Article Text

Abstract
Aneurysmal arterial origin of coronary fistulae is an extremely rare combination. We report a case of a giant left main coronary artery to right atrium fistula in a 48-year-old male. We describe the clinical course and management options.
- Aneurysm
- fistula
- coronary disease
- coronary-artery-fistulae
- left-main-coronary-artery
- coronary-aneurysm, congenital heart disease
- coronary artery disease
Statistics from Altmetric.com
- Aneurysm
- fistula
- coronary disease
- coronary-artery-fistulae
- left-main-coronary-artery
- coronary-aneurysm, congenital heart disease
- coronary artery disease
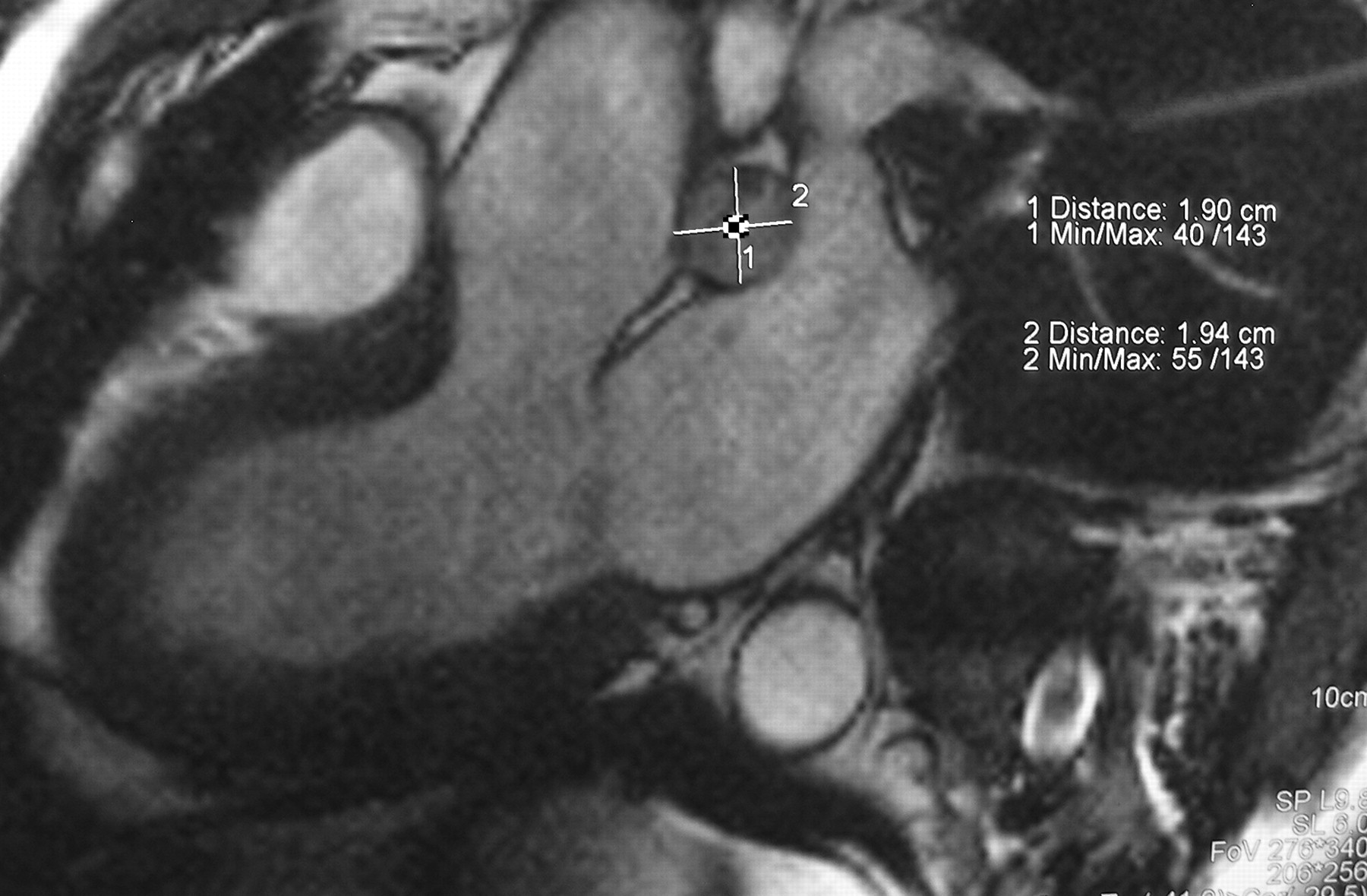
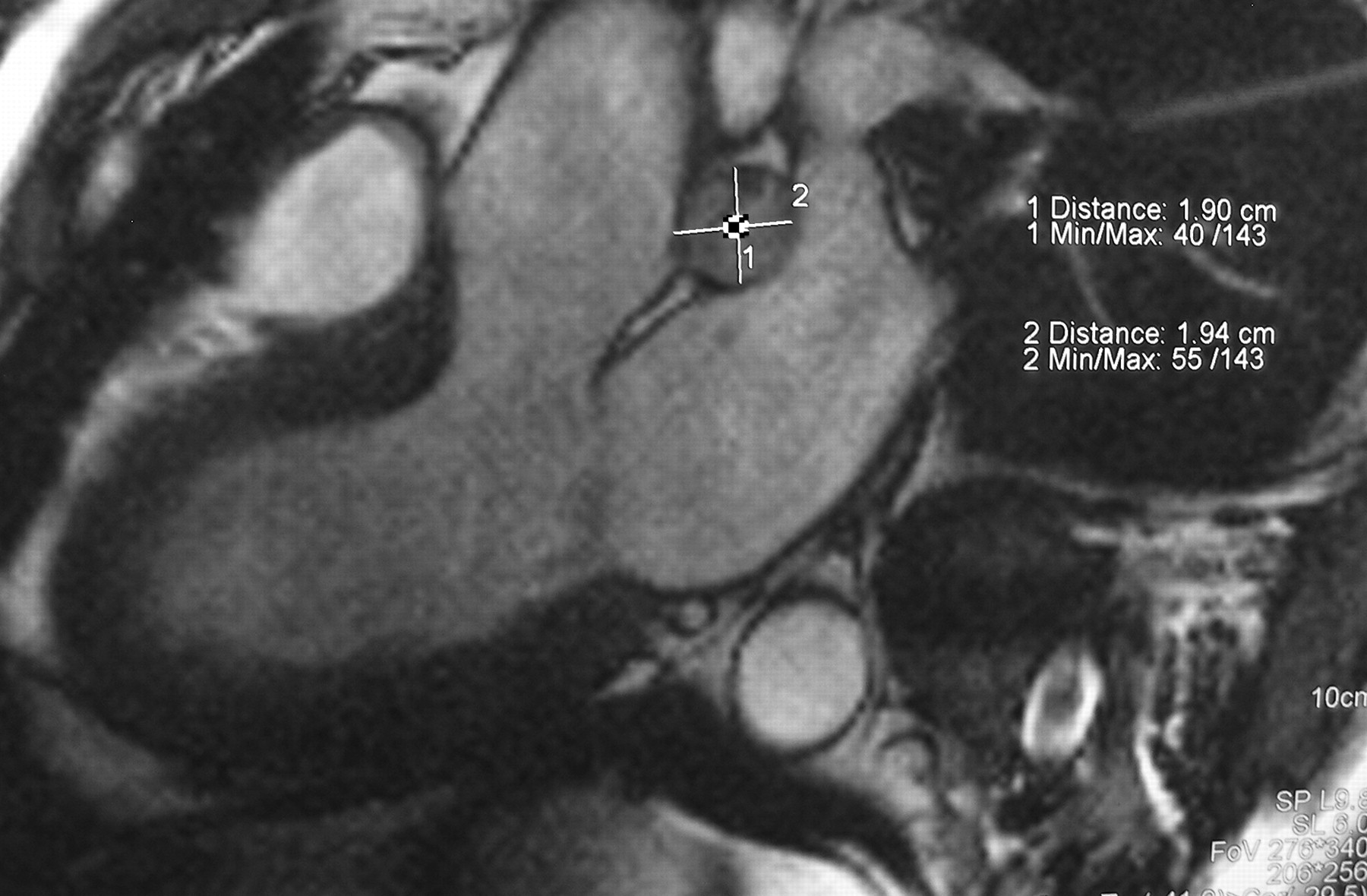
A 48-year-old hypercholesterolaemic male patient with a 1-year-long atypical non-exercise-related chest pain was referred for cardiological evaluation. No congestive heart failure symptoms, other cardiovascular risk factors or comorbidities were present. He had no history of chest trauma or surgical/interventional heart procedures. Physical examination revealed a left upper sternum border 2/6 systolic murmur. Chest x-ray and electrocardiogram recordings were normal. Transthoracic echocardiogram showed a dilated left main coronary artery ostium and a 7 cm long abnormal and severely dilated (18 mm in diameter) arterial vessel behind the aortic root with a continuous flow with systolic augmentation by colour-Doppler shunting into the right atrium. There was no right atrial or ventricular dilatation and right ventricular function was normal. Coronary angiography demonstrated a 17 mm left main coronary artery shunting into the right atrium (figure 1) with an unexpected and perfect right ventriculography at the end of the contrast injection. The calculated Qp/Qs was 2.02. No atherosclerotic coronary artery stenosis were found. Cardiac MRI confirmed the diagnosis (figures 2, 3). With these findings, it was decided to adopt conservative non-surgical management of the patient. No pharmacological treatment was added. After 6 months of clinical and cardiac resonance imaging follow-up, no major adverse cardiac events have occurred, and the patient remains in a good functional class with no progressive right heart or aneurysmal dilatation.

Coronary angiography; left main coronary artery shunting into the right atrium.

Cardiac MRI.
{kind=link}
{kind=link}
{kind=link}
Left main coronary artery severely dilated behind the aortic root.
Coronary artery fistulae are found in 0.1–0.2% of routine angiograms, and most of them are clinically silent. When symptomatic, clinical manifestations may include exertional dyspnoea and/or angina, syncope and palpitations.1 The right coronary artery is the most frequently involved, followed by the left coronary artery.2 Most are originally congenital, but other causes may be present such as that previously mentioned. Our manuscript reports a giant congenital fistula from a severely dilated LMCA shunting into the right atrium. Aneurysmal arterial origin of coronary fistulae is an extremely rare combination. Such huge extramyocardial communications are not always life-threatening because most of the right atrial shunting flow is systolic (when myocardial perfusion is minimal) and usually restrictive, allowing only limited left-to-right shunting (in our case, a QP/QS of 2.0 was calculated).
Current options for coronary artery fistulae treatment include close clinical follow-up, surgical ligation or transcatheter embolisation. It is uniformly accepted that patients with symptoms must be aggressively treated, and surgical or transcatheter closure is recommended. Surgical repair3 and percutaneous transcatheter embolisation using occlusion devices as an alternative to conventional surgery have been reported with good results in a limited number of cases. However, the management of asymptomatic patients is still controversial.4 Aneurysmal growth may provoke compressive symptoms, coronary artery dissections or intramural rupture with subsequent cardiac tamponade, acute myocardial infarction and sudden death.1 When a significant Qp/Qs is present, these fistulae may induce congestive heart failure, myocardial ischaemia, arterial pulmonary hypertension and right ventricular dilatation, and failure and may be complicated with infective endocarditis.5 Some previously reported evidence suggests that long-term behaviour of congenital aneurysmal fistulae is more benign than that originally atherosclerotic.
In our case, the congenital origin of the aneurysmal fistula, its unknown growing rate, the absence of symptoms or increased right heart volumes and the technically demanding surgical operation needed (LMCA ostium occlusion, dissection and ligation of the fistula and the ostial segments of the left anterior descending and circunflex arteries and total arterial coronary artery bypass grafting) justified an initial conservative management. Despite the significant QP/QS found, right heart volumes were not abnormal, and we concluded that an aggressive preventive management similar to that indicated for other frequent and easy-to-correct left-to-right shunting lesions is not justified. A close clinical 6-month follow-up with a cardiac resonance magnetic imaging test for early detection of increasing aneurysmal diameters or right heart volumes was initially performed. After this first follow-up, 1-year interval similar visits will be scheduled. Symptoms and increasing right heart dilatation or aneurysmal diameters will indicate prompt surgical repair or percutaneous closure.
Medical management of these patients is still controversial. Beta-adrenergic receptor blockers and angiotensin II receptor antagonists are beneficial treatments for great vessel aneurysmal growth and rupture prevention. Although no evidence-based information has been reported regarding improving outcomes in these rare entities, they might be useful given their similar pathophysiology.
In our opinion, further reports with appropriate long-term follow-up should be necessary to establish the optimal management options of this rare cardiac congenital disease.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.