Article Text

Abstract
Objective To identify the characteristics, treatments and hospital outcomes of patients diagnosed as having acute coronary syndrome (ACS) in the United Arab Emirates (UAE).
Design A 3-year prospective registry.
Setting Four tertiary care hospitals in three major cities of UAE from December 2003 to December 2006.
Patients 1842 eligible consecutive patients with suspected ACS.
Interventions None.
Main outcome measures Characteristics, treatments and in-hospital outcomes were recorded.
Results The mean age was 50.8±10.0 years, and 93.1% were male. More than half (51%) had ST elevation myocardial infarction (STEMI). The smoking rate was 46.4%, and diabetes was present in 38.9%. Only a minority (17.3%) used the ambulance services. For patients with STEMI, the median symptom to hospital time was 127 (IQR 60–256) min, and the median diagnostic ECG to thrombolysis time was 28 (IQR 16–50) min. Reperfusion in STEMI was in 81.4% (64.8% thrombolysis and 16.6% primary percutaneous coronary intervention). During hospitalisation, only a minority of the patients did not receive antiplatelets, anticoagulants, beta-blockers, ACE inhibitors and statin therapy. In-hospital complications were not common in our registry cohort. In-hospital mortality was 1.68%.
Conclusions ACS patients in UAE are young but have higher risk factors such as smoking and diabetes. Almost half present as STEMI. Only a minority use ambulance services.
Statistics from Altmetric.com
Introduction
Ischaemic heart disease (IHD) is the leading cause of death globally.1 It has been projected that between 1990 and 2020, ischaemic heart disease mortality in the Middle East countries (MEC) will increase by 146% for women and 174% for men.2
Most data for patients with ACS are from several large registries from developed countries and more recently from India.3–8 In the Arab world, a small registry was published from Kuwait.9 None has been published from UAE. The UAE-Acute Coronary Syndrome Registry (UAE-ACS Registry) is a prospective 3 years observational study of consecutive patients hospitalised with suspected ACS. It is the first ACS registry carried out in the UAE. It aims at identifying the characteristics, treatments and hospital outcomes of patients diagnosed as having ACS. Here we report the findings of this registry.
Methods
Study participants
We established a prospective multicentre registry that recruited patients with ACS from four major hospitals in three cities of UAE: Al Jazeera Hospital in Abu Dhabi, Al Ain Hospital in Al Ain, Rashid Hospital and Dubai Hospital in Dubai. All these hospitals are government-owned and provide free emergency services to all patients with ACS. Every centre prospectively enrolled all consecutive ACS patients admitted to all their wards. Data were recorded during admission up to discharge.
The diagnosis of different type of ACS and definitions of data variables were based on American College of Cardiology (ACC) clinical data standard.10 Myocardial infarction was classified as: (1) ST elevation myocardial infarction (STEMI), (2) non-ST elevation myocardial infarction (NSTEMI) and (3) left bundle branch block (LBBB)/uncertain. The patient should manifest a typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis with at least one of the following:
Ischaemic symptoms, which may include: (1) unexplained nausea and vomiting or diaphoresis; (2) persistent shortness of breath secondary to left ventricular failure; (3) unexplained weakness, dizziness, lightheadedness or syncope;
Development of pathological Q waves on the ECG;
ECG changes indicative of ischaemia: (1) ST segment (STEMI) elevation: new or presumed new ST-segment elevation at the J point in two or more contiguous leads with the cut-off points greater than or equal to 0.2 mV in leads V1, V2 or V3, or greater than or equal to 0.1 mV in other leads; (2) NSTEMI elevation: either of the following (in the absence of ST elevation): ST-segment depression or T-wave abnormalities;
Unstable angina was defined as angina pectoris (or equivalent type of ischaemic discomfort) with any one of the three following features:
angina occurring at rest and prolonged, usually more than 20 min;
new-onset angina of at least Canadian Cardiovascular Society (CCS) classification III severity;
recent acceleration of angina reflected by an increase in severity of at least one CCS class to at least CCS class III.
The patient must also not have any biochemical evidence of necrosis.
Patients transferred from other centres were excluded. We recorded age, sex, medical history, baseline clinical characteristics, time to reach hospital, time from admission to thrombolysis, treatment at hospitalisation and at discharge and in hospital outcomes.
Statistical analysis
The data are presented as frequencies, means and medians. The means are calculated with standard deviations, while medians are calculated with interquartile ranges (IQR). Categorical and continuous variables were compared using the χ2 test and t test, respectively. A p value of <0.05 was considered statistically significant. All data analyses were carried out using StatView for Windows, SAS Institute version 5.0.1.
Results
Patient characteristics
During the period of the study, 1842 patients with suspected ACS were registered. The demographic details and baseline characteristics are presented in table 1.
Baseline demographic and clinical characteristics of registry cohort
The overall median symptom onset to presentation was 170 (IQR 75–450) min. The final discharge diagnosis was ST segment elevation MI (STEMI) in 913 patients (51.0%), NSTEMI in 573 (32.0%) and unstable angina (UA) in 303 (16.9%), and data were not available in 53 (2.8%) patients.
The mean age was (50.8±10 years), and the majority of the patients were male (93.1%). Patients with STEMI were younger (49.1±8.9) than NSTEMI (51.8±10.5) (p≤0.0001) and UA (54.2±10.6) (p≤0.0001). A previous history of coronary artery disease was found in 25.7% of all patients, diabetes mellitus in 38.9% and current smoking in 46.4%. The rate of diabetes was significantly higher in UA patients (45.9%) than STEMI (34.9%) (p=0.003), while STEMI patients were found to have a higher smoking rate (55.2%) than NSTEMI (41.9%) and UA (29.4%) (p≤0.0001). The rate of hypertension was highest in UA (48.8%) compared with NSTEMI (38.7%) and STEMI (28.3%). (p≤0.0001). Upon presentation, 11.6% of the patients had a left-ventricular failure. Only 315 (17.3%) came to the hospital by ambulance.
In-hospital and discharge medical therapy
With regard to in-hospital medical therapy and intervention (table 2), only a minor proportion (3.0 %) of the patients with ACS did not receive aspirin, and about 27% of patients with NSTEMI did not receive clopidogrel. Low-molecular-weight heparin was the predominant heparin formulation used. Glycoprotein IIb/IIIa inhibitors were used more frequently in NSTEMI (66.3%) than in STEMI (25.5%) or UA (26.0%). Although beta-blockers were commonly prescribed in all subgroups, the ACE inhibitor was used less frequently in patients with NSTEMI. Lipid-lowering drugs, especially statins, were used in more than 90% of the patients. Among patients with diabetes mellitus, insulin was used more frequently in patients with STEMI than oral agents. A coronary angiogram (and angioplasty if indicated) was performed in 53.3% of all patients during admission with ACS while exercise stress test done only in 1% of all patient with acute coronary syndrome.
A substantial proportion of patients (11.3%) with UA did not receive aspirin at discharge, and 33.2% of patients with NSTEMI did not receive clopidogrel at discharge (table 2).
In-hospital and discharge pharmacological and intervention treatments based on final diagnosis
Reperfusion therapy for STEMI
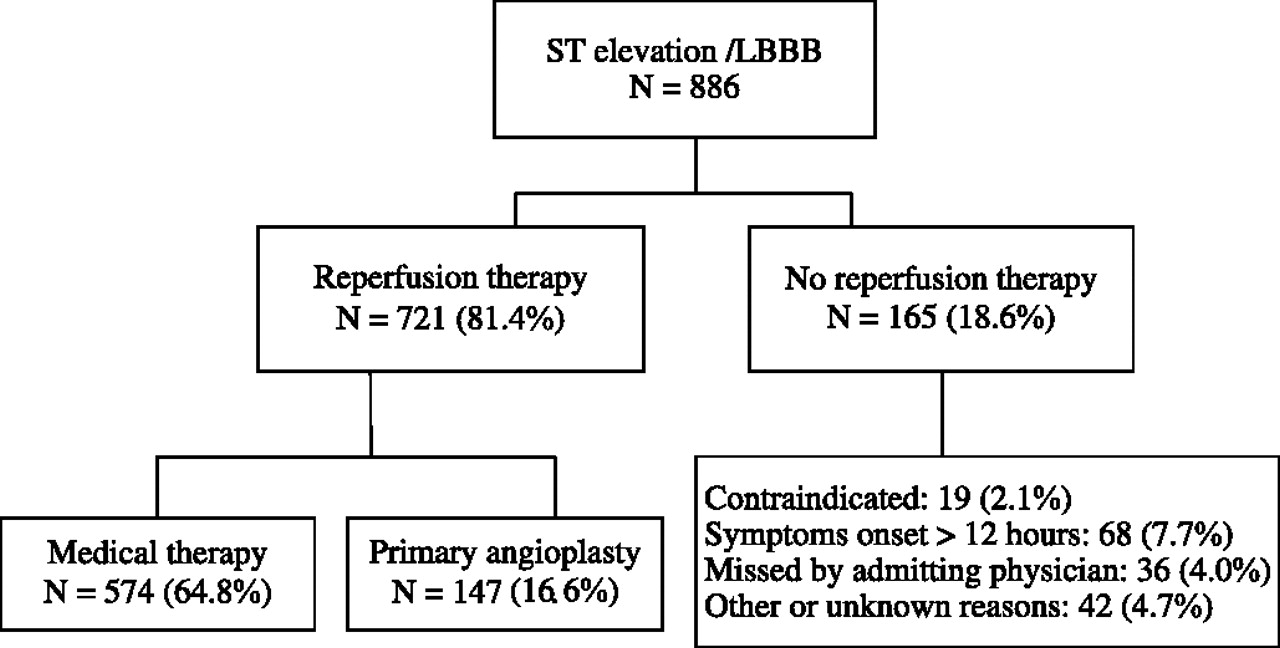
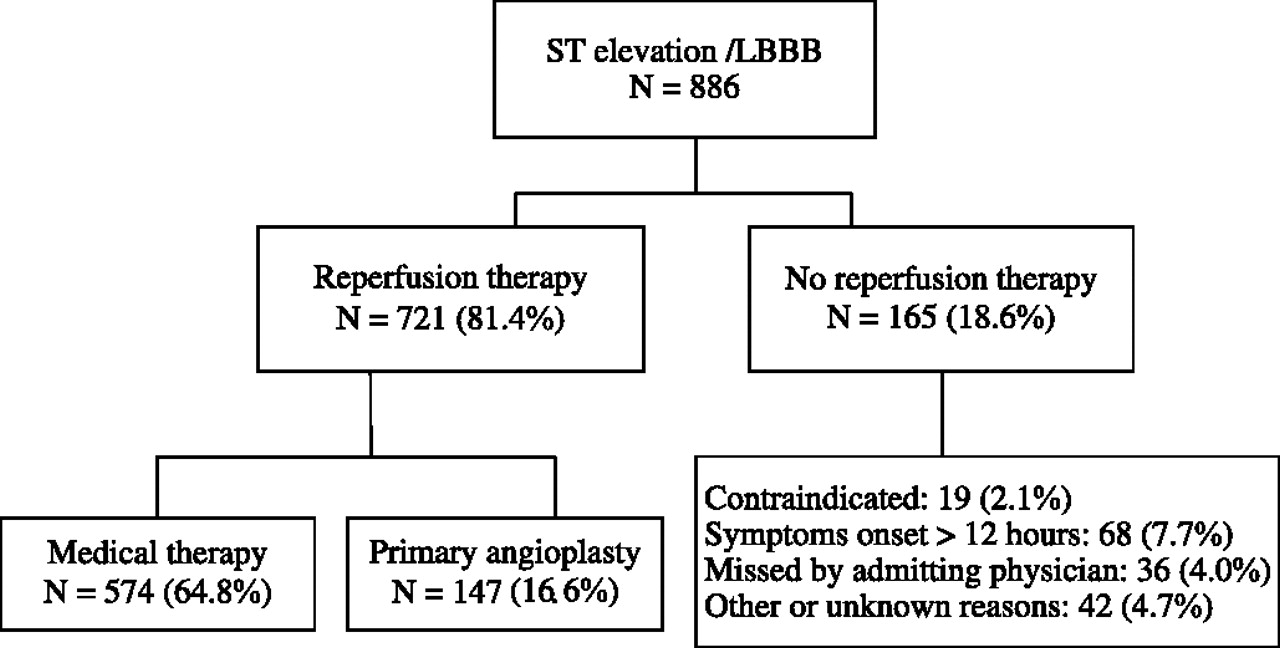
Among patients with ST elevation ACS and LBBB (886 patients), 81.4% received some form of reperfusion therapy (figure 1). Five hundred and seventy-four patients (64.8%) received fibrinolytic therapy, and 147 patients (16.6%) underwent primary percutaneous intervention.
{kind=link}
Reperfusion therapy for ST elevation myocardial infarction.
The main fibrinolytic agents were Tenecteplase (70.8%), Retaplase (21.3%) and Streptokinase (7.1%). Of those who received thrombolytic therapy, the median time of onset of symptoms to the diagnostic ECG was 135 (IQR 65–275) min. The median time from diagnostic ECG to needle (available for 96.7% of patients) was 29 (IQR 16–52) min. Reperfusion therapy was not used in 68 patients due to late presentation, and 19 patients with contraindication, and 36 patients were missed by the admitting doctor.
In-hospital complications and mortality
In-hospital complications were not so common in our registry cohort. Recurrent ischaemia was reported in 7.3% and 3.3% of the patients who developed congestive heart failure. Mechanical ventilator was used in 3.3% and inotropes used in 3.5% of the patient. Ventricular tachycardia/ventricular fibrillation was reported in 3.5% and cardiogenic shock in 2.2% of the patients during their hospital stay. The in-hospital mortality was 1.68%.
Discussion
We analysed data from a large registry of patients with ACS from the UAE. We assessed the characteristics of patients, practice patterns and rate of major outcomes from four large government hospitals in three of the largest cities of the UAE. In these tertiary hospitals, free treatment is available for any acute cases.
Table 3 compares our registry with that of various registries in the region as well as that from the developed world. In contrast to the data from developed countries, but consistent with data from developing countries, we recorded more cases of STEMI than NSTEMI or unstable angina. We had the youngest patients with STEMI compared with the GRACE study, European Heart Survey I & II, India, as well as Kuwait.3–9 This has important implications and could be partially explained by the large number of young adults who come to the UAE for employment, but it also means that these young people have a large amount of risk factors sufficient for them to suffer MI, as shown recently in an analysis of young individuals with acute MI.11 For instance, in STEMI, our patients had a smoking rate of 55.2% and diabetes rate of 34.9%, compared with India where the current smoking rate in ST elevation was 27.9% and diabetes rate 30.4%.8 Current smoking in European Heart Survey I & II was 42.8% and 45.6%, while the diabetes rate was in only 21.1% and 21.4%.6 7 This calls for primary prevention especially in this segment of society.
Comparison of our registry with that of various registries in the region and from the developed world
Few patients used an ambulance to reach the hospital; most used private or public transport. Although we had the lowest onset of symptoms to admission time compared with other registries, we should reduce this further if we can. We need to educate our patients to recognise the signs of ACS and ask for medical attention earlier, and make our ambulance services available and efficient to patients with ACS, so they can be transported to the hospital much faster and more safely.
Table 3 also shows our practice and management for STEMI compared with other registries. In our study, the rate of primary percutaneous coronary intervention was lower, at 16.6%, compared with 18% in GRACE3–5 and 38% in European Heart Survey II.7 This was because primary percutaneous coronary intervention was available only during the daytime hours. However, our overall reperfusion rate in ST elevation was much higher, 81.4% compared with 77% in Kuwait, 67% in India, 56% in Euro Heart Survey I and 64% in Euro Heart Survey II.6–9 The use of key medical treatment antiplatelet drugs, beta blockers, ACE inhibitors and lipid-lowering drugs was similar if not better than other registries. For instance, in EHS II,7 antiplatelets such as aspirin, Clopidogrel/Ticlopidine and GP IIb/IIIa inhibitor were used in 96.8%, 69.8% and 30.7%, respectively of patients with STEMI, compared with 98.9%, 48.0% and 25.5%, respectively, in our patients, while beta blockers, ACE inhibitors/ARBs and statins were used in 83.0%, 75.4% and 80.7%, respectively, compared with 82.7%, 75.8% and 96.7%, respectively, in our registry.
For patients with NSTE ACS, antiplatelet therapy such as aspirin, Clopidogrel/Ticlopidine and GP IIb/IIIa inhibitors was used in 94.5%, 67.4% and 20.8%, respectively, in EHS II compared with 96.6%, 71.2% and 52.4%, respectively, in our cohort with NSTE ACS, while beta blockers, ACE inhibitors/ARBs and statins were used in 82.8%, 69.5% and 73.7%, respectively, in EHS II compared with 83.8%, 68.8% and 93.9% respectively in our registry.
Because all of the patients received similar and free treatment in our centres, there should not be any difference in treatment across the socio-economic strata, as was seen in the registry from India.8 However, follow-up treatment could be different, as patients do not receive this free of charge.
The mortality in our patients was very low (1.65% in STEMI and 1.62% in NSTEMI) and compares favourably with other registries (table 3). This could be explained partially by our young patients and low comorbidities.
There are several limitations to our study, as the centres in our study were not randomly selected, and volunteered to participate. Thus, practice patterns of such tertiary centres might not necessarily represent the practice in all hospitals in the country. However, we believe a large number of MI patients and ACS patients come to these major centres, which are free of charge and government-owned. These were the only centres where nearly all the patients have been attending before the recently opened private hospitals. Second, follow-up was not available in this registry, and we do not know what happened to these patients especially if their socio-economic status did not allow them to continue to take their medications.
Conclusion
Patients with ACS in large centres of the UAE tend to be very young and have a higher rate of STEMI than do patients in developing countries. They also have a reduced comorbidity. They attend for medical attention on their own rather than by ambulance but receive fairly prompt and evidence-based treatment in terms of revascularisation and antiplatelet, beta blockers, ACE inhibitors and lipid-lowering drugs. The in-hospital mortality is low. However, we do not know their 30-day and longer mortality and morbidity. We need strategies to improve the huge burden of risk factors which give these young people IHD in the first place and to reduce further the delays in recognising the symptoms of ACS and accessing early medical care.
Acknowledgments
We would like to thank AA Alsheikh-Ali, for his kind advice and help.
References
Footnotes
Funding MSD partly funded this project.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.