypertension was found in 65% patients, 32.38% had diabetes mellitus, 41.65% were smokers (current and former), 37.17% had dyslipidemia, 31.06% had body mass index more than 25 kg/m, 27.04% were physically active, 37% had left ventricular dysfunction, and 8.57% had renal impairment ( table 1). Statistically significant differences were seen in the prevalence rates of different risk factors in the compared age groups (p=<0.05) except for hypertension and dyslipidemia (p=0.596 and 0.306).
Conclusions Risks to health, as an area of study, has recently begun to receive attention in developing countries including India. Population-based strategies aimed at bringing down risk factor levels in the community can translate into major public health benefits.
Statistics from Altmetric.com
Introduction
Demographic trends and lifestyle changes in India envisage a rapid health transition with rising burden of non-communicable diseases (NCDs), particularly coronary heart disease (CHD). As was previously thought, CHD is not a disease of the rich, as it equally affects the poor. There has been a sixfold rise in the burden of CHD in urban areas and a twofold rise in rural areas between the years 1960 and 2000. Three-fourth of the Indian population lives in villages, and the absolute number of CHD patients living in rural India are more (16 million vs 14 million) than those in urban India, with urban Indians having better accessibility to cardiac care compared with rural Indians.1 It is estimated that by the year 2020, India will bear 60% of the world's cardiovascular disease (CVD) burden. There were 2.3 million CVD-related deaths in India in 1990, 2.8 million in 2002, and it is expected to cause an alarming 5 million deaths by 2020.2 CHD is the predominant CVD accounting for 90%–95% of all cases and deaths. It has been calculated that, in 2000, 9.2 million years of productive life were lost in India due to CHD. The projected cumulative loss of national income for India due to non-communicable disease mortality for 2006–2015 will be US$237 billion.2 The recently concluded interheart study has established that nine potentially modifiable risk factors (abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial stress, decreased consumption of fruits and vegetables, moderate consumption of alcohol and physical activity) are responsible for 90% CHD in men and 94% in women irrespective of their age, region and ethnicity.3 The earlier occurrence of acute myocardial infarction observed in South Asian populations was explained by the higher level of risk factors, particularly smoking and diabetes, among Asians. Major differences in cardiovascular disease mortality rates in different Indian states were reported varying from 75–100/100 000 population in the sub-Himalayan states of Nagaland, Meghalaya, Himachal Pradesh and Sikkim, to a high of 360–430/100 000 population in Andhra Pradesh, Tamil Nadu, Punjab and Goa.4 At least 80% of premature deaths from heart disease and stroke could be prevented through healthy diet, regular physical activity, avoiding tobacco and smoking, and control of diabetes and hypertension.2 Lifestyles, diet patterns and cultural practices are not the same across a vast country like India, and these may, in turn, influence the risk factor prevalence rates and mortality rates in various states.5 Collecting data on risk factors and monitoring their trends will help in estimating the future disease burden in a population, and planning of appropriate interventions. Several NCD surveillance and control programmes were launched in India in the last one decade to meet these ends.1
CMR-WHO collaborative initiative on NCD risk factor surveillance 2003–2005 and 2005–2006, World Bank-supported NCD Risk Factor Surveillance under the Integrated Disease Surveillance Project 2007 and National Programme for Prevention and Control of Diabetes, CVD and Stroke 2008 were the programs launched in India to assess the NCD risk factor burden.
The objective of the present study was to examine the prevalence of behavioural, biological and metabolic risk factors in different age groups of rural South Indians undergoing coronary interventions under a governmental health insurance scheme (see online supplementary data).
Methods
This cross-sectional study includes 1294 patients who underwent coronary interventions (percutaneous transluminal coronary angioplasty and coronary artery bypass grafting) in the cardiology department of GSL General Hospital between 1 January 2008 and 29 February 2012 under a governmental insurance scheme meant for people of low socioeconomic status. Approval for this study was received from the ethics committee of the GSL Medical College and General Hospital, Rajahmundry, India. Informed consent was obtained from each participant before the collection of any data. Age, gender and anthropometric measurements, like height, weight and body mass index (BMI) were recorded for all the subjects. History of hypertension, diabetes, smoking and family history of ischaemic heart disease was obtained from every subject. Physical activity was assessed using a General Practice physical activity questionnaire which was found to be more suitable for rural populations. Basic investigations, like haemogram, blood urea, serum creatinine, fasting and postprandial blood glucose, lipid profile and echocardiography were carried out for all patients prior to coronary intervention. The inclusion criteria were age above 25 years, haemoglobin concentration of 10 gm%/dl or more, left ventricular ejection fraction more than 30%, serum creatinine less than 2.5 mg/dl, and no history of allergy to contrast media.
Criteria for risk factors
Hypertension was diagnosed when the patient's blood pressure was >140/90 mm Hg, or was already on antihypertensive medication. Diabetes was diagnosed when the fasting blood glucose was more than 126 mg/dl or post prandial blood glucose (PPBS)>180 mg/dl, or if the patient was already on oral hypoglycaemic agents or insulin. Individuals were classified as non-smokers (never smoked) and smokers (ex-smokers and current smokers). Those subjects who were involved in three or more hours of moderate to vigorous physical activity in a week were considered as active. An early morning fasting blood sample was taken for estimating lipid profile. Total cholesterol to high density lipoprotein cholesterol (HDL) ratio >4.5 was taken as dyslipidemia.6 A BMI=>25 kg/m2 was considered as overweight. Left ventricular ejection fraction <50% was considered as left ventricular dysfunction, and serum creatinine >1.5 mg/dl was considered as renal impairment.
Statistical analyses
All analyses were performed using SPSS software trail V.16.0 and MS-Excel 2007. Fisher's exact test was used to examine differences with categorical variables. Values are presented as mean (±SD). For all statistical analyses, p<0.05 was considered statistically significant.
Results
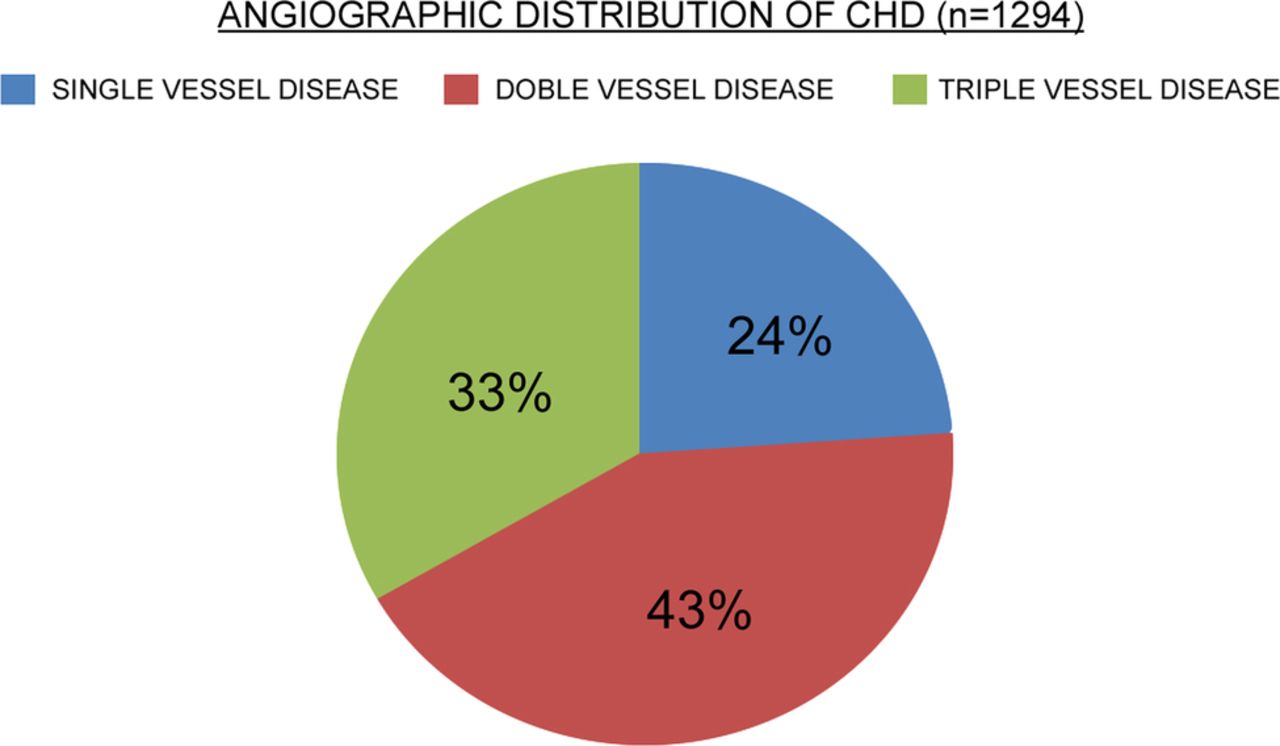
The total number of patients studied was 1294. The mean age of the subjects was 56.4±9.2 years; 877 (67.8%) were men and 417(32.2%) were women. They were divided into three age groups: 189 (14.6%) were in the age group of 25–44 years; 833 (64.4%) were in the age group of 45–64 years, and 272 (21%) were in the age group above 65 years. A total of 551 (42.6%) subjects had single vessel disease, 433 (33.5%) had double vessel disease, and 310 (23.9%) had triple vessel disease (figure 1). Hypertension was found in 65% patients, 32.38% had diabetes mellitus, 41.65% were smokers (current and former), 37.17% had dyslipidemia, 31.06% had BMI more than 25 kg/m, 27.04% were physically active, 37% had left ventricular dysfunction, and 8.57% had renal impairment (table 1). Statistically significant differences were seen in the prevalence rates of different risk factors in the compared age groups (p=<0.05) except for hypertension and dyslipidemia (p=0.596 and 0.306). Increasing age, male sex and hypertension were found to be significant risk factors in all age groups (table 3). Smoking, high BMI, family history of coronary artery disease, left ventricular dysfunction and dyslipidemia were predominant risk factors in the 25–44 years age group (table 2). Smoking, dyslipidemia diabetes and overweight were the predominant risk factors in the 45–64 years age group (table 4). Physical inactivity, dyslipidemia, smoking and renal impairment were found to be predominant risk factors in the above 65 years age group.
Prevalence of cardio metabolic risk factors in rural Southern India (n=1294)
Behavioural risk factors in different age groups in rural Southern India
Biological risk factors in different age groups in rural Southern India
Metabolic risk factors in different age groups in rural Southern India

{kind=link}
Percentage distribution of angiographic CHD among patients in rural Southern India.
Discussion
Focusing on risks to health is the key to preventing disease, but much scientific effort, and most health resources are directed towards treating disease—the ‘Rule of rescue’ still rules. Risks to health, as an area of study, have recently begun to receive attention in developing countries, including India.7 Models of individual risk perception and behaviour which are available in industrialised nations are yet to be developed in developing countries. NCDs now impose the largest health burden in India in terms of number of lives lost, disability and early death. NCDs account for 62% of the disease burden (including accidents) in the country, and mainly affect middle-aged and older age groups which are growing at a faster rate. Most NCD risk factors are inter-related, and strategies to control these risk factors will have beneficial effects in terms of reducing overall disease burden. The three major components of the national programme for prevention of diabetes, CVD and stroke are health promotion for the general population, disease prevention for those at high risk, and assessment of the risk factor burden.8 Persons with NCDs will incur significantly higher treatment costs in terms of out-of-pocket expenses, and this leads to financial distress and impoverishment.9
This study reports on the prevalence of behavioural, biological and metabolic risk factors in patients who underwent coronary interventions, and compares the pattern of distribution of these risk factors in different age groups.
Age
In this study, nearly 2/3 (64.4%) of the CHD patients were in the age group of 45–64 years. Premature morbidity and mortality in the most productive phase of life is posing a serious challenge to Indian society and its economy. A substantial proportion of mortality (28%) in India in the last few years was due to cardiac disease. CVDs largely affect middle-aged and older populations which are growing at a faster rate in India. The population above 65 years of age is expected to increase from 4.4% in 2000 to 7.6% in 2025. The projected figure for the geriatric population in India is 168 million by the year 2026. The health burden from NCDs will rise in parallel with ageing.8
Gender
This study shows male preponderance for CHD. Gender contributes to approximately 40% of the variation in the sex ratios of CHD mortality.10 One of the proposed explanations for the gender difference in cardiovascular disease is hormonal difference. Among women, oestrogen is the predominant sex hormone which may have protective effects through glucose metabolism, haemostatic system, and a direct effect on improving endothelial cell function. The production of oestrogen decreases after menopause, and may change the female lipid metabolism toward a more atherogenic form by decreasing the HDL cholesterol level and by increasing low density lipoprotein and total cholesterol levels. Moreover, risk factors, like abdominal obesity and smoking, are more prevalent in men compared with women.11
Hypertension was found to be the most common risk factor in all age groups. Hypertension is a significant independent risk factor for CHD, morbidity and mortality regardless of age, gender and ethnicity. Worldwide, high blood pressure is responsible for 7.1 million deaths and 64.3 million disability-adjusted life-years.7 The number of hypertension cases in India was 118 million in 2000, and the projected estimates are 214 million cases by 2025.12 The majority of hypertensives were asymptomatic, and most hypertension-related events were non-fatal, contributing largely to morbidity and loss of national productivity. The population-attributed risk for acute myocardial infarction due to hypertension in India is 24%.13
Smoking was the next predominant risk factor in both the 25–44 years and 45–64 years age groups. Smoking and tobacco use are widely prevalent. In both rural and urban populations of India, various epidemiological studies show prevalence rates varying between 24% and 37.6% in different parts of south India (smokeless tobacco/bidis/cigarettes).14 ,15 About 250 million people in India use tobacco, and tobacco accounts for 800 000 to 900 000 deaths every year. Average tobacco consumption in India is around 900 g/adult/year. By comparison with other countries, smoking is an important risk factor in India and is responsible for one in five deaths among men and one in 20 deaths among women.8
Dyslipidemia was the next common risk factor in the 25–44 years, and in the above 65 years age group. A diet high in saturated fat content, heredity and various metabolic conditions, such as diabetes mellitus, influence an individual's level of cholesterol. Cholesterol levels usually rise steadily with age, more steeply in women. Cholesterol is a key component in the development of atherosclerosis, and increases the risks of ischaemic heart disease, ischaemic stroke and other vascular diseases. Dyslipidemia is responsible for 56% of global cardiovascular disease and 18% of cerebrovascular disease.7
Overweight/obesity was seen in more than 40% in the age group of 25–44 years, 32% in the age group of 45–64 years, and 22% in the age group above 65 years. Studies on the prevalence of obesity conducted in this region show prevalence rates varying from 32% to 38% in rural areas, and 36% to 49% in urban areas.14–16 Overweight and obesity lead to adverse metabolic effects on blood pressure, cholesterol, triglycerides and insulin resistance. Risks of CHD, ischaemic stroke and type 2 diabetes mellitus increase steadily with increasing BMI. Type 2 diabetes mellitus—confined to older adults for most of the 20th century—now affects obese children even before puberty. The key causes are increased consumption of energy-dense foods high in saturated fats and sugars, and reduced physical activity.17 The projected estimate for an obese population in India is 52.1 million by 2030.
Physical inactivity. Only 11% in the age group above 65 years, 28% in the age group of 45–64 years, and 45.6% in the age group of 25–44 years were physically active. The global estimate for prevalence of physical inactivity among adults is 17%, ranging from 11% to 24%.9 In general, physical activity improves glucose metabolism, reduces body fat and lowers blood pressure; these are the main ways in which it is thought to reduce the risk of cardiovascular diseases and diabetes. Participation in physical activity can improve musculoskeletal health, control body weight, and reduce symptoms of depression. Physical activity is also associated with lower risk of colon, breast and prostate cancers.18 ,19 Physical activity is an inexpensive investment for national health.
Diabetes
Besides hypertension and smoking, diabetes was found to be an important risk factor in the 45–64 years age group, and in the above 65 years age group. Diabetes is second only to CVD as a health burden in India. During the past one decade, the number of people with diabetes in India increased from 32 million to 50 million, and the projected figure may reach 87 million by 2030.20 Around 60% of low-income patients borrow, mortgage or sell their property just to keep their blood sugar levels under control.7 Hyperinsulinaemia, insulin resistance, and the higher rate of prevalence of metabolic syndrome in people with type 2 diabetes were attributed to high coronary risk in south Asians. In Chennai, India (formerly Madras), in an urban population study, the prevalence rates for coronary artery disease were 9.1% in normal subjects and 21.4% in those with type2 diabetes.21–23 The attributable risk due to diabetes for myocardial infarction was 9.9% in the interheart study.22
Left ventricular dysfunction was seen in 40.2% patients in the 25–44 years age group, 29% in the above 65 years age group, and 25% in the 45–64 age group. Left ventricular dysfunction is associated with increased morbidity and mortality and is responsible for increased number of hospital admissions. The prognosis and management options vary depending on the degree of left ventricular dysfunction.24
Positive family history for coronary artery disease was present in 21% of those in the age group of 25–44 years, 16% of those in the age group of 45–64 years, and 7% of those above 65 years of age. Family history reflects not only genetic susceptibility, but also interactions between genetic, environmental, cultural and behavioural factors. Individuals with genetic susceptibility develop disease at an earlier age. Early detection of CHD in these individuals may help in risk factor modification.25 Non-invasive methods, like coronary calcium scoring, might help predicting CHD in these patients. Some studies indicate that positive family history is a predictor of impaired endothelium-dependent coronary blood flow regulation in human beings.26
Impaired renal function was seen in 10.3% of patients in the age group above 65 years, 9% in the age group of 44–65 years, and 4.23% in the age group of 25–44 years. Renal dysfunction has a major impact on cardiac mortality, and renal failure worsens the outcome of the coronary bypass grafting and percutaneous coronary interventions.27 Both the Kidney Early Evaluation programme and the National Health and Nutrition Examination Survey have revealed association between renal impairment and CHD. With the high burden of diabetes mellitus and hypertension, both of which contribute to chronic kidney disease in India, this important risk factor cannot be ignored.28 ,29
Conclusions
This study conducted in rural populations of South India among selected patients undergoing coronary interventions showed age variations in cardiometabolic risk profile. In general, the classical cardiobiological profile is relatively worse among the youngest patients (25–44 years of age) compared with older patients (45 years of age and above). The fact that the youngest adult patients (25–44 years of age) have a twofold increased rate of being obese compared with the oldest patients (>64 years of age) is certainly a matter of concern. One in five of the youngest adults also report to have a family history of CHD compared with one in 15 among the oldest patients. It is also worrying that one in four of the youngest adult patients are diabetic.
Such worsening trends in the cardiometabolic profile among a younger cohort in this selected group of cardiac patients in rural India indicate two underlying phenomena: first, a more aggressive cardiovascular preventive strategy is necessary, and second, the cardiometabolic risk profile is of relatively recent origin. Such conclusions are important particularly when this group of selected patients is privileged to fall within the government health insurance scheme (see online supplementary data).
In addition, targeted interventions aiming at modifying behavioural cardiac risk factors in younger adults can prevent or postpone the development of cardiometabolic risks at an early age, as behavioural risks ultimately lead to metabolic risks. Nevertheless, considering the socioeconomic implications of such a worrying trend, a comprehensive population-based cardiovascular strategy integrated into the ongoing national health programmes is imperative. A 2% annual reduction in NCD mortality in India for the next 10 years would result in an economic gain of US$15 billion for the country.30
Acknowledgments
The authors would like to acknowledge the encouragement of the management and administration, GSL Medical College and General Hospital, and Arogyasri department for their help in preparing this manuscript. The authors are also thankful to N Lakshmanrao, Assistant Professor of Community Medicine Department for Statistical Analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All the authors participated in the concept, design, acquisition and interpretation of data, drafted the article, and take responsibility for the final version of the published article.
-
Competing interests None.
-
Ethics approval Institutional ethics review committee of GSL Medical College.
-
Provenance and peer review Not commissioned; externally peer reviewed.