Article Text

Statistics from Altmetric.com
We present an interesting case of Horner's syndrome in a patient with interrupted aortic arch (IAA) as a rare and seldom described cause of Horner’s syndrome in an adult.
A 21-year-old young man presented with drooping of left upper eyelid, with miosis, decreased sweating and mild enopthalmos with upper backache since 2 months. On evaluation, severe hypertension was present in right upper limb, absent pulses in left upper limb and unequal and feeble pulses in lower limbs (figure 1).

Clinical photograph of the patient demonstrating Horner's syndrome involving the left eye.
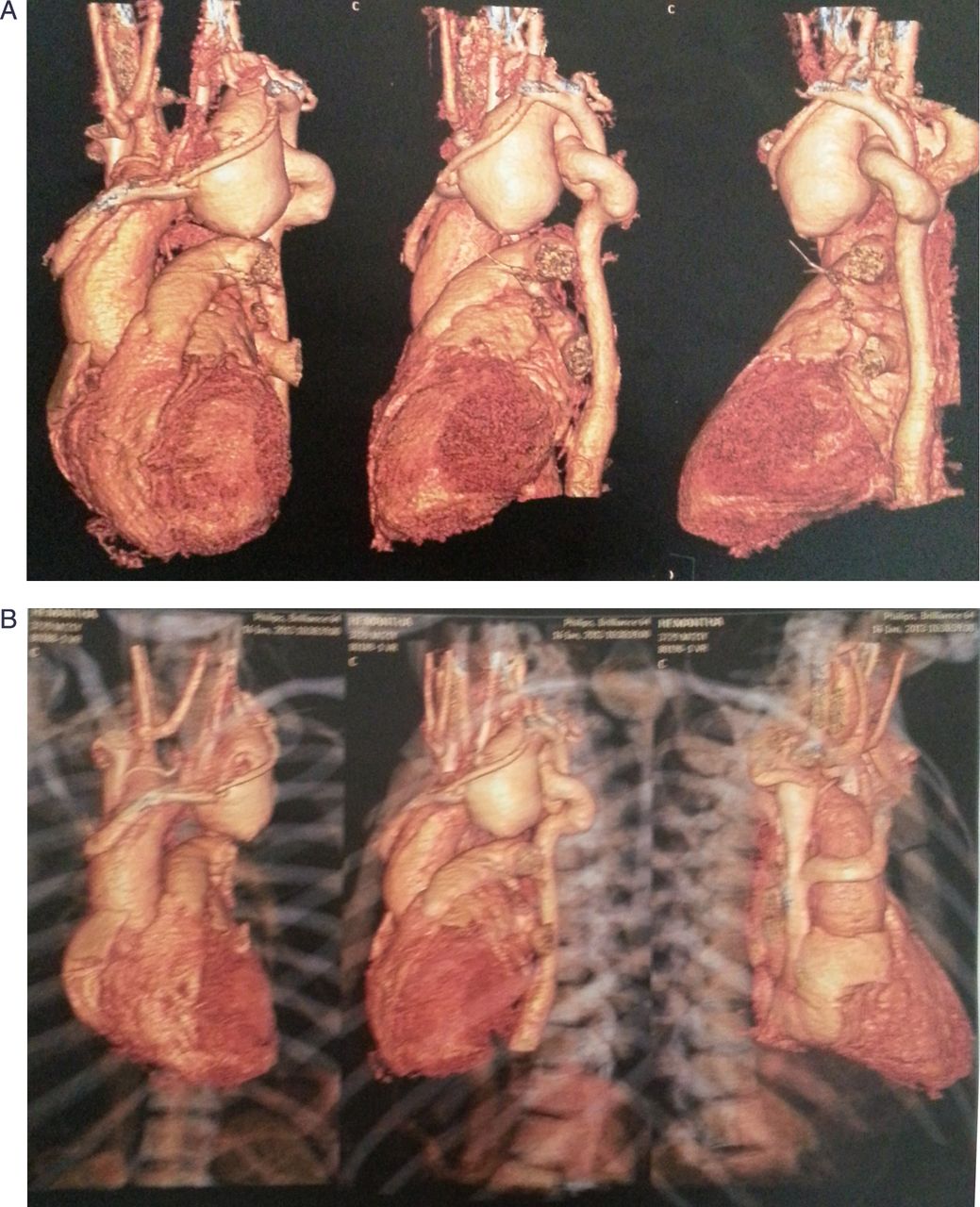
Tran-thoracic echocardiogram showed a left aortic arch with common brachiocephalic trunk and interruption of the aortic arch beyond the common carotid artery (IAA type B). The heart was structurally and functionally normal. ECG showed LV hypertrophy (figure 2). Cardiac CT confirmed IAA type B and revealed a prominent network of very large and tortuous collaterals to descending aorta with aneurysmally dilated left subclavian artery (figures 3A, B). The Horner's syndrome was caused by the compression of the sympathetic plexus by the progressive enlargement of the proximal portion of the aorta which was subsequently proved during surgery and also explains the delayed onset. The patient underwent surgical correction with an artificial graft conduit for the reconstruction of the arch anomaly while the collaterals were left alone in the expectation of spontaneous regression with good results. There was inadequate control of blood pressure in the immediate postoperative period (possibly due to resetting of the pressure receptors) and partial recovery of Horner's syndrome possibly because of residual damage to the plexus.
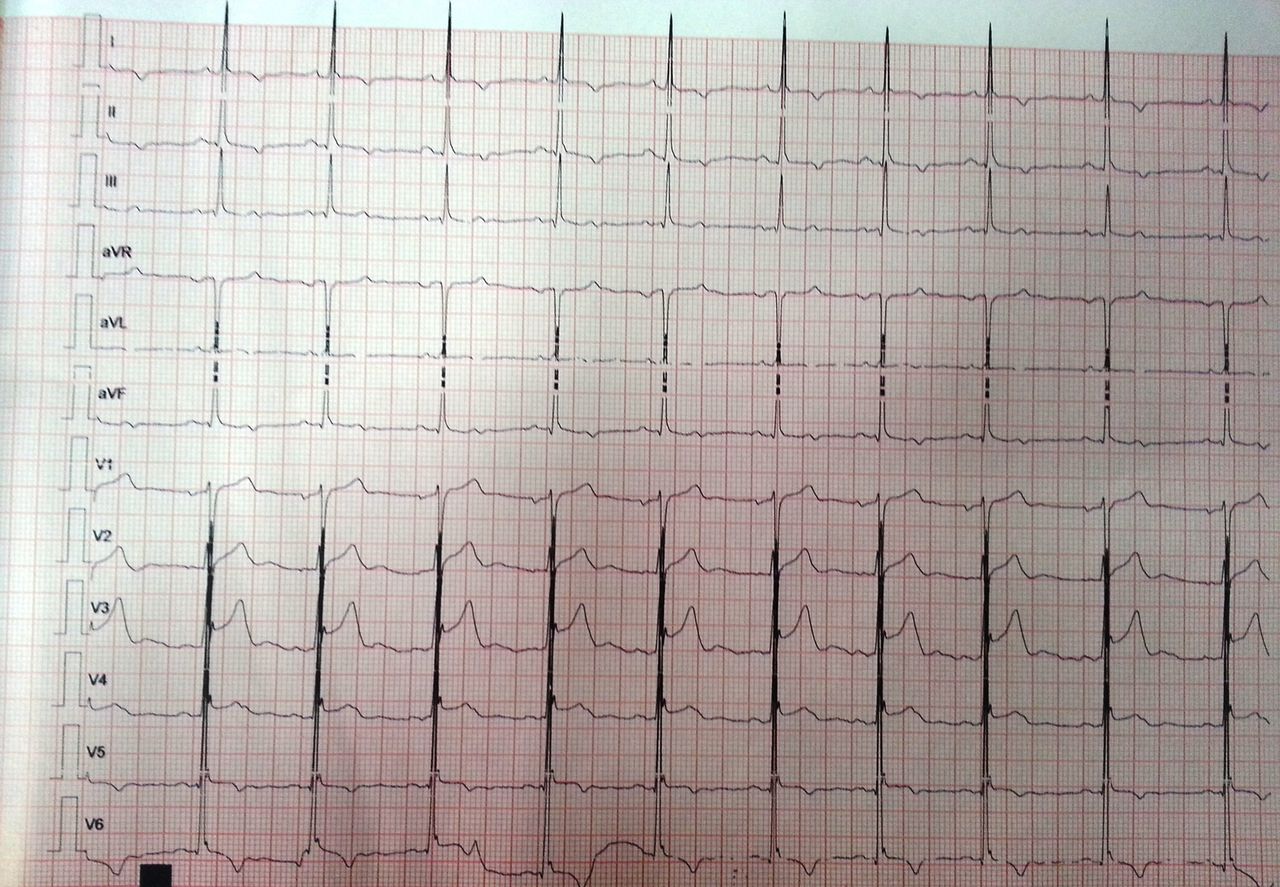
ECG showing LV hypertrophy with corresponding ST-T changes.

{kind=link}
{kind=link}
{kind=link}
(A and B) 3D reconstruction CT aortogram showing interrupted aortic arch with dilated subclavian artery.
IAA is a rare disease with a prevalence of 3/million live births and is a disease predominantly presenting in infancy. Till now there have been very few case reports of IAA in adults and is usually seen to be associated with ventricular septal defect, patent ductus arteriosus, aorto-pulmonary window or truncus arteriosus.1–,3 It may be seen in association with syndromes like CHARGE or PHASE syndrome and Di-George syndrome. The association of Horner's syndrome with IAA has been reported only once.4 The presence of an IAA might be missed clinically as the patient may be completely asymptomatic and in the presence of good collaterals there might not be any asymmetry of pulses and there might be no murmurs and even upper limb hypertension may not always be present. The echocardiogram, ECG and x-ray might appear to be normal.
Footnotes
-
Contributors All the authors have contributed in the drafting of the manuscript and helped in patient care.
-
Funding Institutional funds.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.