Article Text

Abstract
Objective To investigate the effects of antithrombotic therapy on target lesion revascularisation (TLR) and major adverse cardiovascular and cerebrovascular events (MACCEs) at 12 months after femoropopliteal intervention with second-generation bare metal nitinol stents.
Methods A total of 277 lesions in 258 limbs of 248 patients with de novo atherosclerosis in the above-the-knee femoropopliteal segment were analysed from the Japan multicentre postmarketing surveillance.
Results At discharge, dual antiplatelet therapy (DAPT) was prescribed in 68.5% and cilostazol in 30.2% of patients. At 12 months of follow-up, prescriptions of DAPT significantly (p=0.0001) decreased to 51.2% and prescription of cilostazol remained unchanged (p=0.592) at 28.0%. Prescription of warfarin also remained unchanged (14.5% at discharge, 13.3% at 12 months, p=0.70). At 12 months, freedoms from TLR and MACCE were 89.4% and 89.7%, respectively. In a multivariate Cox proportional hazards model, neither DAPT nor cilostazol at discharge was associated with both TLR and MACCE at 12 months. However, warfarin at discharge was only independently associated with TLR at 12 months. Kaplan-Meier estimates demonstrated that warfarin at discharge yielded a significantly (p=0.013) lower freedom from TLR at 12 months than no warfarin at discharge. Freedom from TLR at 12 months by the Kaplan-Meier estimates was 77.8% (95% CI 59.0% to 88.8%) in patients with warfarin at discharge and 91.2% (95% CI 86.3% to 94.3%) in those without warfarin at discharge.
Conclusions Clinical benefits of DAPT or cilostazol might be small in terms of TLR and MACCE at 12 months. Anticoagulation with warfarin at discharge might increase TLR at 12 months.
- peripheral artery disease
- femoropopliteal artery disease
- medical treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The femoropopliteal artery is the most common site of involvement in patients with atherosclerotic peripheral artery disease.
Nitinol stenting has become the standard of care in the treatment of femoropopliteal artery disease.
An appropriate antithrombotic therapy after femoropopliteal intervention remains unclear.
What does this study add?
Freedoms from target lesion revascularisation (TLR) and major adverse cardiovascular and cerebrovascular events (MACCE) at 12 months after femoropopliteal stenting with second-generation nitinol bare metal stent were 89.4% and 89.7%, respectively.
Neither dual antiplatelet therapy nor cilostazol at discharge was associated with freedom from TLR and MACCE at 12 months.
Warfarin at discharge was independently associated with TLR at 12 months, and the 12 month Kaplan-Meier estimates found a significantly lower freedom from TLR in warfarin at discharge than no warfarin at discharge.
How might this impact on clinical practice?
Further studies regarding antiplatelet and anticoagulation therapies in the real-world practice would provide insights into an appropriate antithrombotic therapy after femoropopliteal intervention.
Introduction
The cardiovascular community has been confused about medical management for patients with peripheral artery disease (PAD) undergoing endovascular therapy. It is widely recognised that antiplatelet therapy is an integral part of preventing cardiovascular mortality and morbidity in patients with PAD.1 The femoropopliteal artery is the most common site of involvement in patients with atherosclerotic PAD.2 With technological improvements in the endovascular armamentarium, nitinol stenting could be one of treatment options for femoropopliteal artery disease.3 4 Given the high chance of restenosis and need for further intervention after femoropopliteal intervention, a couple of recent studies have addressed the effects of dual antiplatelet therapy (DAPT), defined the use of a P2Y12 receptor inhibitor and aspirin, and cilostazol in reducing restenosis and repeat revascularisation.5–8 However, few reports are available regarding the effects of antithrombotic therapy after femoropopliteal intervention in the real-world practice.9
The aim of this study was to investigate the effects of antithrombotic therapy on clinical outcomes such as target lesion revascularisation (TLR) and major adverse cardiovascular and cerebrovascular events (MACCEs) at 12 months after femoropopliteal intervention with second-generation bare metal nitinol stents based on results from the Japan multicentre postmarketing surveillance.
Methods
Population
The second-generation bare metal nitinol stent, Misago stent (Terumo Corp, Tokyo, Japan) Japan postmarketing surveillance was performed to evaluate the safety and efficacy of the Misago stent in routine daily practice in the Japanese population. A total of 295 patients who underwent Misago stent deployment were registered between January 2013 and February at 78 sites in Japan. Of these, 277 lesions in 258 limbs of 248 patients with de novo atherosclerosis in the above-the-knee femoropopliteal segment were evaluated. At each participating institution, patients were treated according to the local strategy. The regimen of drugs including antithrombotic agents was decided by the attending physician. TLR was also performed based on the attending physician’s decision. Annual clinical follow-up was scheduled for up to 5 years. The informed consent for the postmarketing surveillance was given by all patients, and the institutional review boards approved the study.
Endpoints
The primary endpoint of this study was TLR at 12 months. The secondary endpoint was the composite outcome of MACCE at 12 months. TLR was defined as any repeat percutaneous intervention or bypass surgery of the target lesion performed for restenosis or reocclusion. MACCE was defined as myocardial infarction, ischaemic stroke and all-cause death. Major bleeding was defined as fatal bleeding.
Statistical analysis
Normally distributed continuous variables are presented as means±SD; they were compared using the t-test. Non-normally distributed variables were compared using the Mann-Whitney U test; categorical baseline variables were compared using Fisher’s exact test, the χ2 test or analysis of variance as appropriate. Cumulative TLR rates and MACCE rates during the follow-up period were estimated using the Kaplan-Meier method and compared using the log-rank test. Cox proportional hazards model was used for univariate/multivariable analyses to assess the influence of factors on TLR and MACCE. Variables with a value of p<0.10 at clinical characteristics analysis were entered into the regression model. Also, the shared-frailty Cox model was conducted with each institute and ID as a random intercept. All statistical analysis was performed with SPSS V.22 and STATA V.14. All p value <0.05 was considered statistically significant.
Results
Baseline characteristics
Overall 248 patients, 258 limbs and 277 lesions characteristics are summarised in table 1. The most prevalent risk factor was hypertension, followed by diabetes mellitus. The mean lesion length was 12.5±9.8 cm, and 41.9% of lesions had chronic total occlusion (CTO). The number of stents implanted was 1.6±0.9.
Demographics and lesion characteristics
At discharge, DAPT was prescribed for 68.5% (170) and cilostazol for 30.2% (75) of patients. Warfarin was prescribed 14.5% (36). The DAPT group had a significantly higher prevalence of previous coronary revascularisation and a significantly lower prevalence of cilostazol and severe calcified lesion than the no DAPT group. Warfarin showed a trend towards lower prevalence in the DAPT group than the no DAPT group. Also, there was a significantly higher prevalence of DAPT and previous coronary revascularisation in the no cilostazol group than in the cilostazol group (tables 2 and 3).
Clinical characteristics based on medical therapy at discharge
Lesion characteristics based on medical therapy at discharge
At 12 months of follow-up, prescription of DAPT significantly (p=0.0001) decreased to 51.2%, whereas prescription of cilostazol remained significantly unchanged (p=0.592) at 28.0%. Warfarin also remained significantly unchanged (p=0.70) at 13.3%. The DAPT group still had a significantly higher prevalence of previous coronary and lower prevalence of cilostazol and severe calcified lesion than the no DAPT group (online supplementary table 1). Except for DAPT, there was no significant difference in clinical and lesion characteristics between the cilostazol and the no cilostazol groups (online supplementary table 2).
Supplemental material
Supplemental material
Clinical outcomes
At 12 months, the stent thrombosis rate on limb basis was 1.2% (3/258), and the stent fracture rate on lesion basis was 1.1% (3/277). Major bleeding (intracranial haemorrhage) was observed in 0.4% (1/248). Significant improvement in Rutherford classification (p<0.0001) was observed (table 4). Clinical improvement of at least 1 Rutherford classification was achieved in 85.4%, and no significant difference was observed between treatment groups at discharge (DAPT+: 85.5% vs DAPT− 85.2%; p=0.965, cilostazol+: 84.8% vs 84.4%; p=0.947). Also, ankle-brachial index (ABI) significantly (p<0.0001) improved at 12 months from 0.63±0.19 to 0.84±0.18. All treatment groups at discharge showed a significant (p<0.001) improvement of ABI (DAPT+: 0.63±0.19 to 0.85±0.18, DAPT−: 0.62±0.20 to 0.83±0.16, cilostazol+: 0.60±0.20 to 0.82±0.17, cilostazol−: 0.64±0.19 to 0.85±0.18), and no significant difference in change of ABI was observed between treatment groups at discharge (DAPT+ vs DAPT−; p=0.848, cilostazol+ vs cilostazol−; p=0.685). No major amputation was observed, while minor amputation was executed in two limbs of one patient receiving warfarin in no DAPT and no cilostazol groups at discharge. Therefore, minor amputation rate was 0.4% (1/248) on patient basis and 0.8% (2/258) on limb basis.
Clinical symptoms before and after revascularisation
TLR at 12 months
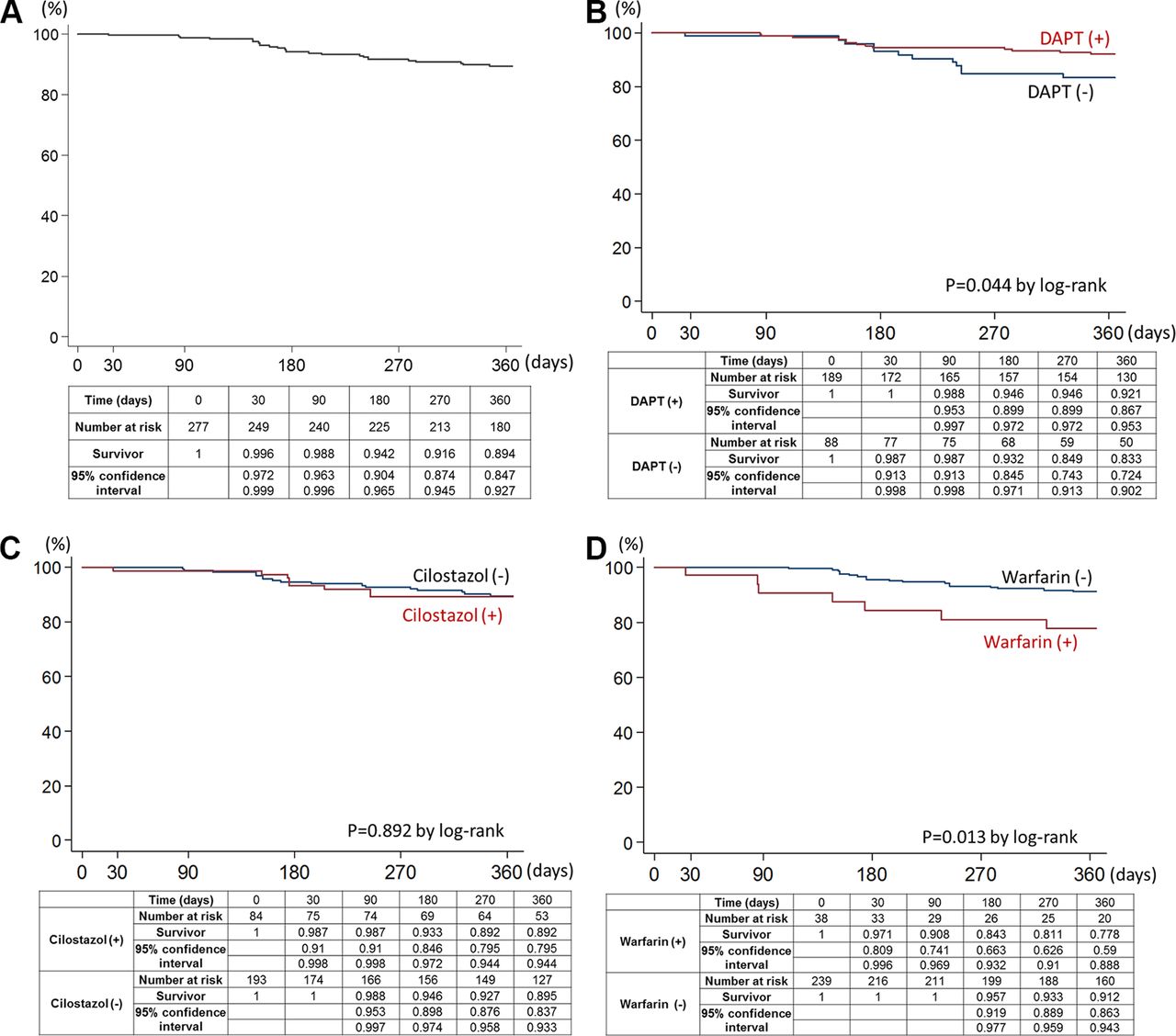
Kaplan-Meier estimates showed that freedom from TLR was 89.4% (95% CI 84.7 to 92.7) at 12 months (figure 1A) and significantly (p=0.044) higher freedom from TLR in DAPT group at discharge than no-DAPT group at discharge (figure 1B). However, there was no significant (p=0.892) difference in freedom from TLR between the cilostazol and no cilostazol groups at discharge (figure 1C). The multivariate Cox proportional hazards model identified warfarin at discharge as the only independent predictor of TLR (table 5). According to Kaplan-Meier estimates, freedom from TLR was significantly (p=0.013) lower in warfarin group at discharge than no warfarin group at discharge (figure 1D). Freedom from TLR at 12 months by the Kaplan-Meier estimates was 77.8% (95% CI 59.0% to 88.8%) in patients with warfarin at discharge and 91.2% (95% CI 86.3% to 94.3%) in those without warfarin at discharge.
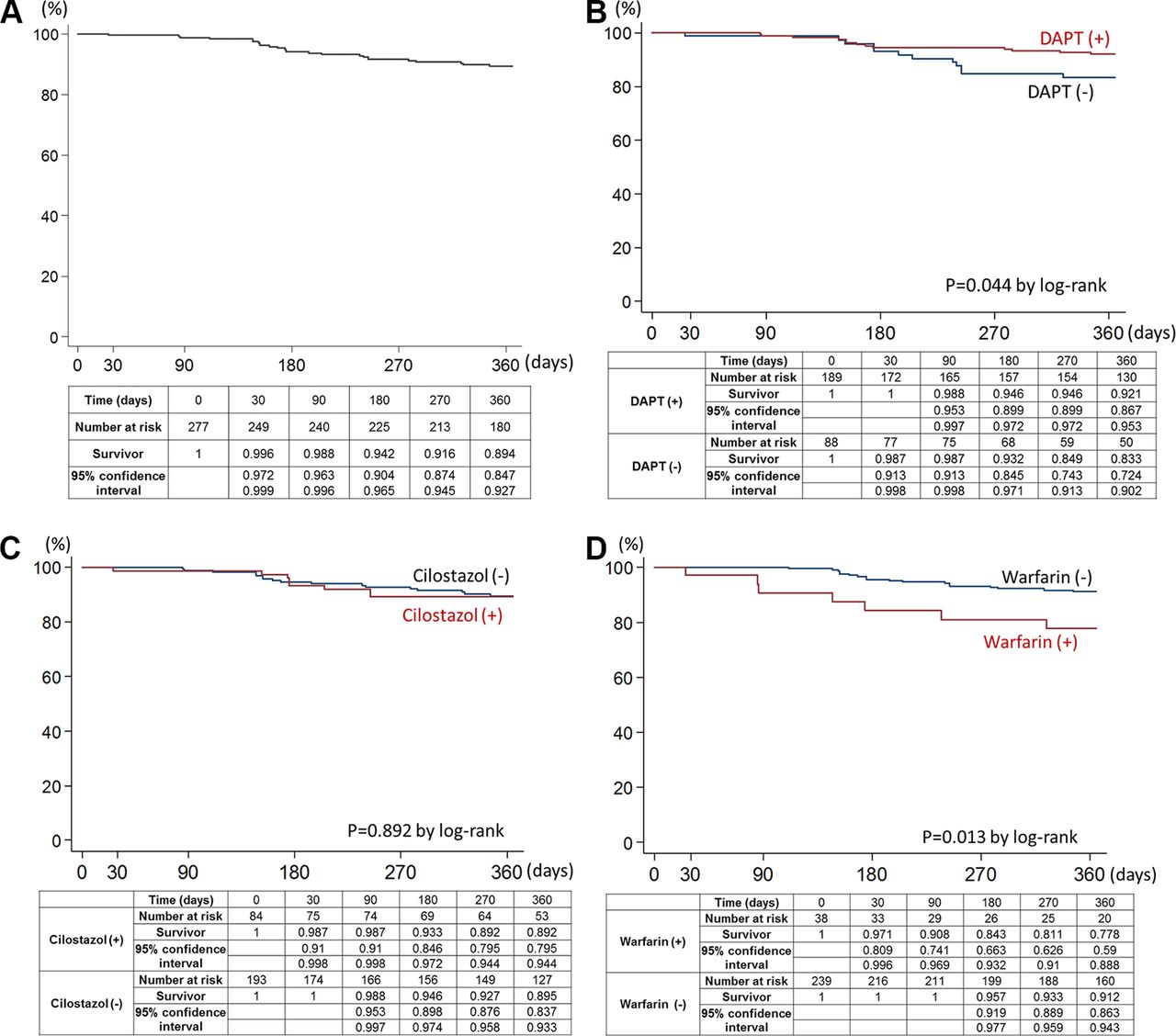
(A) Kaplan-Meier curve at 12 months of follow-up for freedom from target lesion revascularisation. (B) Kaplan-Meier curves at 12 months of follow-up for freedom from target lesion revascularisation by DAPT status at discharge. (C) Kaplan-Meier curves at 12 months of follow-up for freedom from target lesion revascularisation by cilostazol status at discharge. (D) Kaplan-Meier curves at 12 months of follow-up for freedom from target lesion revascularisation by warfarin status at discharge. DAPT, dual antiplatelet therapy.
Cox proportional hazards model for TLR at 12 months
MACCEs at 12 months
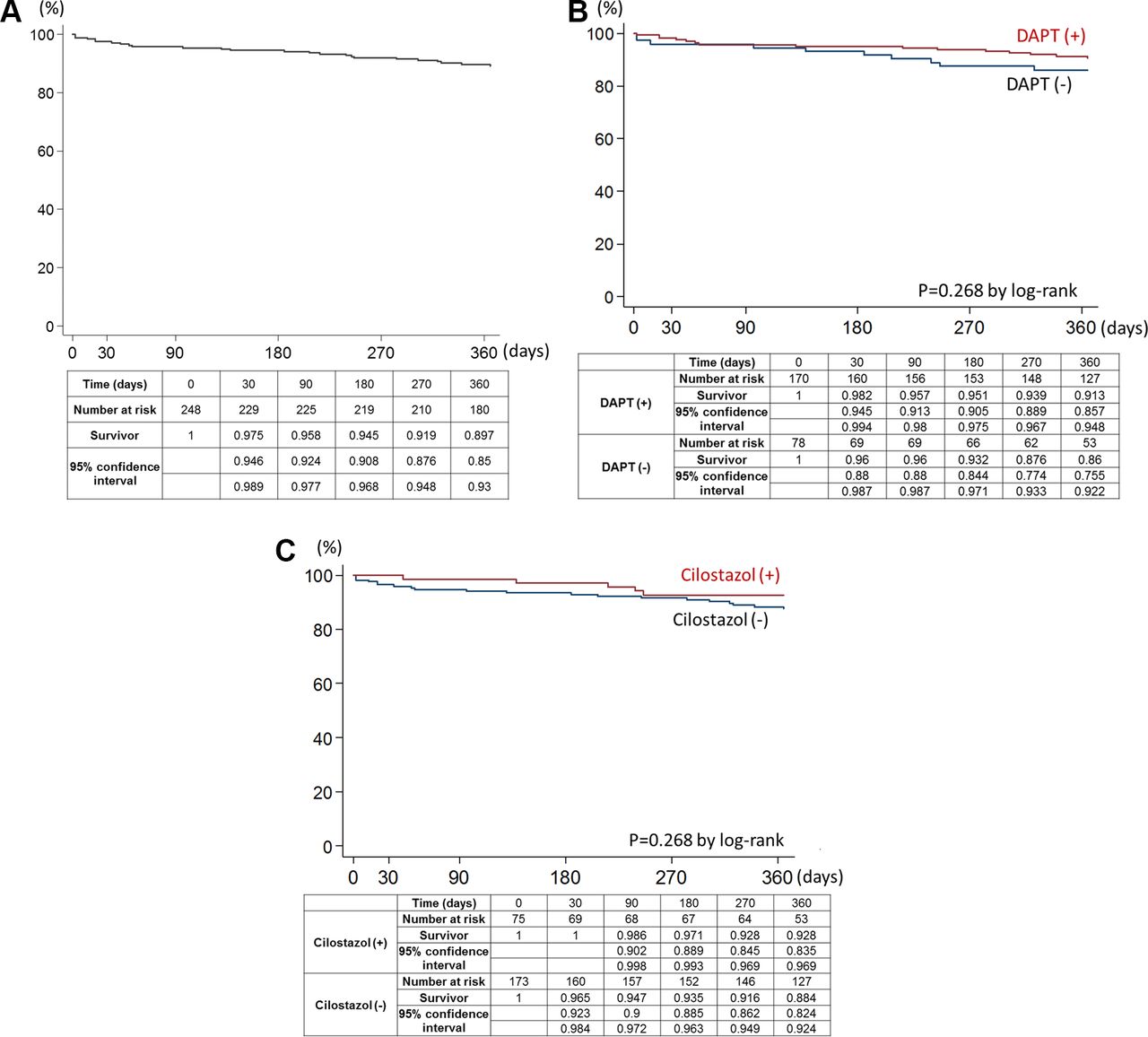
Kaplan-Meier estimates showed that freedom from MACCE was 89.7% (95% CIs 85 to 93) at 12 months (figure 2A) and found no significant difference in freedom from MACCE between the DAPT and no DAPT groups at discharge (p=0.268) and the cilostazol and no cilostazol groups at discharge (p=0.268), respectively (figure 2B and C). The multivariate Cox proportional hazards model found no independent predictor of MACCE (table 6).

{kind=link}
{kind=link}
(A) Kaplan-Meier curve at 12 months of follow-up for freedom from major adverse cardiovascular and cerebrovascular events. (B) Kaplan-Meier curves at 12 months of follow-up for freedom from major adverse cardiovascular and cerebrovascular events by DAPT status at discharge. (C) Kaplan-Meier curves at 12 months of follow-up for freedom from major adverse cardiovascular and cerebrovascular events by cilostazol status at discharge. DAPT, dual antiplatelet therapy.
Cox proportional hazards model for MACCE at 12 months
Discussion
The main findings of this study were as follows: (1) the 12-month Kaplan-Meier estimates of freedom from TLR and MACCE were 89.4% and 89.7%, respectively; (2) in the multivariate Cox proportional hazards model, neither DAPT nor cilostazol at discharge was associated with both TLR and MACCE at 12 months, and warfarin at discharge was only independently associated with TLR at 12 months; and (3) the 12-month Kaplan-Meier estimates demonstrated a significantly lower freedom from TLR in warfarin at discharge than no warfarin at discharge.
With a robust popularity of endovascular intervention for symptomatic PAD, the number of femoropopliteal artery stenting procedures is increasing.10 Given the lack of homogeneity in definitions of in-stent restenosis across clinical studies of femoropopliteal stenting,11 TLR is a more practical metric than restenosis; it reflects the correlation between endovascular therapy and clinical outcomes.12 13 Previous clinical trials with current bare metal nitinol stents have reported that the TLR rate at 12 months ranges from 10.1% to 20.9% (mean lesion length: 6.4–11.2 cm, CTO in 17%–64% of lesions).14–23 In these clinical trials, there is a broad range of minimum duration of antiplatelet therapy (1–3 months for clopidogrel or ticlopidine, indefinite to lifelong for aspirin). Even in the recent postmarketing survey with drug-eluting stent of Zilver PTX (Cook Medical Technologies LLC), which continued clopidogrel or ticlopidine for at least 60-day postprocedure and aspirin indefinitely, freedom from TLR at 12 months was 91%.24 In the present study in which patient characteristics (diabetes in 62% and haemodialysis in 29%) and lesion characteristics (mean lesion length of 12.5 cm, CTO in 41.9% and severe calcification in 16.2%) could reflect the real world, freedom from TLR at 12 months was 89.4% with a significant improvement of ABI and Rutherford category. Also, the present study found no safety concerns. Although caution needs to be taken comparing outcomes between different studies, this second-generation nitinol bare metal stent appears to be acceptable in terms of safety and effectiveness. The administration of DAPT was in 68.5% at discharge and significantly decreased to 51.2% at 12 months but still remained high. Given that prior coronary revascularisation was observed in 55% and 61% at discharge and at 12 months in the DAPT group, the drive of DAPT administration might be extrapolated from clinical experience in coronary intervention. Also, reflecting no consensus on the role of cilostazol in the setting of postintervention, administration of cilostazol remained at approximately 30% (30.2% at discharge and 28.0% at 12 months) in the present study.
According to the MIRROR (Management of Peripheral Arterial Interventions with Mono or Dual Antiplatelet Therapy) study,5 6 which was a prospective randomised study to investigate the effect of aspirin and clopidogrel following femoropopliteal angioplasty or stenting, TLR at 6 months was significantly less common in the DAPT group than in the aspirin monotherapy group (5% in the clopidogrel group vs 20% in the placebo group, p=0.04). When clopidogrel and placebo were stopped after 6 months, patients of both groups remained on aspirin only. There was no longer a significant difference in TLR rates at 12 months (25% in the clopidogrel group and 32% in the placebo group). However, it remains unclear whether the disappearance of a difference is due to the discontinuation of clopidogrel or not. Also, a few prospective studies reported that cilostazol reduced restenosis, repeat revascularisation and cardiovascular events following femoropopliteal balloon angioplasty or stenting.7 8 However, there are some criticisms that these studies have been small and had an open-label design; thus, they were only hypothesis generating.25
In the present study, there was no significant difference in improvement of Rutherford category and improvement of ABI between patients with and without DAPT at discharge or patients with and without cilostazol at discharge. Kaplan-Meier estimates showed a significantly higher freedom from TLR within 12 months in DAPT group at discharge than no DAPT group at discharge, while no significant difference in TLR was observed between cilostazol group and no cilostazol group. However, of great interest, multivariate Cox proportional hazard model found that not DAPT or cilostazol but warfarin at discharge was independently associated with TLR. Prevalence of warfarin remained unchanged between at discharge and at 12 months (14.5% and 13.3%, p=0.70), and Kaplan-Meier estimates demonstrated significantly lower freedom from TLR in warfarin at discharge than no warfarin at discharge. In the literature, there have been limited data regarding the role of warfarin, with and without antiplatelet therapy, in patients with PAD especially undergoing revascularisation. In the Dutch Bypass, Oral anticoagulants or Aspirin study, a multicentre, open, randomised trial, to compare the effectiveness of oral anticoagulants (phenprocoumon or acenocoumarol) such vitamin K antagonist with that of aspirin in the prevention of infrainguinal bypass graft occlusion and other clinical events,26 oral anticoagulants such as vitamin K antagonist yielded significantly higher prosthetic graft occlusion compared with aspirin. The risk of bleeding was almost doubled in the oral anticoagulation group, which may affect the original anti-thrombotic regimens. Furthermore, recent studies reported that warfarin was significantly associated with lower extremity arterial calcification.27 28 Therefore, this adverse effect of warfarin on the peripheral artery might one of the reasons for an increasing need for TLR after femoropopliteal revascularisation. Given the recently reported benefits of direct oral anticoagulants in symptomatic patients with PAD from multicentre double-blind randomised study,29 the clinical effects of warfarin on the peripheral artery might be distinct from those of direct oral anticoagulants.
Antiplatelet therapy is an integral part of preventing cardiovascular morbidity and mortality. According to updated guidelines,1 30 prescribing aspirin or clopidogrel in patients with symptomatic PAD has a class 1 recommendation with evidence level A. Furthermore, DAPT (ie, the combination of aspirin and clopidogrel) has a class IIb recommendation with evidence level B. In the present study, 68.5% received DAPT at discharge and 51.2% even at 12 months in parallel with previous coronary revascularisation. However, we found no association between DAPT at discharge and MACCE. Also, we found no other factors associated with MACCE. Therefore, the present study suggests that antiplatelet monotherapy might be reasonable even after femoropopliteal revascularisation in terms of prevention of cardiovascular mortality and morbidity, supporting the updated guidelines.1 30
The present study has several potential limitations. First, our data are non-randomised and observational in nature and may therefore be affected by confounding. Given the patients’ clinical background, administration of antithrombotic agents was determined by the attending physicians probably considering the risk and benefits trade-off in the real-world practice. Second, administration of antithrombotic agents was assessed at two time points such as at discharge and at 12 months, and no data are available regarding interruption and resumption of antithrombotic therapy within 12 months. However, administration of DAPT at 12 months still remained high at over 50%, and approximately 30% (30.2% at discharge and 28.0% at 12 months) received cilostazol and approximately 15% (14.5% at discharge and 13.3% at 12 months) received warfarin during the study period. Therefore, the effects of ‘on’ and ‘off’ medication fluctuation could be considered small. Finally, the dose of aspirin and cilostazol and the intensity of warfarin might affect the clinical outcomes. Also, although it is speculated that most of patients with warfarin had standard indications such as atrial fibrillation, valve replacement and deep vein thrombosis for anticoagulation, the reason for warfarin administration is not reported in this postmarketing surveillance.
Conclusion
In the real world practice, clinical benefits of DAPT or cilostazol might be small in terms of TLR and MACCE at 12 months. Anticoagulation with warfarin at discharge might increase TLR at 12 months.
Acknowledgments
We would like to thank the investigators and institutions that participated in the Misago stent Japan postmarketing surveillance.
References
Footnotes
Contributors The contribution of each author is as follow: (1) conception and design or analysis and interpretation of data, or both: OK, MN and KN; (2) drafting of the manuscript or revising it critically for important intellectual content: OK, NO, MN and SY and (3) data collection: OK, HM, YI, DK, TN and YY.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests OK reports honorarium of lectures and advisory board fees from Boston Scientific Corporation, honorarium of lectures and research grants from Terumo, and a consultancy fee from Medtronic. MN and KN report consigned research funds from Terumo. TN reports honorarium of lectures from Abbott Vascular, Boston Scientific and Medtronic and consulting fee from Boston Scientific and Century Medical Inc.
Patient consent Not required.
Ethics approval National Cerebral and Cardiovascular Center.