Article Text

Abstract
Objectives This meta-analysis and systematic review seeks to compare both characteristic parameters and procedural outcomes of atrial fibrillation (AF) catheter ablation in patients under general anaesthesia (GA)/deep sedation and mild/moderate sedation.
Background Catheter ablation has become a widely applied intervention for treating symptomatic AF and arrhythmias that are refractory to medical therapy. It can be conducted through from mild sedation to GA.
Methods PubMed and Embase were searched up to July 2018 for randomised controlled trials, cohort and observational studies that assessed the outcomes of catheter ablation under GA/deep sedation or mild/moderate sedation. Nine studies were included in this meta-analysis after screening with the inclusion and exclusion criteria. Heterogeneity between studies and publication bias was evaluated by I2 index and Egger’s regression, respectively.
Results Our meta-analysis found catheter AF ablation with GA/deep sedation to be associated with reduced risk of recurrence (RR: 0.79, 95% CI 0.56 to 1.13, p=0.20) and complications (RR: 0.95, 95% CI 0.64 to 1.42, p=0.82), though statistically insignificant. In terms of procedural parameters, there was no significant difference between the two groups for both procedural time (SMD: −0.13, 95% CI −0.90 to 0.63, p=0.74) and fluoroscopy time (SMD: −0.41, 95% CI −1.40 to 0.58, p=0.41). Univariate meta-regression did not reveal any covariates as a moderating factor for complication and recurrence risk.
Conclusion Apart from an increased likelihood of procedural success, ablation by GA/deep sedation was found to be non-significantly different from the mild/moderate sedation approach in both procedural parameters and outcome measures.
- general anesthesia
- sedation
- arrhythmia
- atrial fibrillation
Statistics from Altmetric.com
Condensed Abstract
Catheter ablation remains the intervention of choice in patients with treatment-resistant arrhythmias. However, there has been much debate as to whether general anaesthesia/deep sedation or mild/moderate sedation is ideal in arrhythmic ablation procedure. We identified nine suitable studies for the final meta-analysis. When general anaesthesia/deep sedation was compared with mild/moderate sedation, it tended to have a lower risk of recurrence but higher risk of complications. There is also no significant difference in both procedural duration and fluoroscopy time between the two approaches. Furthermore, our univariate analysis demonstrated found no confounding factors influencing the outcome measures.
Key messages box
What is already known about this subject?
Both the use of general anaesthesia (GA)/deep sedation and conscious sedation are viable means of conducting catheter ablation. However, ablation procedures tend to last for several hours, which can cause discomfort while requiring patients to keep still, hence favouring the use of GA or deep sedation. With the emergence of cryoballoon ablation, the use of mild to moderate sedation becomes a viable option, avoiding risks associated with GA induction and maintenance.
What does this study add?
In light of this evidence, it is clear that there are advantages in both approaches. It is therefore important to know that the availability of an alternative AF ablation approach does not compromise vital procedural outcomes such as acute success, periprocedural complications and recurrence rates. As such, this meta-analysis aims to compare procedural characteristics and outcomes between the two approaches
How might this impact on clinical practice?
Mild to moderate sedation can be an alternative to general anaesthesia for performing cryoballoon ablation.
Introduction
Atrial fibrillation (AF), the most common arrhythmia encountered in clinical practice, affects around 1% of the general population1 and is associated with a number of life-threatening diseases including stroke, systemic embolism and heart failure.2–5 Pharmacological therapy such as antiarrhythmic drugs and anticoagulants has been used to maintain sinus rhythm and prevent stroke, respectively. However, these therapies demonstrate low successful rates for reducing AF recurrence and are associated with adverse effects such as bleeding.6 Over the past two decades, techniques of AF ablation have been refined with high efficacies,2 7–9 with many studies reporting its advantage over antiarrhythmic drugs.2 10 Thus, catheter ablation has become a widely adopted option for treating symptomatic AF.
Since the intervention can be complex and lengthy, and patient can experience discomfort during the procedure, sedative agents are commonly applied to avoid body movement, maintain stability of catheters and reduce pain. Apart from their sedative effects, several anaesthetic agents have direct electrophysiological effect on cardiovascular system and therefore can be administered to avoid arrhythmogenesis.11–15 Currently, ablation can be performed under either general anaesthesia (GA), deep sedation or mild to moderate sedation based on patient’s condition, anaesthesiologist preference and institutional protocols.16–18 Several studies have compared the efficacy of catheter ablation under GA and non-GA conditions, yet the definite impact of those anaesthetic methods on ablation outcomes remains unclear. Therefore, we conducted a systematic review and meta-analysis to examine outcomes of catheter ablation under GA/deep sedation and mild/moderate sedation techniques.
Methods
Search strategy, inclusion and exclusion criteria
The meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. PubMed and Embase were searched for studies that investigated the outcomes of AF catheter ablation under GA/deep sedation or mild/moderate sedation. The following terms were used: (((arrhythmia) OR (atrial fibrillation)) AND ((anesthesia) or (anaesthesia) OR (sedation)) AND ((ablation) OR (radio frequency) OR (pulmonary vein isolation))). The search period was from the beginning of the databases through to 16 July 2018 with no language restrictions. The following inclusion criteria were applied: (1) the design was a case–control, prospective or retrospective cohort study in humans, (2) related to GA or non-GA and (3) contained clear outcomes, including recurrence rate, hospital readmission, mortality and so on. Included studies also adhered to the follow-up recommendations postablation from the 2016 European Society of Cardiology (ESC) guidelines for the management of AF developed in collaboration with European Association for Cardiothoracic surgery (EACTS). These suggest ‘patients should be seen at least once by a rhythm specialist in the first 12 months’.
The quality assessment of these studies included in our meta-analysis was performed using the Newcastle-Ottawa Quality Assessment Scale (NOS). The point score system evaluated the categories of study participant selection, comparability of the results and quality of the outcomes. The following characteristics were assessed: (A) representativeness of the exposed cohort; (B) selection of the non-exposed cohort; (C) ascertainment of exposure; (D) demonstration that outcome of interest was not present at the start of study; (E) comparability of cohorts on the basis of the design or analysis; (F) assessment of outcomes; (G) follow-up period sufficiently long for outcomes to occur; and (H) adequacy of follow-up of cohorts. This scale varied from zero to nine stars, which indicated that studies were graded as poor quality if they met <5 criteria, fair if they met 5 to 7 criteria and good if they met >8 criteria. The details of the NOS quality assessment are shown in online supplementary table 1.
Supplemental material
Data extraction and statistical analysis
Data from different studies were entered in prespecified spreadsheets in Microsoft Excel. All potentially relevant studies were retrieved as complete manuscripts, which were assessed fully to determine their compliance with the inclusion criteria. We extracted the following data from the included studies: (1) publication details: last name of first author, publication year and locations; (2) study design; (3 outcomes(s); and (4) characteristics of the population including sample size, gender, age and number of subjects. Two reviewers (GW and KHCL) reviewed each included study independently. Disagreements were resolved by adjudication with input from a third reviewer (GT).
Heterogeneity across studies was determined using Cochran’s Q-value and the I2 statistic from the standard χ2 test. Cochran’s Q-value is the weighted sum of squared differences between individual study effects and the pooled effect across studies. The I2 statistic from the standard χ2 test describes the percentage of variability in the effect estimates resulting from heterogeneity. I2 >50% was considered to reflect significant statistical heterogeneity. The random-effects model using the inverse variance heterogeneity method was used with I2 >50%. To locate the origin of the heterogeneity, sensitivity analysis excluding one study at a time was also performed. Funnel plots showing standard errors or precision against the logarithms of the OR were constructed. The Begg and Mazumdar rank correlation test and Egger’s test were used to assess for possible publication bias (figure 3). Possible associations between population covariables and study outcomes were explored using multivariate meta-regression. To account for missing data, we used mean imputation (<10% missing) or random imputation (>10% missing). All statistical analysis was conducted using Review Manager 5.3 for MacOS and Comprehensive Meta-Analysis version 3.0 (Biostat, Inc, Englewood, New Jersey, USA). Statistical significance was set as p value of less than 0.05.
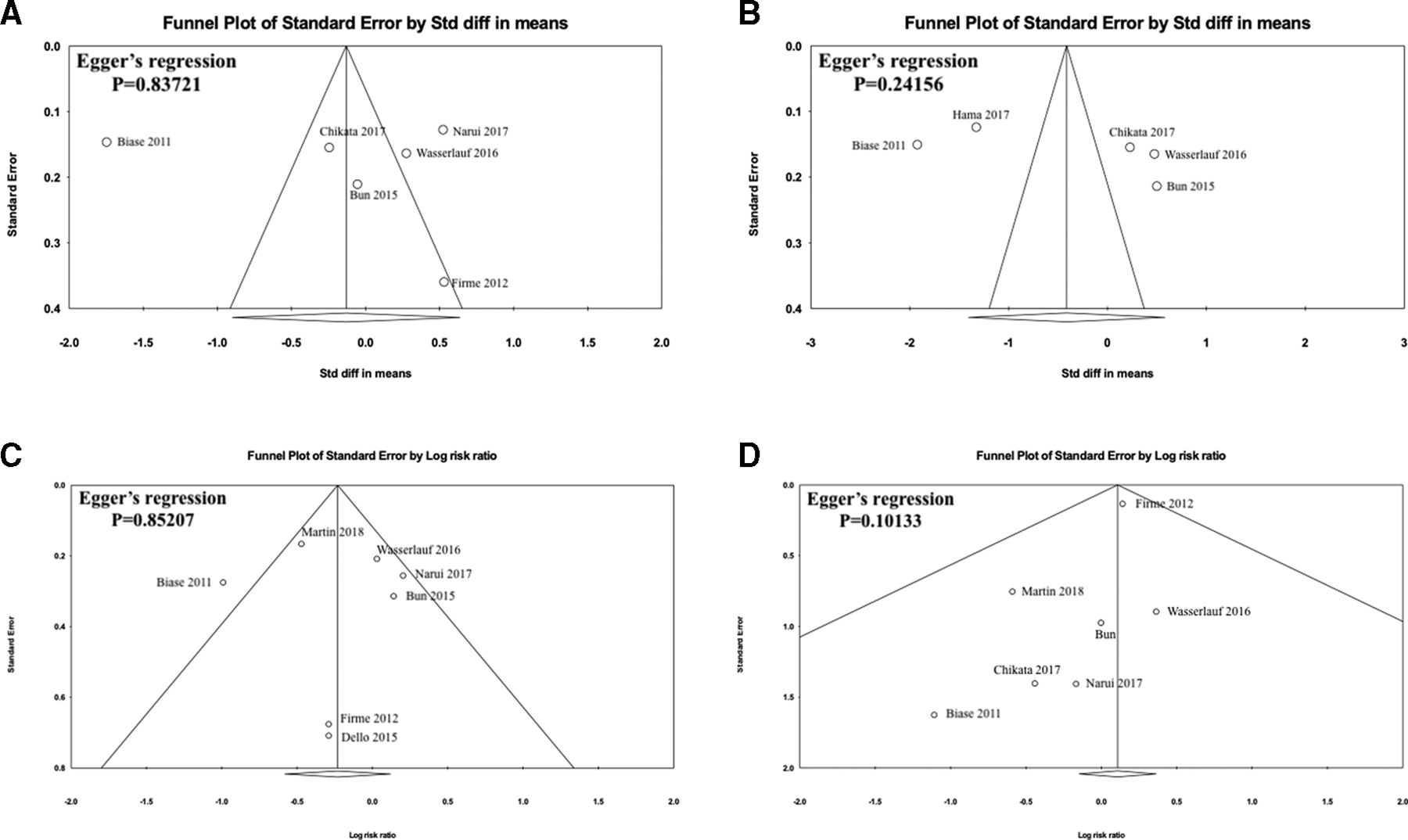
Trim-and-fill funnel plots with Egger’s regression test of (A) mean procedural time, (B) mean fluoroscopy time, (C) recurrence, (D) complications comparing between GA/deep sedation and mild/moderate sedation in patients undergoing AF ablation. AF, atrial fibrillation; GA, general anaesthesia.
Results
Patient baseline characteristics
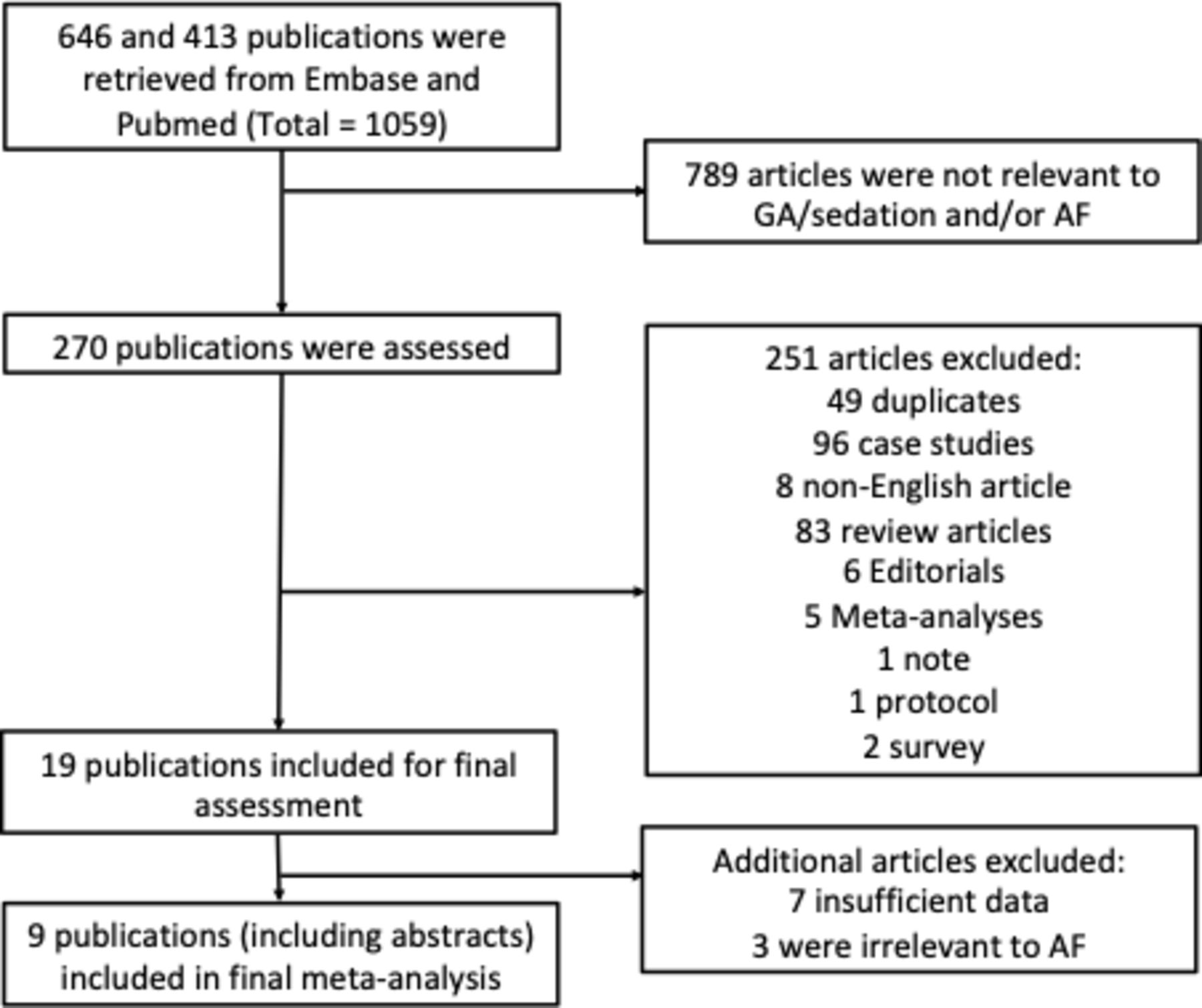
A flow diagram detailing the search and study selection process is illustrated in figure 1. In the end, a total of nine cohort studies involving 1715 patients between 2006 and 2018 met our selection criteria for inclusion.3 19–26 The mean age of the population is 59.9±10.0, consisting of mainly male patients (78.0%). The baseline characteristics of the included cohort and follow-up duration based on individual studies are summarised in table 1. Only the baseline characteristics of seven (out of nine) studies were included in table 1. This is due to the lack of sufficient characteristics data provided by the remaining two studies.24 25 Regardless, sufficient outcome and procedural data were provided by all nine studies for effective pooling of outcome measures. Outcome and procedural measures pooled in this meta-analysis include: (1) mean procedural time, (2) mean fluoroscopy time, (3) procedural success rate, (4) recurrence rate and (5) complication rate. Only seven of the nine studies reported specific anaesthetic protocols,3 19–23 26 which mainly involve initiation with an induction agent (eg, propofol) and an opioid (fentanyl or remifentanil) with or without a neuromuscular blocker, followed by endotracheal or supraglottic airway device maintenance.
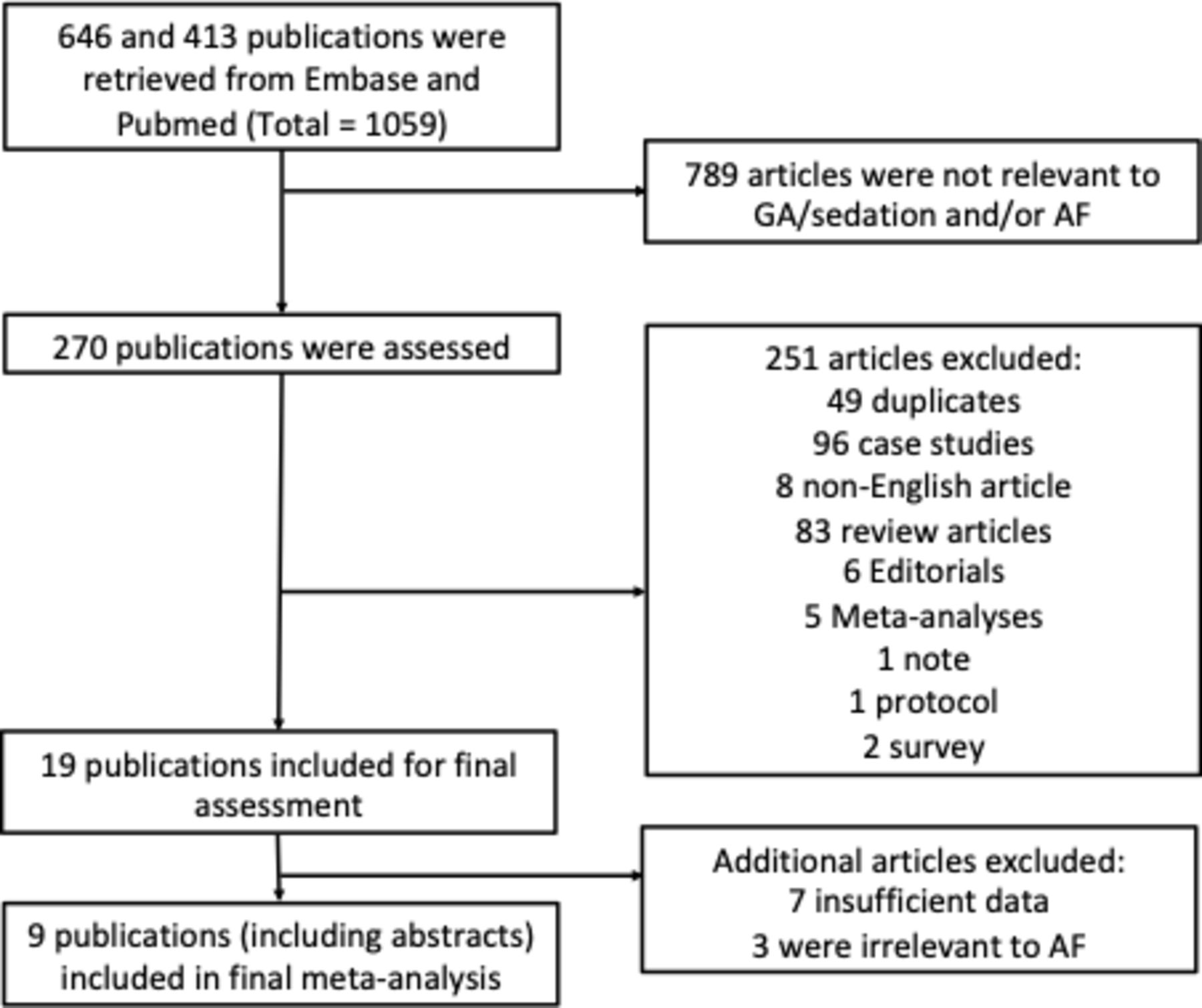
PRISMA flow diagram for the study selection process. AF, atrial fibrillation; GA, general anaesthesia; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Baseline characteristic of patients from the included studies
GA/deep sedation versus mild/moderate sedation in patients undergoing catheter ablation: mean procedural and fluoroscopy time
Eight of nine studies reported mean procedural time in catheter ablation patients using either GA/deep sedation or mild/moderate sedation.3 19–23 25 26 Of these, standard mean differences could not be calculated for two studies21 25 as the SD was not reported. Pooled analysis of AF ablation and GA/deep sedation ablation were found to be associated with a shorter procedural time (SMD: −0.13, 95% CI −0.90 to 0.63, p=0.74; figure 2A). Similarly for mean fluoroscopy time in AF ablation, it was also found to be shorter with GA/deep sedation (SMD: −0.41, 95% CI −1.40 to 0.58, p=0.41; figure 2B).

Forest plots comparing (A) mean procedural time of arrhythmic ablation and (B) mean fluoroscopy time between the GA/deep sedation and mild/moderate sedation group. GA, general anaesthesia.
A high degree of heterogeneity was observed across the studies (I2: 97% and 98%, respectively). In order to locate the origin of the heterogeneity, sensitivity analysis excluding one study at a time was performed. Doing so did not significantly alter the overall heterogeneity. Regardless, results of the Egger’s test showed no evidence of publication bias (Egger’s regression test p=0.67485 and 0.17132 respectively; figure 3A and B).
GA/deep sedation versus mild/moderate sedation in patients undergoing catheter ablation: procedural success rate
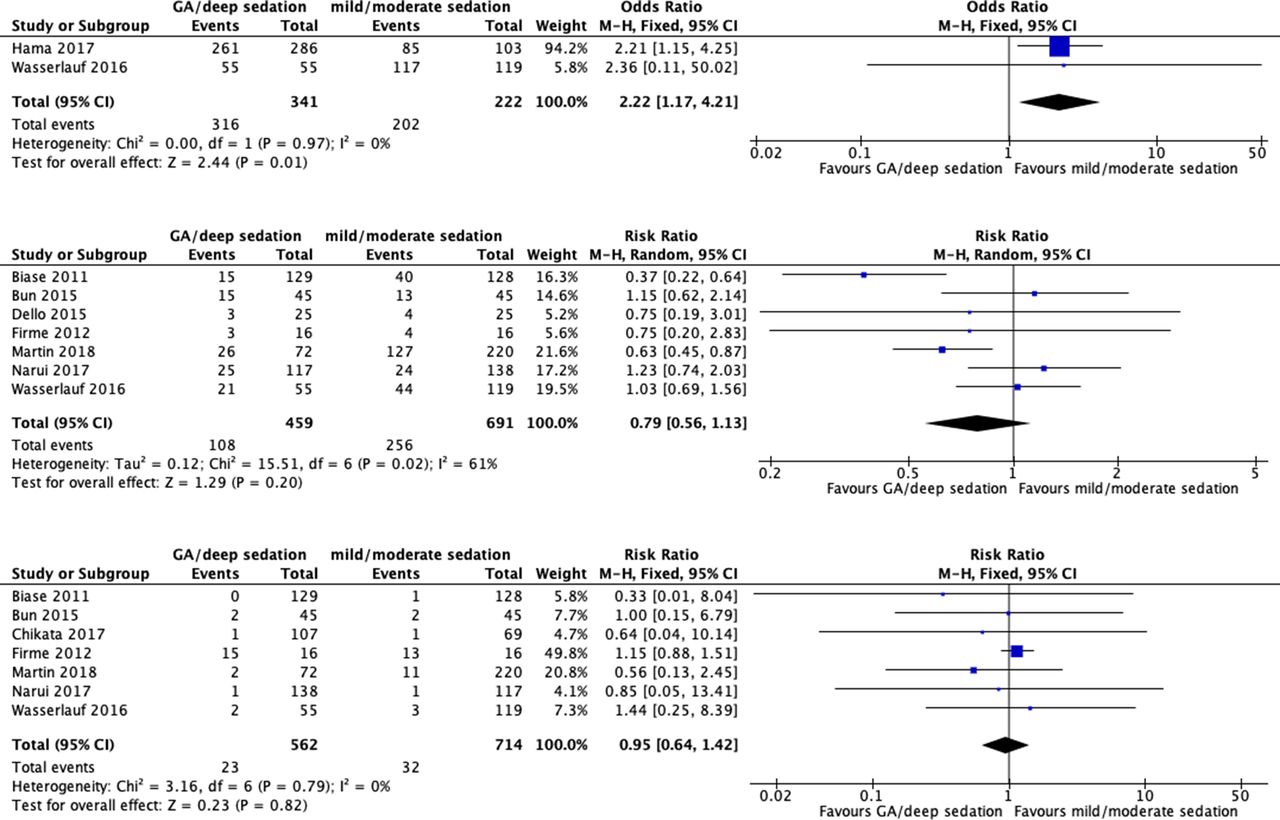
Only two studies reported procedural success rates in AF catheter ablation patients with.23 24 The majority of the remaining studies only used patients who have undergone successful catheter ablation for determining recurrence and complication outcomes. Procedural success was more significant with AF ablation between GA/deep sedation and mild/moderate sedation (OR=2.22, 95% CI 1.17 to 4.21, p=0.01; figure 4A). I2 was 0%, indicating a lack of heterogeneity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Forest plots comparing procedural success rates of AF ablation between the GA/deep sedation and mild/moderate sedation group. (B) Forest plots comparing recurrence rates post-AF ablation between the GA/sedation and mild/moderate sedation group. (C) Forest plots comparing complication rates post-AF ablation between the GA/sedation and mild/moderate sedation group. AF, atrial fibrillation; GA, general anaesthesia.
GA/deep sedation versus mild/moderate sedation in patients undergoing catheter ablation: recurrence rate
Seven out of nine studies reported recurrence rates after a mean follow-up of 13.9 months3 19–23 25 after AF ablation. Primary analysis of the included AF studies demonstrated that patients who use GA/deep sedation tended to have a lower risk of recurrence on follow-up compared with the mild/moderate sedation group, but this did not reach statistical significance (RR: 0.79, 95% CI 0.56 to 1.13, p=0.20; figure 4B). A moderate degree of heterogeneity (I2=61%) was observed. Sensitivity analysis excluding one study at a time was performed but doing so did not significantly alter the overall heterogeneity. Results of the Egger’s test showed no evidence of publication bias (Egger’s regression test p=0.85207; figure 3C).
GA/deep sedation versus mild/moderate sedation in patients undergoing catheter ablation: complication rate
Lastly, a total of seven out of nine studies reported complication rates postablation in patients using GA/deep sedation and mild/moderate sedation.3 19–23 26 Only two studies favoured the use of mild/moderate sedation, while five studies found GA/deep sedation to be associated with lower complication risks. One study found no difference between the two approaches, yielding a risk ratio of 1.00. Primary analysis did not demonstrate a significant difference between the two groups (RR: 0.95, 95% CI 0.64 to 1.42, p=0.82; figure 4C). I2 was 0%, indicating a lack of heterogeneity. Results of the Egger’s test showed no evidence of publication bias (Egger’s regression test p=0.10133; figure 3D).
Univariate meta-regression analysis of recurrence and complication outcomes
A univariate meta-regression analysis was conducted using all common covariates for recurrence and complication rates. Procedural success was omitted, as there was not a sufficient number of studies for meta-regression. The covariates used were mean age, male gender, hypertension, procedure duration and follow-up duration. Follow-up duration was not included in the regression analysis of complications as it only involves periprocedural and immediate postprocedural complications. Results of the meta-regression are shown in table 2 accordingly. When adjusted for other variables, none of the covariates moderated recurrence and complication outcomes. Slope coefficient did not differ significantly from zero (p>0.05).
Univariate meta-regression analysis for recurrence and complications
Discussion
The main findings of this systematic review and meta-analysis: (1) the use of GA/deep sedation may confer increased chance of procedural success; (2) since there is no significant difference in mean procedural and fluoroscopy time, the GA/deep sedation is equally efficient as the mild/moderate sedation approach; (3) patients who use GA/deep sedation are associated with lower risk of recurrence on follow-up compared with the mild/moderate sedation group though statistically insignificant; ad n(4) GA/deep sedation was also found to be equally safe with mild/moderate sedation in terms of total complication rate.
To the best of our knowledge, this is the first systematic review and meta-analysis comparing GA/deep sedation to mild/moderate anaesthesia in catheter ablation for AF. The outcome measures include mean procedural time, fluoroscopy time, success, recurrence and complication rates. The increased chance of procedural success may to due to more thorough patient immobilisation through GA/deep sedation, which would reduce unwanted movements and enhance procedural accuracy. During our meta-regression analysis, hypertension was also found to be a significant confounding variable to the complication outcome. This is in keeping with a recent study that found hypertension to be associated with increased risk of complication during catheter ablation of AF.27 However, the causal mechanism underlying this association remains unknown. This meta-analysis has not revealed any significant difference in procedural time between GA/deep sedation and mild/moderate anaesthesia. We postulate that the time freed up from improved procedural accuracy of GA/deep sedation compared with mild/moderate anaesthesia may be offset by the additional time needed for deeper sedation of patients.
The effect of anaesthetic agent on recurrence rate
Our study demonstrates that patients who use GA/deep sedation tended to have a lower risk of recurrence on follow-up compared with the mild/moderate sedation group. The result can partially be explained by the antiarrhythmic effect of propofol, an anaesthetic agent that is commonly used to induce deep sedation but can also terminate supraventricular tachycardia and ventricular tachycardia storm.11–13 15 28 In addition, Narui et al22 found that deep sedation induced by propofol is correlated with a lower frequency of dissociated pulmonary vein (PV) activity. Since dissociated PV activity is a risk factor for AF recurrence, propofol can possibly reduce the recurrence rate.28 Another possible explanation of the lower recurrence rate under GA/deep sedation is attributed to a greater immobility and less interruption during the procedure, which in turn allows for better controlled thoracic expansion.19 Nevertheless, since our study demonstrated no significant difference on recurrence rate between two anaesthetic groups, further study is required for elucidating the relationship between recurrence rate after ablation and anaesthetic agents.
Safety and concerns regarding GA/deep sedation and conscious sedation
Although in this study we demonstrate that there is no significant difference between the two groups in terms of the complication rate, there are still some concerns for the safety of both GA/deep sedation and conscious sedation. Since GA can potentially interfere with the normal laryngeal reflexes that function to inhibit swallowing or coughing, the use of GA is associated with higher risk of aspiration and some other common complications such as nausea, vomiting and throat pain.19 Moreover, a higher risk of atrio-oesophageal fistula has been shown to be associated with GA comparing with conscious sedation. This complication can be possibly due to the fact that GA can immobilise and decrease deglutition of oesophagus, which promote the lesion extending to the esophageal wall.29 However, this type of complication is not noted in other studies and can be easily prevented by carefully monitoring the oesophageal temperature and limit the RF delivery to 20 s.19 Most studies show that GA/deep sedation is associated with lower complication risks, with Firme et al3 demonstrating a reduced incidence of cough with GA, and Di Biase et al19 also stated that most GA complications can be rare and easily treated.
Concerns for conscious sedation usually lies in the intensive chest pain that can be caused during the procedure. Martin et al21 recently showed that patients under conscious sedation are more easily agitated or suffer from uncontrolled pain, thereby negatively affecting the procedures. This disadvantage is further supported by Narui et al,22 in which patients with mild sedation endured pain and uncomfortable conditions during procedure. A survey by Münkler et al30 also demonstrated a high patient satisfaction with deep sedation, with 83% of patients considering it to be ‘good’ or ‘very good’.
Limitations
Several limitations should be noted. First, a high heterogeneity was found in the study for the mean procedural and fluoroscopy time, indicating an inconsistency of the data obtained. Moderate heterogeneity was found for recurrence rate, and therefore, these results should be interpreted with caution. Although the there is little heterogeneity for procedural success rate, the sample size can be too small to estimate the accurate heterogeneity. The heterogeneity may be potentially caused by the differences in the baseline population characteristics and ablation techniques, and the accuracy may be improved by including more studies. In addition, the various indicators of success vary in the extent to which they are influenced by the external factors; for instance, procedural success is highly dependent on the operational conditions, while recurrence rate could be affected by a wider range of factors including fibrosis,31 postoperational adherence, lifestyle and socioeconomic circumstances, which may further explain the discrepancy in the results of procedural success and other indicators of success. Another limitation is that most studies only take data from patients who have undergone successful catheter ablation, which may potentially limit the accuracy of analysis. Finally, due to lack of the data, some parameters and subgroup analyses such as mean anaesthesia time, number of ablation application and PVC-specific recurrence cannot be adequately analysed.
Conclusions
For AF catheter ablation, there are no significant differences between GA/deep sedation and mild/moderate sedation in terms of mean procedural and fluoroscopy time, recurrence rate and complication rate. However, GA/deep sedation is associated with a higher procedural success rate, suggesting that GA/deep sedation is a favoured anaesthetic technique in catheter ablation.
Acknowledgments
JH is supported by a postdoctoral research fellowship from the Department of Anesthesia and Intensive Care, The Chinese University of Hong Kong. GT is supported by a clinical assistant professorship from the Croucher Foundation of Hong Kong.
References
Footnotes
Contributors All authors contributed intellectually to this manuscript.
Funding This project was funded by internal research grants from the Chinese University of Hong Kong, Hong Kong, China, and the First Affiliated Hospital of Dalian Medical University, Dalian, China.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.