Article Text

Statistics from Altmetric.com
- Congenital heart disease
- paediatric cardiology
- heart failure
- imaging and diagnostics
- electrocardiography
A 10-year-old girl presented with NYHA class II dyspnoea and palpitations experienced over the past 1 year. Elsewhere, in the past, she had undergone balloon aortic valvuloplasty for severe aortic stenosis followed by surgical ligation of a large patent ductus arteriosus (PDA), 3 days later. The postoperative period was complicated by infective endocarditis and embolic stroke that improved with antibiotics and physiotherapy, though with mild residual weakness.
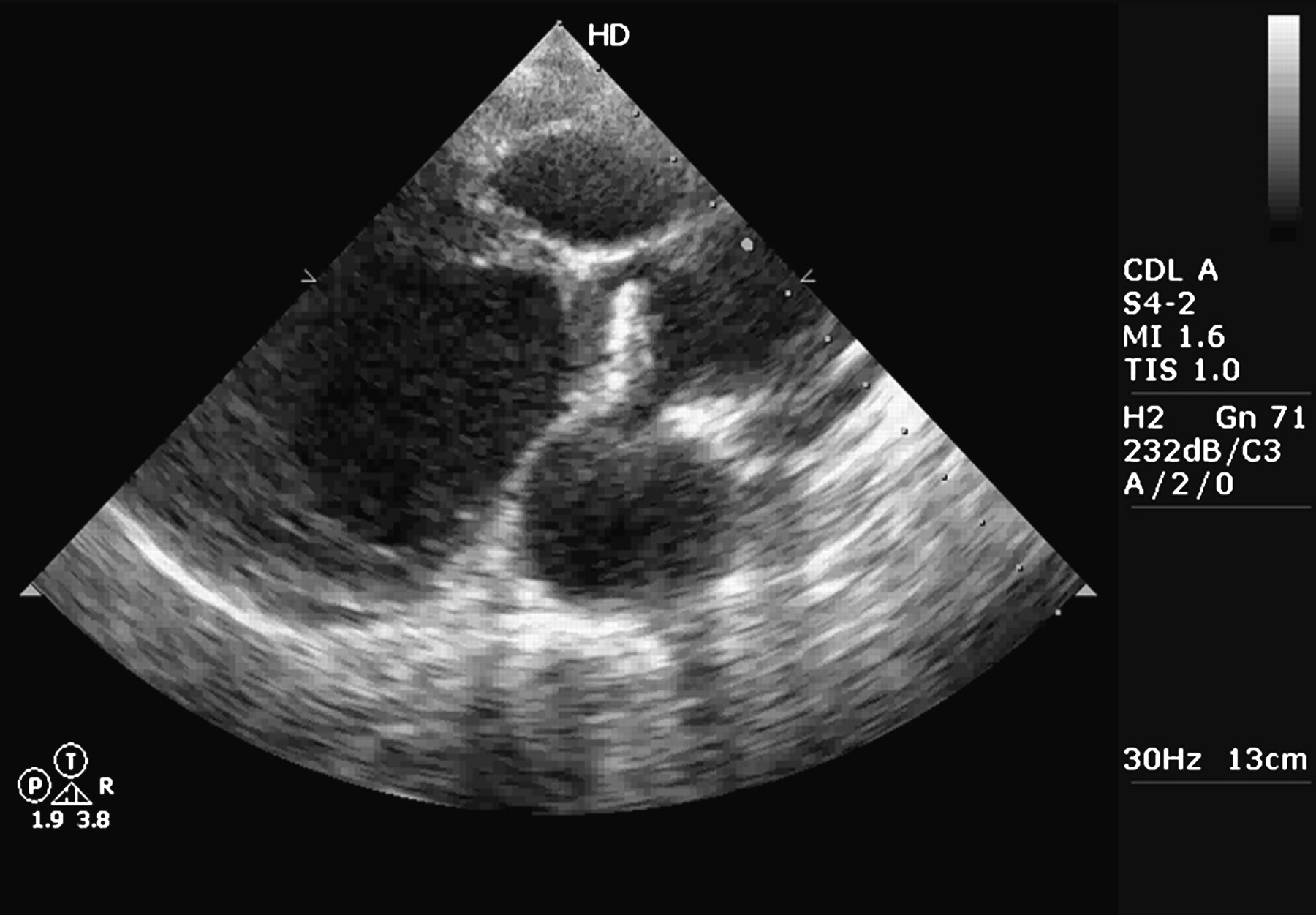
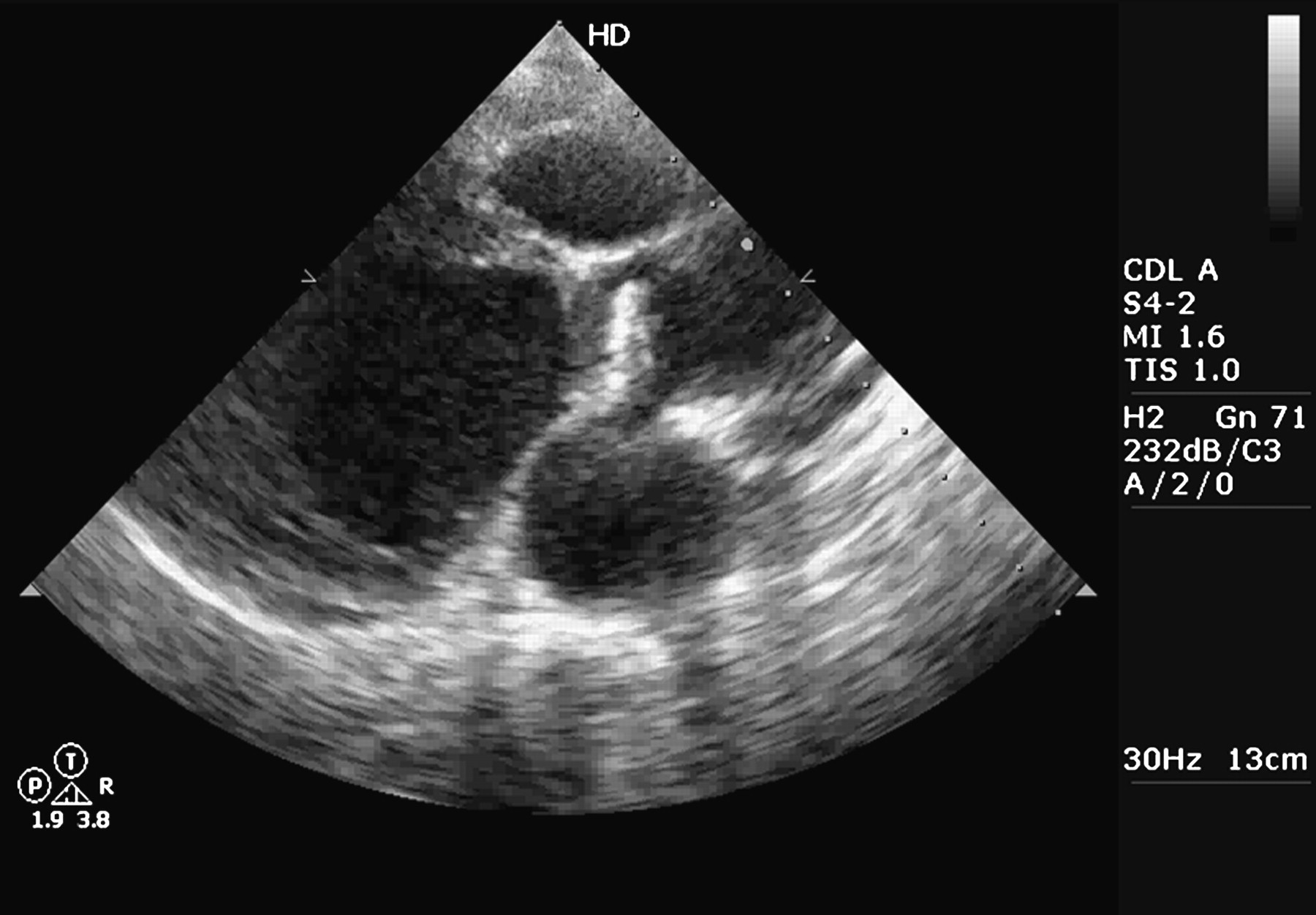
A 2D echocardiography showed a calcified disc-like structure at the aortic valve position that was highly mobile, with its movement typically resembling a single-leaflet tilting disc mechanical valve. In systole (figure 1), it was aligned to the long axis of the ascending aorta mimicking the disc in open position, and in diastole (figure 2), it tilted back to the closing position. There was acoustic shadowing behind the calcified cusp that matched its mobility (online supplement, video 1). This was associated with severe aortic regurgitation (AR) and global left ventricular (LV) dysfunction, hence referred for aortic valve replacement (AVR).

Systolic frame showing the calcified cusp in an open position.
{kind=link}
{kind=link}
Diastolic frame with the calcified cusp in closed position. A sub-aortic membrane can be seen.
Calcification of the aortic valve is attributed to inflammatory and degenerative processes which get accelerated in patients with a bicuspid aortic valve because of altered haemodynamics.1 This case exemplifies the fact that injury, infection and altered flow pattern can lead to significant calcification within 3 years, even in valves as young as this patient's.
Reference
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video 1
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.