Article Text

Abstract
Objective To determine the relationship between maximal oxygen uptake (VO2max), as determined by the Bruce protocol, and selected risk factors for cardiovascular disease (CVD) in an North Indian population.
Design Cross-sectional design.
Setting The study was carried out at Fortis Escorts Hospital, Amritsar, Punjab, India.
Patients 105 CVD patients.
Interventions All patients were subjected to a symptom-limited treadmill test and their fasting blood lipid parameters were measured.
Main outcome measures (a) Body composition; (b) blood lipid parameters; (c) haemodynamic measurement (heart rate at rest and during exercise); (d) physical activity questionnaire (perceived functional ability, physical activity score and physical activity readiness).
Results VO2max was found to be negatively associated with age (r=0.192), body mass index (r=0.163), waist circumference (r=0.197), hip circumference (r=0.208) and percentage of body fat (r=0.238); positively correlated with perceived functional ability (r=0.580), physical activity readiness (r=0.534), physical activity score (r=0.784), maximum heart rate (r=0.236) and metabolic equivalents (r=0.938); and showed no association with total cholesterol (r=0.102), triglycerides (r=0.079) and high-density lipoproteins (r=0.153).
Conclusion VO2max was associated with body composition parameters but did not show any relation with blood lipid parameters. The most significant association was found between VO2max and the physical activity questionnaire.
- Cardiovascular diseases
- aerobic capacity
- blood lipid profile
- hypertensive heart disease
- education
- cardiac rehabilitation,atherosclerosis
- atherosclerosis
- risk factors
- risk stratification
- epidemiology
- public health
- lipids
Statistics from Altmetric.com
- Cardiovascular diseases
- aerobic capacity
- blood lipid profile
- hypertensive heart disease
- education
- cardiac rehabilitation,atherosclerosis
- atherosclerosis
- risk factors
- risk stratification
- epidemiology
- public health
- lipids
Introduction
The emergence of the cardiovascular disease (CVD) epidemic in developing countries has contributed a greater share to the global burden of CVD in the past two to three decades.1 2 The WHO's annual report for the year 2000 indicates that coronary heart disease (CHD) is one of the main causes of mortality in developing, industrial and underdeveloped countries.3 North Indian men and women have higher rates of incidence of and mortality from CVD.4 5 Studies have shown that individuals with an inactive lifestyle are prone to CHD twice as much as those with an active lifestyle,6 thus indicating that physical inactivity and low aerobic capacity are equally important predictors of mortality in CVD as conventional risk factors such as smoking, hypertension, overweight and diabetes.7–9
Aerobic capacity forms an important part of an individual's capacity to efficiently perform activities of daily living and is closely related with health and quality of life.10 The maximal oxygen uptake (VO2max) indicates the functional capacity of cardiorespiratory function and is often considered as the benchmark indicator of cardiorespiratory fitness.11
Many risk factors have been linked to the development of CVDs. Being overweight and obese increases the risk of developing CVD.12 North Indians are unique in that they show a predisposition towards development of CVD even with lower body mass index (BMI).13 14 It has been proved that waist circumference, which is closely related to intra-abdominal fat,15–17 is a more important predictor for the development of CVD, with waist circumference also being closely related to the lipid profile.18 Aerobic capacity has been associated with lipid parameters in adolescents and children,19 20 and with lipid parameters, waist to hip ratio, BMI and percentage of body fat in adults.21
A patient diagnosed as having cardiac disease who is on medication undergoes lifestyle changes that alter the risk factors and improve the aerobic capacity. Since no study has investigated the relationship between these risk factors and aerobic capacity in patients diagnosed as having cardiac disease, this study aimed to explore this association in such a population of patients with cardiac disease for more than 1 year.
Methods
Participants
This study was carried out on patients presenting to the superspecialty Fortis Escorts Hospital in Amritsar, Punjab, India. A total of 105 patients with known CVD were evaluated using a symptom-limited treadmill test. The study population comprises a random sample that is representative of the north Indian population with ages in the range of 40–75 years. The patients included those with post-coronary artery bypass graft (n=24), post-percutaneous transluminal coronary angioplasty (n=55), CHD (n=11), intraventricular conduction delay (n=4), left bundle branch block (n=2) and right bundle branch block (n=9). The study was approved by the institutional ethics committee of Guru Nanak Dev University, Amritsar, Punjab, India.
Anthropometric assessment
For anthropometric assessment, the subjects were barefoot and wore minimum clothes. Weight was measured using a Seca scale and height using an incorporated stadiometer with a precision of 1 mm. The skin-fold measurements were assessed using a calibrated Harpenden skinfold calliper. The waist and hip circumferences were measured using a measuring tape that was used for all participants.
Assessment of maximal aerobic capacity
A maximal symptom-limited exercise tolerance test was performed with a treadmill. For safety reasons, and to obtain reliable information on exercise test variables, the tests were supervised by a physician with the assistance of a trained nurse. The ECG, blood pressure and heart rate were recorded during the exercise test. VO2max was used as a measure of cardiorespiratory fitness. Exercise capacity was assessed on a treadmill using the Bruce protocol. VO2max was calculated using the following equations, based on time spent by each patient on the treadmill
VO2max in men: 14.8−(1.379×T)+(0.451×T2)−(0.012×T3)
VO2max in women: 4.38×T−3.9
where T is the total time in fraction of minutes.
The test was interrupted if the subjects presented with cardiorespiratory symptoms or ECG abnormalities. The most common reasons for termination of the exercise test were leg fatigue, exhaustion, breathlessness and pain in leg muscles, joints or back.
Assessment of blood lipid parameters
Blood was collected from the participants after fasting for a minimum of 12 h, and then the fasting glucose, total cholesterol, high-density lipoprotein (HDL), triglyceride (TGL) and low-density lipoprotein (LDL) levels were measured.
Determination of composite index
The metabolic composite index was determined to investigate its relationship with aerobic fitness. Scores were calculated for four variables, namely TGL, HDL, LDL and fasting glucose. For each of these variables, a Z score was calculated as the number of SD units from the sample mean after the normalisation of the variables, that is, Z=((value−mean)/SD). The composite index of blood lipids and fasting glucose is the sum of the four Z scores.22
Assessment of physical activity
The questionnaires used for the assessment of physical activity included the perceived functional ability, physical activity readiness and physical activity score.
Statistical analysis was performed using SPSS V.16 statistical software.
Results
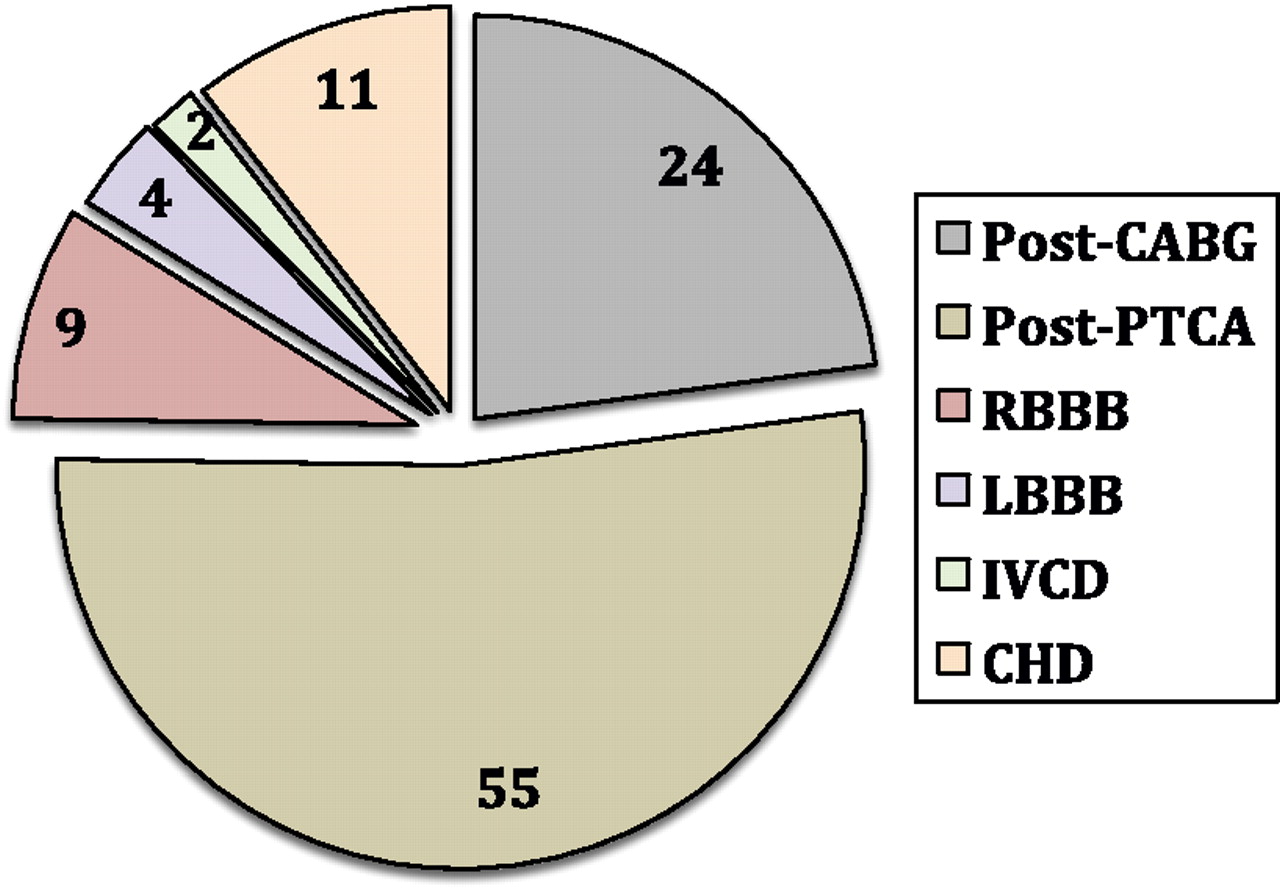
Figure 1 shows the distribution of CVDs in the study population recruited in our study, which included patients with post-coronary artery bypass graft (n=24), post-percutaneous transluminal coronary angioplasty (n=55), CHD (n=11), intraventricular conduction delay (n=4), left bundle branch block (n=2) and right bundle branch block (n=9).

Distribution of cardiovascular diseases in the study population. CABG, coronary artery bypass graft; CHD, coronary heart disease; IVCD, intraventricular conduction delay; LBBB, left bundle branch block; PTCA, percutaneous transluminal coronary angioplasty; RBBB, right bundle branch block.
Table 1 lists the maximum, minimum and mean (SD) values for the anthropometric indices and CVD risk factors. The mean VO2max of the study population was found to be 31.54±7.38 ml/kg/min.
Physical characteristics and lipid profile of the study population
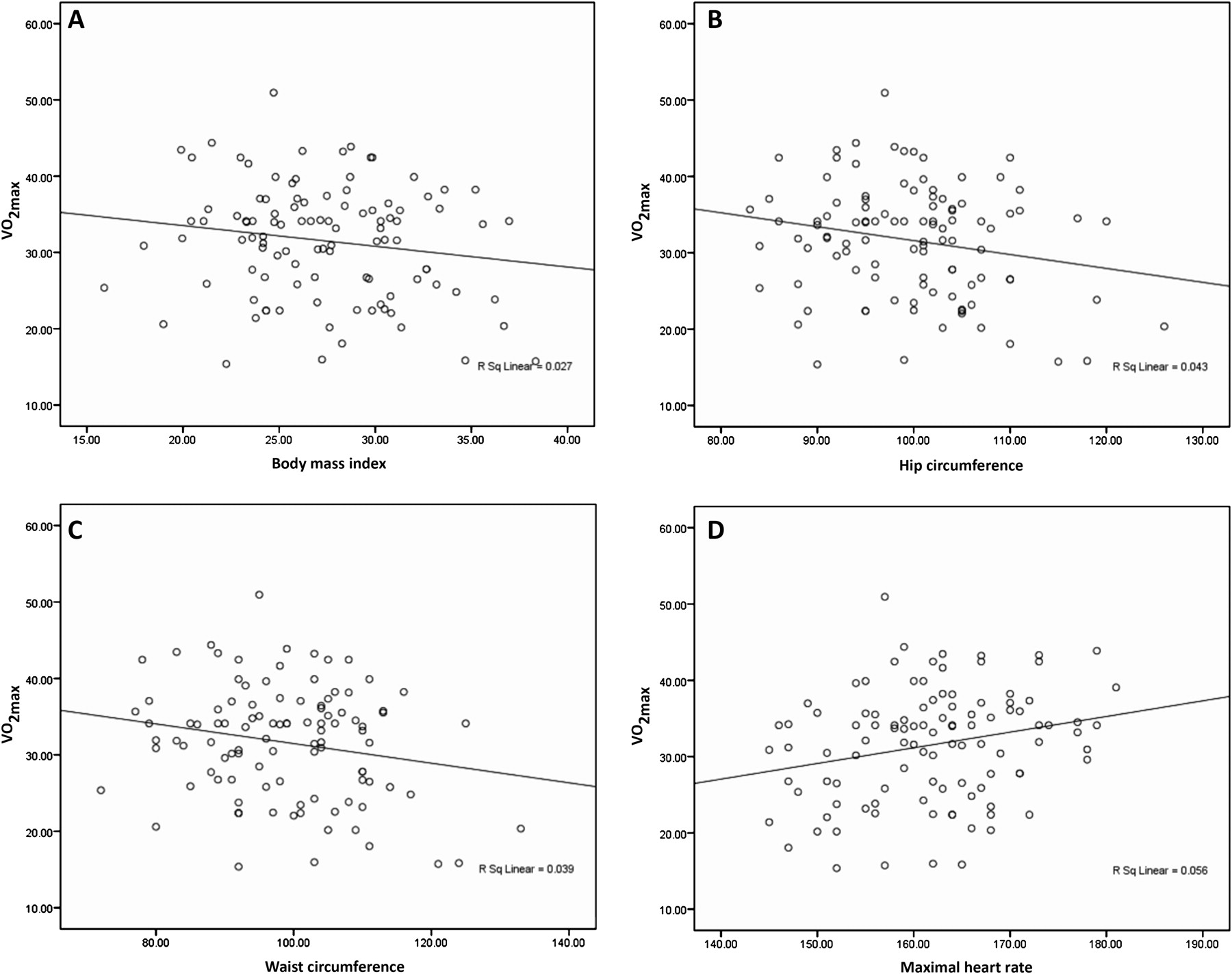
Table 2 indicates that VO2max is significantly correlated with the following parameters: negatively with age (r=0.192), BMI (r=0.163), waist circumference (r=0.197), hip circumference (r=0.208) and percentage of body fat (r=0.238); positively correlated with perceived functional ability (r=0.580), physical activity readiness (r=0.534), physical activity score (r=0.784), maximum heart rate (r=0.236) and metabolic equivalents (r=0.938). There was no association between VO2max and the composite index (r=0.003).
Correlation of VO2max with various parameters
The graphs in figure 2 depict the negative correlation of VO2max with BMI, hip circumference and waist circumference, and the positive correlation with maximum heart rate.
{kind=link}
{kind=link}
Correlation of maximal oxygen uptake (VO2max) with body mass index (A), hip circumference (B), waist circumference (C) and maximal heart rate (D).
Discussion
There is little data regarding association of various risk factors, the strength of their associations in patients diagnosed as having cardiac diseases who are on medications and lifestyle changes. This study was devised to investigate the relationship between VO2max, obesity and lipid profiles of patients with CVD who reported to a superspecialty tertiary care hospital.
The mean VO2max in our study population was found to be 31.54±7.38 ml/kg/min. A similar study on aerobic capacity in cardiac patients reported a value of 27.8 ml/kg/min,23 whereas in age-matched sedentary men the normative value was found to be in the range 32–42 ml/kg/min for the 40–75 years age group.24
We attribute the near-normal VO2max value, compared with age-matched sedentary individuals, in our study population to the fact that most of the patients had their CVD incident/diagnosis at least more than 1 year ago. Most of the patients underwent surgery which would have improved the vascularisation of the heart, which in turn would have promoted better functioning of the heart, followed by a healthier lifestyle and a continuing programme of cardiac rehabilitation. Thus, this stress examination was not the first time the patients were subjected to a stress test.
Association of lipid profile with aerobic capacity
The mean HDL of our study population was 40.70±8.80 mg/dl, which is far below the desirable value of >60 (table 1). The TGLs were found to be elevated, with a mean value of 177.98±85.06 mg/dl. The total cholesterol was found to be within the normal range (154.5±37.28 mg/dl). A diagnosis of dyslipidaemia is made when there are abnormal findings in any two of the four parameters in the lipid profile. Our patients demonstrated increased blood TGL levels and reduced HDL levels, which put them in the dyslipidaemic category.25 Causative factors of dyslipidaemia may be either primary, due to genetic composition, or secondary, due to environmental factors. Both primary and secondary factors are known to cause dyslipidaemia in North Indians, who are more prone to dyslipidaemia due to their genetic makeup. Several studies have found an association between apolipoprotein B gene polymorphisms and hyperlipidaemia in North Indians. The secondary environmental factors that have been proven to predispose North Indians to abnormal lipid profiles include reduced leisure physical activity than in Caucasians, a diet rich in carbohydrates and low in ω3 polyunsaturated fatty acids, and an abnormal fat distribution (ie, high waist:hip ratio) with increased truncal fat, which is known to predispose individuals to insulin resistance and dyslipidaemia.25–29
The total cholesterol level was found to be 154.5±37.288 mg/dl, which is within the normal range of <200 mg/dl. The LDL value was found to be 89.6±28.91 mg/dl, which is also within the normal range of <100 mg/dl. These values could be attributed to the fact that the patients were on lipid-lowering drugs, as LDL and total cholesterol are the primary targets of cholesterol-lowering therapy.30
Based on the observation of a near-normal VO2max, when compared with a sedentary population in a similar age group,24 and an altered lipid profile we decided to explore the correlation of VO2max with blood lipid parameters. VO2max showed a negative relation with total cholesterol (r=0.102), TGL (r=0.079) and LDL (r=0.064), and a positive relation with HDL (r=0.153), but these correlation coefficients were not statistically significant. These findings suggest that HDL increases as the aerobic capacity of the patients increases, while total cholesterol, TGL and LDL decrease. HDL, also called ‘good cholesterol’, transports VLDL (very low-density lipoprotein) and LDL back to the kidneys and liver for their excretion, a process called ‘reverse cholesterol transport’,31 and thus protects against the development of atherosclerosis.32 A low HDL level is also proven to be the strongest predictor of subsequent cardiovascular events in patients with angiographically proven coronary artery disease.33 The low level of HDL and high levels of TGL in our study population imply that although the patients underwent revascularisation surgery, were on medications, underwent lifestyle changes and achieved near-normal VO2max, there is some factor that predisposes North Indians to an altered lipid profile. The reason could be the genetic makeup of North Indians which makes them highly vulnerable to altered lipid profiles.
Association of VO2max with metabolic composite index
The metabolic composite index is the sum of the Z scores of four parameters, namely HDL, TGL, LDL and fasting glucose, which was proposed as a method to investigate the association with aerobic fitness.22 Overweight adolescents demonstrated higher values of the metabolic composite index compared with non-overweight adolescents. This relationship has not been explored in adults or in patients with CVD. Mesa et al demonstrated that in adolescents with the same fitness level, overweight adolescents had a higher metabolic composite index than those who had a normal BMI; however, we did not find any association of this composite index with VO2max in our study. It is possible that medications could have confounded this association in our study.
Association of VO2max and anthropometric characteristics
The mean BMI in our study population was 27.31±4.4 kg/m2, which puts them in the obese category according to the cut-off value for North Indians. The cut-off value for BMI in North Indians is less than that for the Western population. In Western countries, a BMI ≥25 is considered overweight, while for North Indians the value is 23 kg/m2 as North Indians have a higher proportion of body fat in comparison with Caucasians with similar BMI values.13 34 Furthermore, we found a negative correlation of VO2max with BMI (r=0.163), that is, the aerobic capacity reduces as the BMI increases.
The waist circumference is considered to reflect the intra-abdominal fat content of an individual. The normal value for North Indian men is 90 cm and for women is 80 cm.35 We found a mean value of 98.78±11.29 cm for our study population, which is higher than the normal value and implies that the patients predominantly had intra-abdominal obesity. VO2max was also found to be negatively correlated with waist circumference (r=0.197).
We also found that VO2max was inversely related to the percentage of body fat. The correlation of physical activity with BMI and percentage of fat distribution has been demonstrated in patients with metabolic syndrome, which overlap with many symptoms of CVD and may even be considered to be a precursor to cardiac disease.36 Thus, the correlation of aerobic capacity with BMI and percentage of body fat observed in sedentary individuals,37 and patients with metabolic syndrome,36 is also observed in cardiac patients.
Association of VO2max with physical activity questionnaire
The physical activity questionnaires used in this study, namely physical activity rating, perceived functional ability and physical activity score, were strongly associated with VO2max. The individual's perception of his/her physical capacity and subjective effort has been demonstrated to be a fairly accurate indicator of his/her aerobic capacity. The association reported has been so strong that non-exercise-based prediction equations38 39 used for the estimation of VO2max incorporate these questionnaires into their formation.
Although our study only aimed to report the relationship of VO2max with predictors of CVD in North Indians, prospective studies on the association of cardiovascular risk factors and VO2max will give us definite data regarding these associations, since much of the data in cross-sectional studies is diluted by the effect of medications that the CVD patients take.
Conclusion
VO2max was associated with body composition parameters but did not show any relationship with lipid parameters, with patients exhibiting dyslipidaemia despite taking medication to normalise lipid profiles and having an aerobic capacity comparable with an aged-matched sedentary population. The most significant association was found between VO2max and physical activity questionnaires.
Acknowledgments
The authors would like to thank the staff and patients of Fortis Escorts Hospital who extended their full support and cooperation during this study.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the institutional ethics committee of Guru Nanak Dev University.
Provenance and peer review Not commissioned; internally peer reviewed.