Article Text

Abstract
Objective High-sensitivity troponin (hs-Tn) assays need to be applied appropriately to improve diagnosis and patient outcomes in acute coronary syndromes (ACS).
Methods Experts from Asia Pacific convened in 2015 to provide data-driven consensus-based, region-specific recommendations and develop an algorithm for the appropriate incorporation of this assay into the ACS assessment and treatment pathway.
Results Nine recommendations were developed by the expert panel: (1) troponin is the preferred cardiac biomarker for diagnostic assessment of ACS and is indicated for patients with symptoms of possible ACS; (2) hs-Tn assays are recommended; (3) serial testing is required for all patients; (4) testing should be performed at presentation and 3 hours later; (5) gender-specific cut-off values should be used for hs-Tn I assays; (6) hs-Tn I level >10 times the upper limit of normal should be considered to ‘rule in’ a diagnosis of ACS; (7) dynamic change >50% in hs-Tn I level from presentation to 3-hour retest identifies patients at high risk for ACS; (8) where only point-of-care testing is available, patients with elevated readings should be considered at high risk, while patients with low/undetectable readings should be retested after 6 hours or sent for laboratory testing and (9) regular education on the appropriate use of troponin tests is essential.
Conclusions We propose an algorithm that will potentially reduce delays in discharge by the accurate ‘rule out’ of non-ACS patients within 3 hours. Appropriate research should be undertaken to ensure the efficacy and safety of the algorithm in clinical practice, with the long-term goal of improvement of care of patients with ACS in Asia Pacific.
- CORONARY ARTERY DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The total burden of ischaemic heart disease in Southeast Asia has increased by approximately 61.5% since 1990.1–3 Consequently, hospital emergency departments (EDs) are seeing increasing number of patients presenting with chest pain and other signs of acute coronary syndromes (ACS). The emergent nature of ACS renders it important to rapidly and accurately diagnose and risk stratify patients. The diagnostic algorithm of non-ST segment elevation ACS involves the use of cardiac biomarkers, such as troponin, alongside patient's history, symptoms, clinical signs, ECG parameters and available imaging (eg, echocardiography) for drawing sound clinical judgements.4 ,5
An Asia Pacific expert meeting was convened in Singapore on 21 November 2015 to discuss regional practice in the current use of high-sensitivity troponin (hs-Tn) assays, specifically, the hs-Tn I assay and to develop an algorithm to appropriately use this assay in assessing and treating ACS. This article describes the consensus in the use of hs-Tn assays and provides recommendations deemed suitable for this region.
Use of troponin assays in Asia Pacific
Currently, there are limited data on the use of different troponin assays throughout Asia Pacific. Discussion at the consensus meeting revealed that most tertiary centres use troponin levels in ACS diagnosis, many of which commonly use hs-Tn assays for either troponin T or I, while some still use contemporary standard assays. In some resource-limited settings, CK-MB levels were still used. In suburban or rural areas of Australia, Thailand and Malaysia, where there is limited access to 24-hour laboratory services, point-of-care (POC) assays were used. Therefore, we have also included a statement regarding POC assays.
Troponin assays
A range of troponin assays are currently available for quantification of troponin T or I, most of which are described as hs assays while some may not fulfil the standard criteria. These criteria include: (1) having a coefficient of variation (CV) of ≤10% at the 99th percentile of the reference population and (2) being able to measure concentrations below the 99th percentile and above the assay's limit of detection in at least 50% (and ideally >95%) of healthy individuals.6
The 99th percentile is the concentration below which troponin levels lie for 99% of the healthy population (the upper reference limit). The 10% CV is the troponin concentration at which the analytic concentration of troponin is 10% and generally lies at the lower end of the acute myocardial infarction (MI) curve (figure 1).7 The ratio of the 10% CV to the 99th percentile provides an estimate of precision—the smaller the ratio, the higher the precision.7 The 99th percentile and 10% CV differ between assays (table 1).
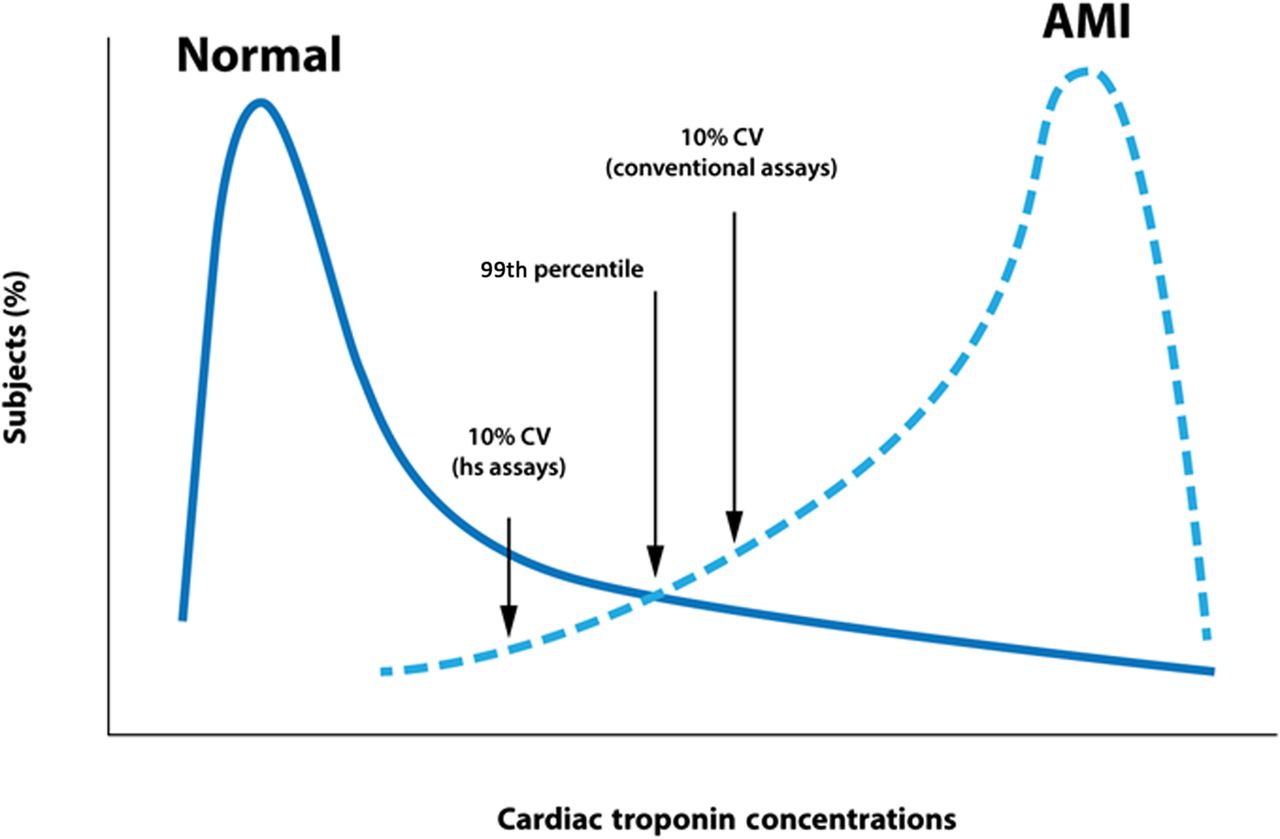
Distribution of high-sensitivity (hs) troponin levels in a healthy population and patients with acute myocardial infarction (AMI), with an indication of the concentration defined by the 99th percentile and the upper 10% coefficient of variation (CV) of the 99th percentile.
As shown in figure 1, the distribution of hs-Tn levels is non-Gaussian and positively skewed.9–11 Moreover, the distribution of cardiac troponin levels is affected by gender and renal function, and potentially by age and ethnicity, leading to different 99th percentile and 10% CV in different populations.8 ,12–17
Gender differences may be particularly important clinically. Studies comparing cardiac troponin I levels measured by Abbott's high-sensitivity ARCHITECT STAT assay showed that the 99th percentile is consistently lower in women than men (table 2).8 ,9 ,15–19 Thus, if the 99th percentile for the overall population is used, a number of women with ACS may not be identified. In contrast, using gender-specific thresholds may double the number of women who are correctly diagnosed with MI, without affecting the number of diagnosed men.20
Comparison of 99th percentile values in men, women and mixed gender populations (general, non-cardiac or healthy individuals) in different studies using the Abbott ARCHITECT STAT high-sensitivity troponin I package
Methods
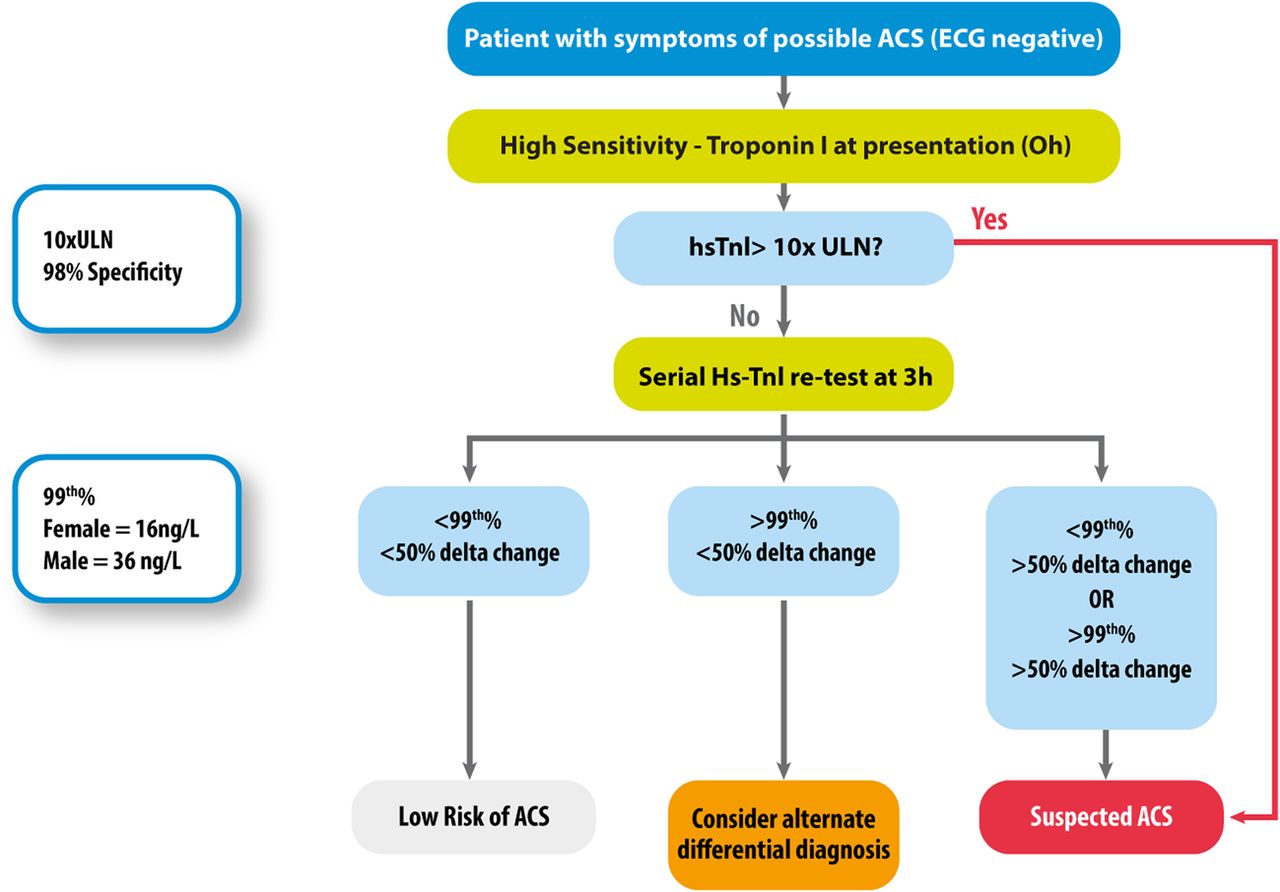
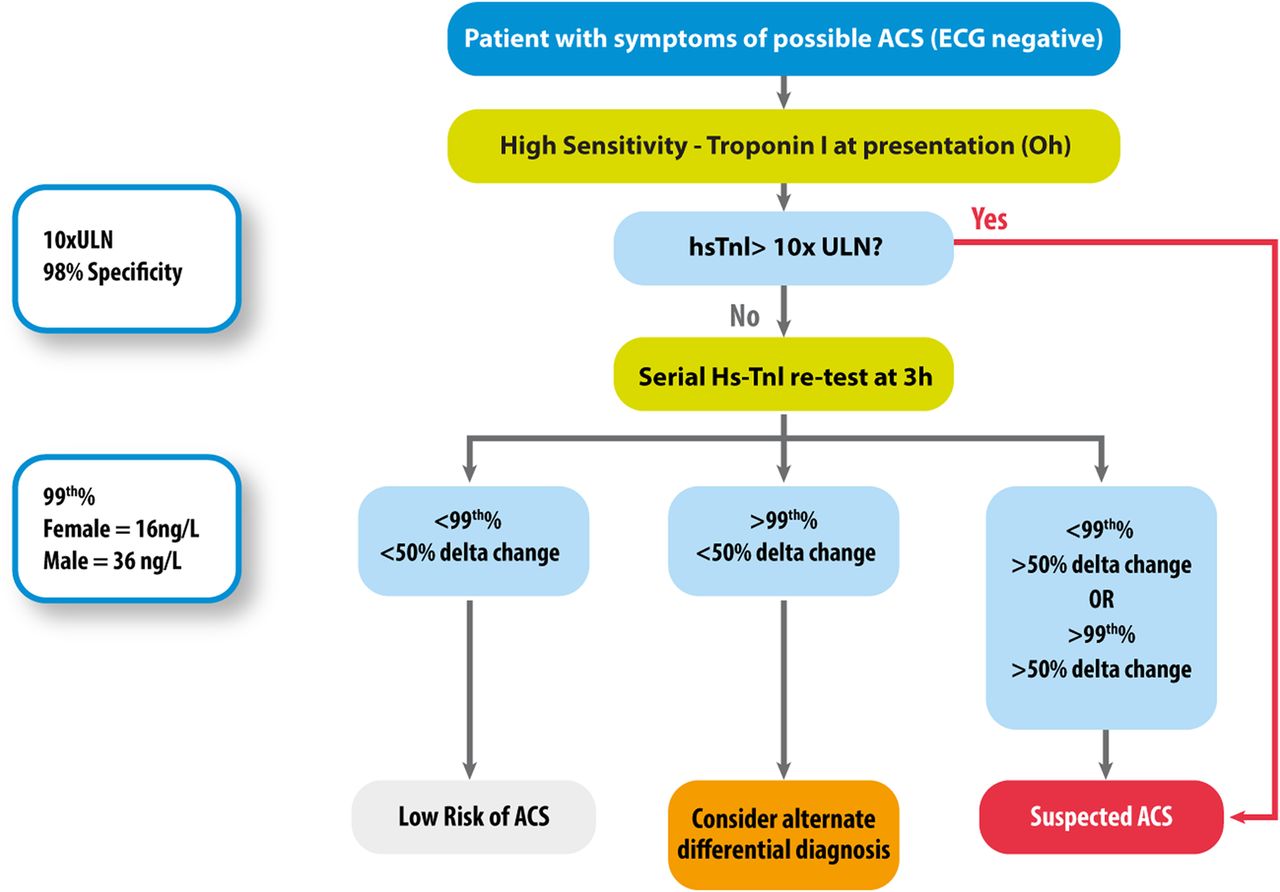
The expert panel was selected from a pool of practicing cardiologists, emergency physicians and chemical pathologists from Asia Pacific countries (Singapore, Malaysia, Philippines, Vietnam, Indonesia, Thailand, Hong Kong and Australia). The main criterion for selection was experience in the clinical or research use of troponin assays. The panel discussed the current literature on hs-Tn testing and developed an algorithm (figure 2) and consensus recommendations for the appropriate use of these tests in Asia Pacific based on their understanding of the literature and individual clinical experience. The wording of each key consensus statement and algorithm was determined through discussion until unanimously agreed. Subsequently, the supporting evidence for the algorithm and for each statement was searched via PubMed, and the wording developed. This was circulated to the entire group, incorporating all feedback and recirculated for unanimous agreement.
{kind=link}
{kind=link}
Consensus-based algorithm for the recommended use and interpretation of high-sensitivity troponin I (hs-Tn I) levels in Asia Pacific. ACS, acute coronary syndromes; ULN, upper limit of normal.
Results
Consensus statements
Troponin is the preferred cardiac biomarker for diagnosing ACS and is indicated for patients with possible ACS
Supporting evidence
Current international guidelines advocate the use of troponin, preferably high-sensitivity assays, during the diagnostic workup of suspected patients with ACS and without ST-segment elevation,4 ,21–24 and troponin is the preferred biomarker in the European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation Task Force for the Universal Definition of Myocardial Infarction.25 Troponin is more sensitive and specific to myocardial injury than creatine kinase (CK), CK-muscle and brain (MB) or myoglobin.24–27 CK-MB should only be used at Asia Pacific centres where troponin testing is unavailable.
The hs-Tn assays should be used in clinical care, with ng/L as the standard unit of measurement
Supporting evidence
The recommended unit of measurement for troponin I or T level reporting in Asia Pacific is ng/L, consistent with the recommendations of the International Federation of Clinical Chemistry and Laboratory Medicine Task Force on Clinical Applications of Cardiac Biomarkers.6
Serial testing is required for all patients requiring troponin testing
Supporting evidence
Troponin levels evolve over the course of ACS,28 reflecting the extent of myocardial damage.24 International guidelines now recommend that more than one hs-Tn test is taken during the assessment and treatment of patients with suspected ACS.4 ,22 ,24 Serial measurements allow physicians to assess the change in hs-Tn levels, which (when considered together with the baseline level) increases the negative predictive value of the test.29 ,30 Data with hs-Tn I assays show that a single baseline hs-Tn test could accurately identify 88%–95% of patients with AMI (depending on presentation time after chest pain onset), but serial measurements increased the detection rate of AMI to 100%.31 Serial testing improves the diagnostic accuracy of hs-Tn I and hs-Tn T levels.32 Stable hs-Tn levels during serial testing are likely to indicate chronic myocardial damage,33 such as heart failure.34
For hs-Tn, testing is suggested at the time of presentation (0 hour) and 3 hours later
Supporting evidence
The initial hs-Tn test should be conducted as soon as possible after presentation. Although the optimal timing of the second hs-Tn measurement has not been established, the European guidelines recommend retesting at 1 or 3 hours after presentation.24 However, the Asia Pacific expert panel recommends retesting at 3 hours for the following reasons:
Retesting at 3 hours is recommended in the Third Universal Definition of MI.25
Using both the baseline level and a change in hs-Tn measured after 1 or 2 hours provides a small but non-significant improvement in diagnostic performance relative to that of a single baseline measure.35 Using both the baseline level and a change in hs-Tn measured at 3 hours produces a marked improvement in the positive predictive value (PPV) of the hs-Tn I assay.28
Clinical experience in Asia suggests that it may be impractical to retest at 1 hour because it is often difficult to get the second sample so soon after presentation due to logistical and personnel constraints. Most laboratories within Asia Pacific do not have the turnaround speed required to make the 1-hour draw meaningful.
Gender-specific cut-offs should be considered for the Abbott hs-Tn I assay (99th percentile: 16 ng/L for women; 34 ng/L for men)
Supporting evidence
The clinical spectrum of ACS differs between men and women. Women tend to develop ACS at an older age than men and are more likely to have comorbidities, such as diabetes, hypertension, renal dysfunction or overweight/obesity.36–41 Coronary artery disease is more likely to go undetected in women than men, because their coronary atheroma burden is lower and they are more likely to have non-obstructive disease on angiography.36 ,40 ,42 ,43 The Valsartan in Acute Myocardial Infarction Trial indicated that women and men had a similar age-adjusted and risk factor-adjusted mortality rate after ACS, but the incidence of composite cardiovascular events was higher in women because of greater rates of hospitalisation.44
In addition, the symptoms of ACS differ between genders—women are less likely to experience chest pain,45 ,46 and are more likely to experience shortness of breath or nausea.46 ,47 This could lead to delays in diagnosis48 and more conservative treatment of women with non-ST-segment elevation ACS,49 which may result in unsatisfactory outcomes. Studies in Singapore38 and Korea39 suggest that women in these countries have higher mortality rate after ACS than men. Within Asia Pacific, social support for women may also be poorer compared with men.
These gender differences highlight the importance of accurately diagnosing ACS in women. As described earlier, using gender-specific 99th percentiles significantly increases the number of women who are accurately diagnosed with ACS, without affecting the number of men diagnosed.20 Therefore, the Asia Pacific consensus group supports the use of gender-specific thresholds in the interpretation of hs-Tn I levels, such as that in the Abbott ARCHITECT STAT assay product insert, which recommends thresholds of 16 ng/L in women and 34 ng/L in men.
For ruling in AMI, the cut-off for a highly abnormal reading is 10 times the upper limit of normal
Supporting evidence
With the early (contemporary) cardiac troponin tests, any detectable cardiac troponin could be assumed to result from acute myocardial injury, making it simple to ‘rule in’ patients with elevated levels as having ACS.34 However, high-sensitivity assays are now capable of detecting much lower levels of circulating troponin that may be indicative of more subtle or transient myocardial injury, not necessarily ACS.34 Therefore, to ‘rule in’ a diagnosis of ACS, a clear elevation in hs-Tn is required.
The Asia Pacific consensus group recommends that only hs-Tn I levels of more than 10 times the upper limit of normal (ULN) should be considered as markedly elevated. Current European guidelines use a ‘rule-in’ level of 52 ng/L for hs-Tn T (Roche assay) and for hs-Tn I (Abbott assay).24 These levels are approximately four and two times the ULN for hs-Tn T (based on a 99th percentile of 14 ng/L) and hs-Tn I (based on a 99th percentile of 26 ng/L), respectively. Early studies with hs-Tn T showed that using a threshold of five times the ULN still only had a PPV of 84%.50 Therefore, the Asia Pacific consensus group recommended a more stringent criterion, which has a higher PPV. Patients with this magnitude of hs-Tn I elevation can be considered as having a high diagnostic likelihood of ACS and managed accordingly, but this does not preclude them from a 3-hour retest to confirm the diagnosis.
However, it must be emphasised that the diagnosis of ACS should not be based merely on biomarker elevation. Rather, an integrated approach should be taken, considering the presence of factors associated with ACS, such as a patient history with multiple CV risk factors, ischaemic ECG changes and echocardiographic wall-motion abnormalities.
For patients with hs-Tn I levels >99th percentile, a dynamic change of >50% at the 3-hour retest classifies them as high-risk AMI. Patients with levels >99th percentile at baseline and a dynamic change of <50% at 3 hours should be assessed for alternate causes of elevated troponin
Supporting evidence
This recommendation is based on a careful analysis of the diagnostic performance of hs-Tn I levels using serial measurements (at admission, 3 and 6 hours) in 1818 patients with suspected ACS.28 The diagnostic performance parameters derived from this analysis are shown in table 3.28 This study demonstrated that the PPV of hs-Tn I is maximised when there is a >50% change in the level between the admission test and the 3-hour retest.28 A <50% change suggests that hs-Tn I levels remain within a relatively stable range, likely indicating chronic myocardial damage,34 which prompts for a reassessment of the diagnosis.
Diagnostic performance of the high-sensitivity troponin I (hs-Tn I) assay28
Use of POC testing may be required in some suburban or rural regions due to logistical limitations
If the reading is elevated, the patient may be classified as high-risk disposition.
If the reading is normal or undetectable, repeat testing at 6 hours or send patient for formal lab testing: DO NOT RULE OUT AMI.
Supporting evidence
Wherever possible, the Asia Pacific consensus group recommends the use of laboratory assays for the determination of hs-Tn levels. However, it is reasonable to use POC troponin tests in some centres like rural hospitals, which may have limited access to the required laboratory services.
POC troponin tests are less sensitive than hs-Tn laboratory assays,51 ,52 with PPV only around 50%.52 Therefore, any patient with an elevated troponin level on POC testing should be considered as being at high risk of having ACS. These patients should undergo further assessment according to the algorithm outlined in figure 2. Any subsequent tests to assess change should be undertaken using the same POC assay, as there is considerable variability between assays.53
As POC troponin testing systems have good specificity but low sensitivity, a result that is low or undetectable does not preclude the possibility of ACS.54 It is recommended that a sample is sent to the laboratory for hs-Tn evaluation. If this is impossible, the POC troponin test should be repeated at 6 hours to assess changes.
All personnel ordering troponin tests should be regularly educated about the optimal use and interpretation of the result, based on the assays used at respective centre
Supporting evidence
Modern hs-Tn assays provide an opportunity to improve ACS diagnosis and patient outcomes, but, like any clinical tool, these need to be applied appropriately for optimum benefits. Data showed that the introduction of these tests at a UK hospital was suboptimal, with problems including inappropriate requests,55 incomplete information in the laboratory request56 and long turnaround times for results.56 The Asia Pacific consensus group recommends regular education of personnel on the appropriate use of troponin tests in clinical practice, including:
The analytical characteristics of the test used at that hospital/medical centre
The need for serial testing in all patients
The interpretation of the results in relation to the 99th percentile for that particular assay, including gender differences, the units used, changes over time versus stable levels
The integration of hs-Tn results into the diagnostic algorithm, alongside other information from the patient's history, clinical signs, ECG and imaging results
Caution in interpretation in presence of comorbidities. For example, published data suggest that renal insufficiency may influence the cut-off levels of certain hs-Tn assays.57
Education should be repeated at regular intervals or when there is a change in assay or personnel, which include ED physicians and nurses, cardiologists and medical students. When a new laboratory assay for hs-Tn is being introduced, the education should precede the assay's introduction.
Conclusions
Given the increasing heart disease burden in this region, it is important to optimise the diagnosis and treatment of patients with ACS. This includes the appropriate use of hs-Tn levels for diagnostic purposes, with the aim of preventing errors and improving the standard of care. We proposed an algorithm that will potentially reduce delays in discharge by the accurate ‘rule out’ of patients without ACS within 3 hours, though it must be considered in the full context of the management of suspected ACS, which consists of a classical history in an individual with multiple CV risk factors, ischaemic ECG changes and echocardiographic wall-motion abnormalities. This algorithm is merely for the interpretation of hs-Tn I levels; it is not a complete diagnostic algorithm and therefore should be used in conjunction with other clinical findings. We recommend that regular education and appropriate research be undertaken to ensure the efficacy and safety of the algorithm in clinical practice, with the long-term goal of improving care of patients with ACS regionally.
Acknowledgments
We would like to acknowledge MIMS Pte Ltd for providing writing and editorial assistance.
References
Footnotes
Contributors Category 1—Conception and design of study: JWCT, LC, MI-D, W-TC; Acquisition of data: TCA, CSPL, KHY, AP, SSM; Analysis and/or interpretation of data: JMA, VPD, TAMC, PT, KHC. Category 2—Drafting the manuscript: JWCT, CSPL, LC; Revising the manuscript critically for important intellectual content: JWCT, CSPL, SSK, TCA, JMA, WTC, VPD, MI-D, SSM, AP, TAMC, PT, KHY, LC. Category 3—Approval of the version of the manuscript to be published: JWCT, CSPL, SSK, TCA, JMA, WTC, VPD, MI-D, SSM, AP, TAMC, PT, KHY, LC.
Funding Abbott Laboratories (Singapore) Pte provided logistic support and funding for the Asia Pacific Troponin Advisory Board Meeting and MIMS Pte to provide editorial support.
Competing interests All authors were provided with logistical support to attend the advisory board meeting. In addition, LC has received institutional research grants and honorarium from Roche, Abbott Diagnostics, Alere, Siemens and Radiometer Pacific. CSPL is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore; has received research support from Boston Scientific, Bayer, Thermofisher, Medtronic and Vifor Pharma and has consulted for Bayer, Novartis, Takeda, Merck, Astra Zeneca, Janssen Research & Development, LLC, Menarini, Boehringer Ingelheim and Abbott.
Provenance and peer review Not commissioned; externally peer reviewed.