Article Text

Abstract
Background Non-communicable diseases are on the rise globally, and developing countries are also witnessing the burden. Rising obesity levels are a matter of serious concern owing to the well-established link between obesity and non-communicable diseases. The objective of this study was to determine the effect of obesity on the prevalence of cardiovascular risk factors among the Indian population.
Methods Data on blood pressure, anthropometric and biochemical measurements were collected for 2021 subjects aged above 20 years. Measurements were restricted to only anthropometrics for those below 20 years (N=1289). The study population was categorised into three groups according to body mass index for statistical analysis.
Results The prevalence of overweight and obesity was 29.5% and 11.1%, respectively, which shows significant rising trends since 1995. Glucose intolerance, dyslipidaemia, hypertension and metabolic syndrome were significantly higher among the overweight and obese subjects than among normal subjects. The prevalence of metabolic syndrome was 59% among the obese group, showing the highest risk for that group. Overweight and obesity, increasing age, hypercholesterolaemia and family history of hypertension showed a strong association with metabolic syndrome.
Conclusion All the cardiometabolic abnormalities showed an increasing trend with increase in body mass index. The morbidity and mortality associated with cardiovascular diseases can be reduced by curbing the obesity epidemic.
- Obesity
- diabetes
- cardiometabolic risk factors
- Indian population
- cardiovascular epidemiology
- dislipidaemia
- hypertension
Statistics from Altmetric.com
- Obesity
- diabetes
- cardiometabolic risk factors
- Indian population
- cardiovascular epidemiology
- dislipidaemia
- hypertension
Introduction
Developed countries, and even the developing nations, are being affected by obesity, which is gradually reaching epidemic proportions in the 21st century. This is apparently causing an epidemiological transition where there is a shift towards an increase in non-communicable diseases and decline in communicable diseases.1 2 Lack of physical activity and excess nutrition intake are reported as major causes of overweight and obesity.3 4 Characterised by industrialisation and urbanisation, ‘sedentarism’ has produced deleterious effects on health. Sedentarism is considered to be an independent risk factor for obesity and cardiovascular diseases.5 The prevalence of overweight and obesity is very high in Europe, the Americas, the Middle East and certain Western Pacific and Polynesian Islands6 resulting in an alarming increase in non-communicable diseases globally.7 8 Overweight and obesity are linked to numerous chronic diseases and disorders such as diabetes, hypertension, hyperlipidaemia and even cancer.9–11 Currently, India is witnessing a phenomenal increase in prevalence of diabetes12 13 and obesity.14 Increased risk of type 2 diabetes is believed to have links with central obesity.9 15 This review details the epidemiology of overweight and obesity in the Indian population in an urban set-up. Our objective was to evaluate the prevalence of cardiovascular risk factors according to body mass index (BMI).
Materials and methods
Multistage random sampling was carried out to obtain a representative sample of 2021 subjects (982 males and 1039 females) aged over 20 years. For population aged 8–19 years, measurements were restricted to only anthropometrics (n=1289, 682 male:607 female). An instrument containing details of sociodemography, anthropometry, medical history, diet and physical activity was administered by trained experts. Written consent was obtained from the participants, and the study was approved by the institution's ethics committee.
Height, weight, waist and hip measurements were recorded. Venous blood samples were collected after a minimum of 8 h of overnight fasting (Fasting Blood Sugar - FBS). A second sample was collected 2 h after administering anhydrous 75 g oral glucose load in 250 ml of water Post Glucose Blood Sugar - PGBS. Plasma glucose was estimated using the glucose oxidase method. All biochemical estimations were carried out using enzymatic procedures within 5 h and a Hitachi-917 autoanalyser (Roche Diagnostics, Germany) was used for all assays. Two blood pressure measurements were taken in the resting state within an interval of 10 min.
The BMI (weight in kg/height in m2) was calculated later. Overweight was defined as a BMI of ≥25 kg/m2, and obesity was indicated by a BMI ≥30 kg/m2. A diagnosis of diabetes was made on the basis of the WHO definition for diagnosis of diabetes in the fasting state16 or a known case of diabetes. Diagnosis of the metabolic syndrome was made using modified NCEP ATP III criteria for Asian Indians.17 The presence of metabolic syndrome was confirmed when three or more of the following risk factors were present: waist circumference ≥90 cm for men and ≥80 cm for women; blood pressure 130/85 mm of Hg fasting plasma glucose (≥100 mg/dl); triglycerides ≥150 mg/dl; high-density lipoprotein (HDL) cholesterol<40 mg/dl for men and <50 mg/dl for women. To determine the effects of increasing weight on the study population, they were categorised into four groups: BMI up to 18.4 kg/m2; group I, BMI 18.5–24.9 kg/m2; group II -BMI 25–29.9 kg/m2 (overweight); and group III, BMI≥30 kg/m2 (obese). Since the abnormalities were very rare or absent in the BMI category up to 18.4 kg/m2, these are not shown in the tables.
Data were analysed using SPSS version 10.0. Age-adjusted prevalences were computed using Stata. The mean and SD were estimated for continuous variables. Prevalences are reported in percentages. The Student t test and χ2 test were used as appropriate to test statistical significance. A p value of <0.05 was considered as significant. A multiple logistic regression analysis was carried out to determine the association with metabolic syndrome as the dependent variable.
Results
The overall prevalence of overweight was 29.5%, and obesity was 11.1%. The age-standardised prevalence of obesity is shown in figure 1, where there was a greater predisposition for females to be overweight or obese compared with males, even since prepubertal age. Overweight was also significantly higher in females (figure 2). The overweight percentage has increased by 67% for both males and females since 1995.
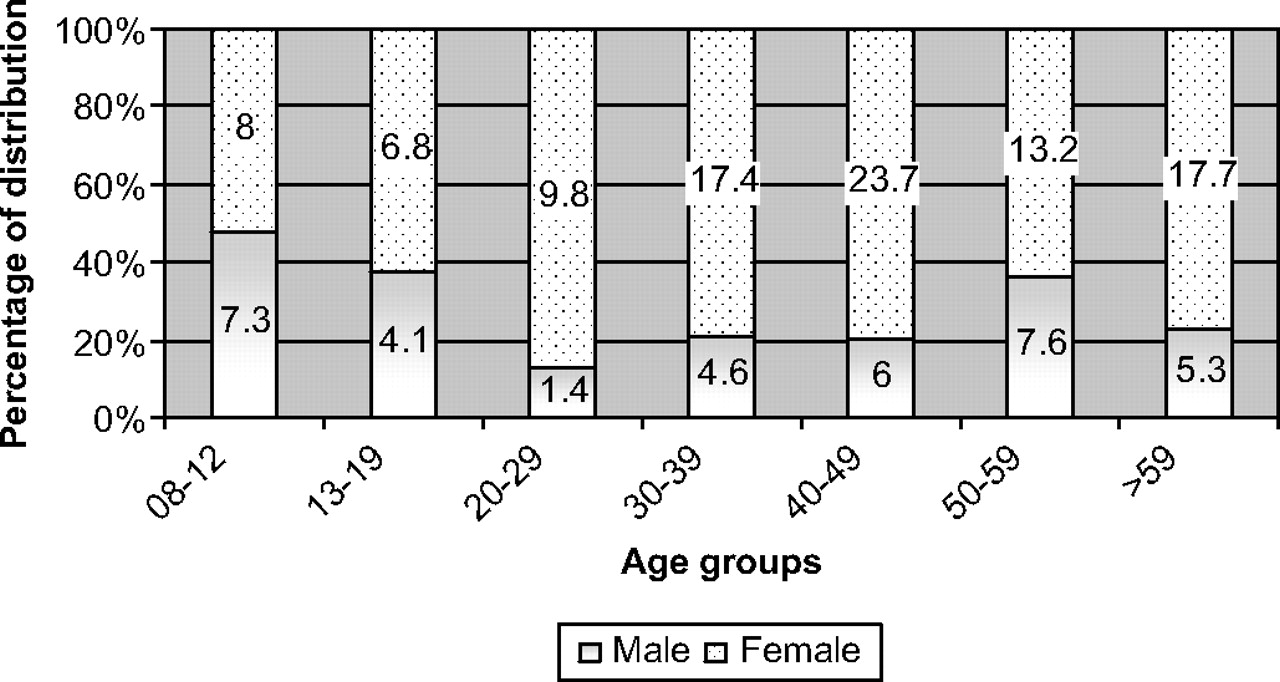
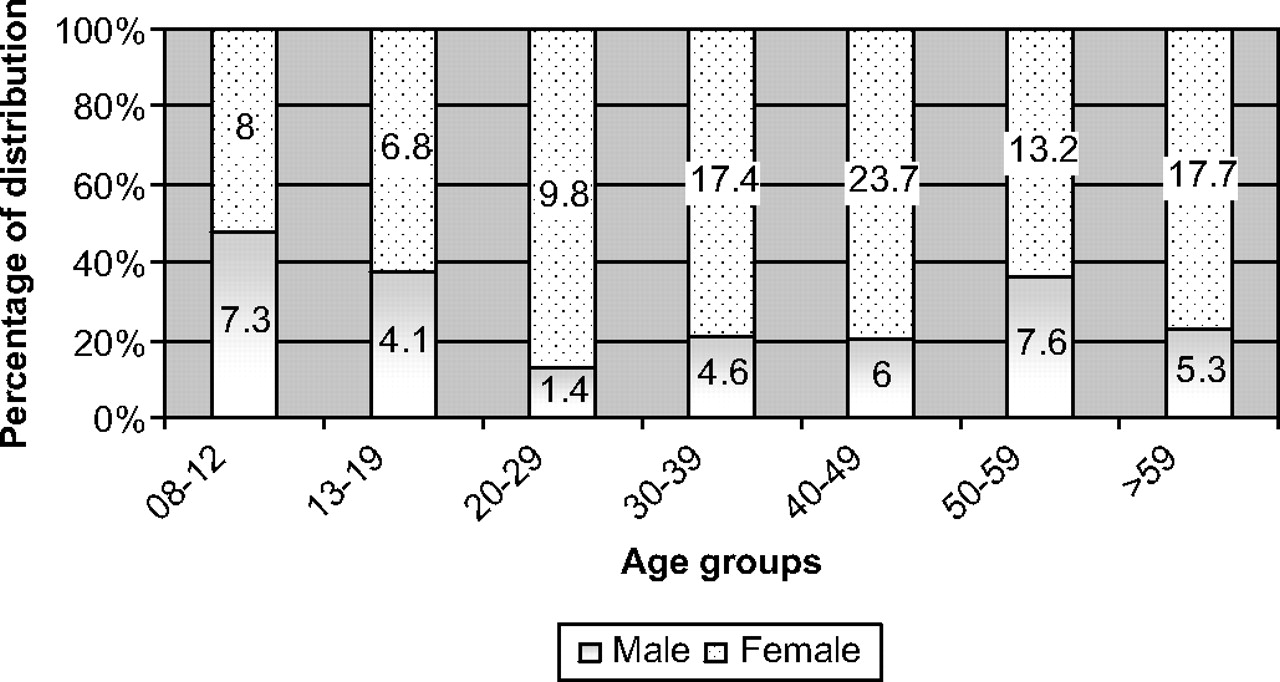
Agewise prevalence of obesity among the general population.
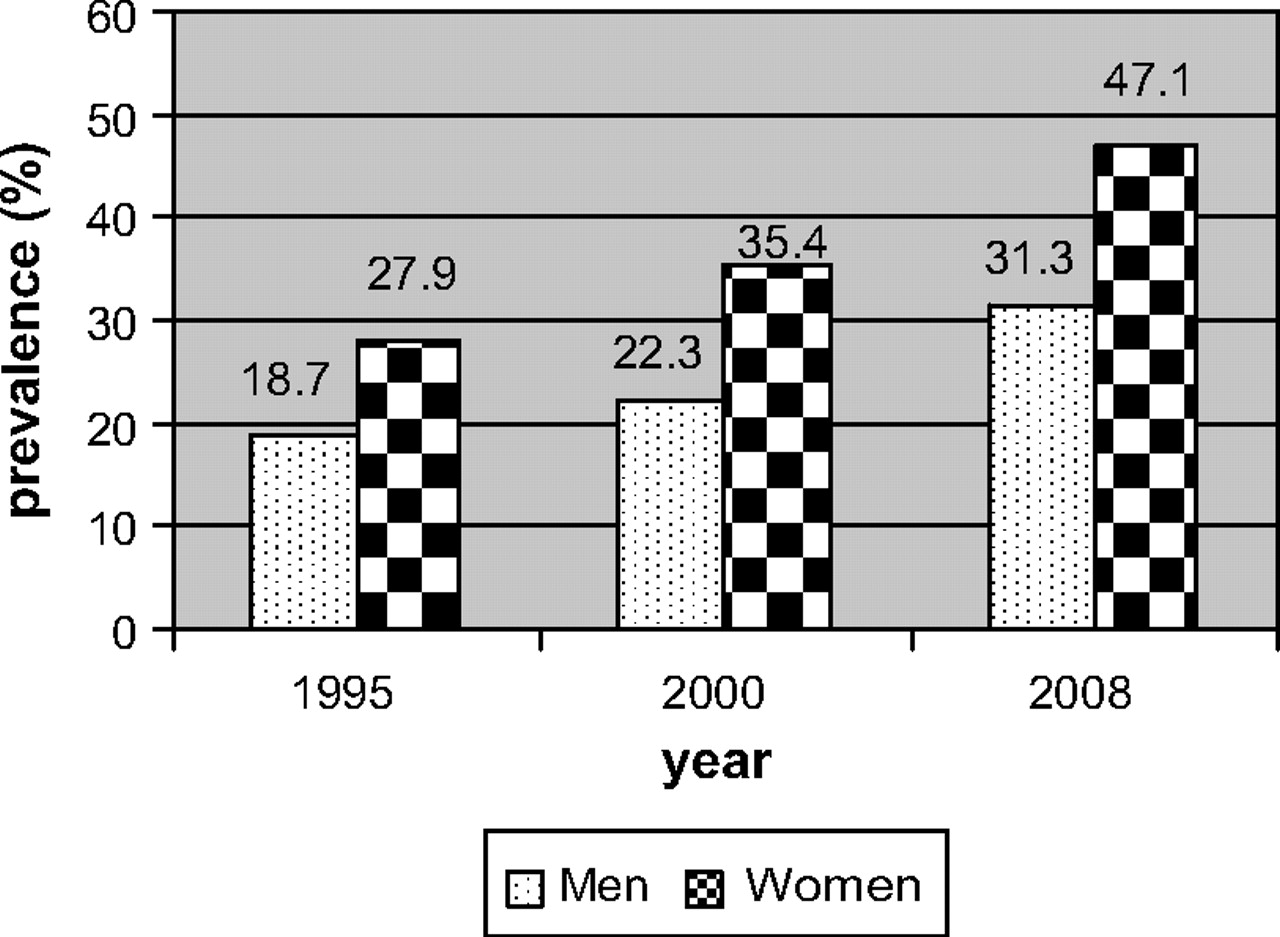
Trends in prevalence of overweight (≥85th percentiles). Rising overweight levels in Indian population observed since 1995 show a slight bias towards women.
The mean values of anthropometric, biochemical and blood pressure measurements according to BMI are described in table 1. All the lipid parameters except HDL-C showed a significant increase with BMI (Group I vs II vs III; p<0.05). Diastolic blood pressure and cholesterol levels were the only two parameters that were significantly different between groups II and III (p<0.05).
Anthropometric and biochemical parameters of the general population according to body mass index
Prediabetes, diabetes and hypertension
The overall age-adjusted prevalence of diabetes and hypertension among the study group was 19% and 32% respectively. The prevalence of glucose intolerance (impaired fasting glucose (IFG) and impaired glucose tolerance (IGT)), diabetes and hypertension according to gender and BMI are shown in table 2. Significant differences were seen in the prevalences of IFG, IGT, diabetes and hypertension between groups I and II (p<0.05).
Prevalence of prediabetes, diabetes and hypertension according to body mass index (BMI)
Metabolic syndrome
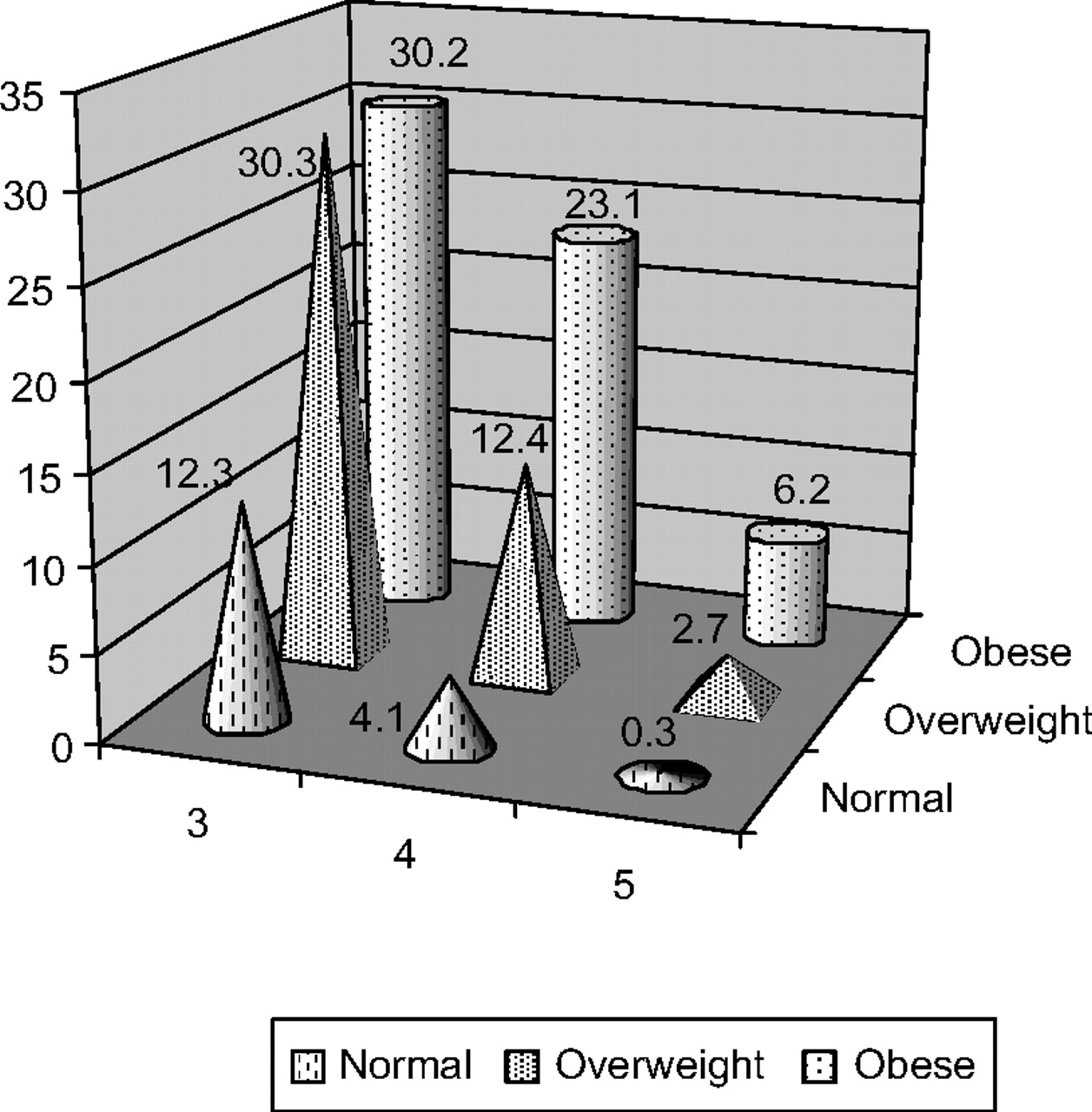
The prevalence of metabolic syndrome among the study population was around 32% (male 23.2%, female 40.1%) Females had a higher prevalence of metabolic syndrome on using modified NCEP ATP III criteria for South Asians. The prevalence of metabolic syndrome was significantly lower in the lower tertiles of BMI (p<0.0001) and was seen to rise according to BMI (group I vs II vs III; p<0.0001 vs p<0.021 vs p<0.813) (figure 3). BMI also had an effect on the number of abnormalities constituting metabolic syndrome, as the presence of three or more abnormalities was found to increase along with increasing BMI (figure 4).
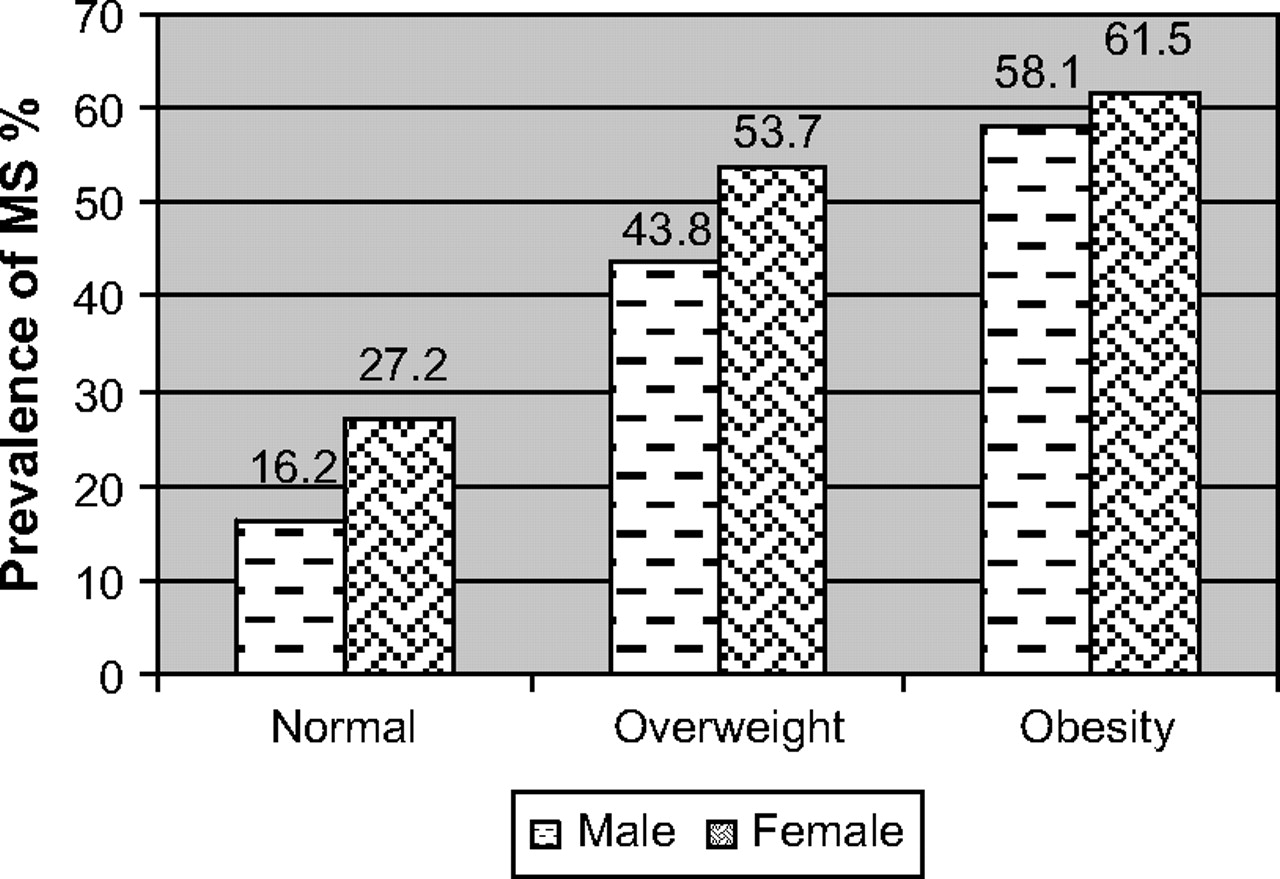
Prevalence of metabolic syndrome according to increasing body mass index. Values are shown as percentages. A significant trend was observed in the prevalence of metabolic syndrome according to body mass index.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentages of three and more parameters constituting metabolic syndrome. The number of individual abnormalities constituting metabolic syndrome increase with increasing weight.
The results of multiple logistic regression analyses with metabolic syndrome as the dependent variable showed a strong association with increasing age, overweight and obesity, hypercholesterolaemia and family history of hypertension (table 3). As per the analyses, the obese population had a 28.5-fold higher risk associated with metabolic syndrome than the non-obese.
Multiple logistic regression analysis with presence of metabolic syndrome as dependent variable
Discussion
Obesity is a chronic metabolic disorder associated with cardiovascular events, increased morbidity and early mortality. Currently, obesity may be considered to have reached pandemic levels, owing to its widespread reports from all parts of the globe.18 19
The magnitude of the effect of BMI on cardiovascular risk factors is clearly shown in this study. The study reports higher values for both systolic and diastolic blood pressure, cholesterol, triglyceride and low-density lipoprotein cholesterol (LDL-C) in both overweight and obese groups. Although not significant, lower levels of HDL-C were found in these groups, indicating the possibility of a lowered natural protective mechanism against atherosclerotic diseases. Thus, an increase in LDL-‘harmful cholesterol’ and a decrease in HDL-‘good cholesterol’ is again a cause of concern for cardiovascular morbidity.
Glucose intolerance was significantly associated with overweight and obesity. The current study showed a substantial increase in impaired fasting glucose and impaired glucose tolerance according to BMI maintaining consistency with other studies.20–23 However, an important characteristic finding was that there was no significant difference in the presence of major cardiovascular risk factors such as glucose intolerance, diabetes and hypertension between Group II and III, showing evidence that the risk is high even for non-obese Indians.
The term ‘diabesity’ has been coined to demonstrate that type 2 diabetes is dependent on obesity, and many epidemiological studies have shown that BMI is a powerful predictor of type 2 diabetes21 hypertension, hypercholesterolaemia and heart disease.24–26 The presence of metabolic syndrome, which constitutes the clustering of clinical and metabolic risk factors, is considered to be a major risk factor for coronary and ischaemic heart diseases.21 22 27 Our study has reported an increasing trend in prevalence of metabolic syndrome according to BMI. Metabolic syndrome was present in 21.7% of normal weight, 45.4% of overweight and 60% of obese subjects. There was a 176.4% increase in the prevalence of metabolic syndrome from Group I (normal group) to Group III (obese group). Regression analysis showed that overweight and obesity had the strongest association with metabolic syndrome. As the BMI increased, the number of individual risk factors constituting metabolic syndrome also increased. Three or more factors were found to be clustered among the overweight and obese group. Literature published recently has also demonstrated that an increased BMI was found to be significantly associated with a high prevalence of metabolic syndrome among specific occupational groups.28 All these data suggest that morbidity and mortality from non-communicable diseases may rise considerably in future.
The prevalence of overweight and obesity has indeed increased at an alarming rate from 1995 to 2008 in both genders largely due to urbanisation. Obesity has already hit the Western world, and it is time for Indians to wake up to the alarm bells. Overweight and obesity are found to be prevalent in all age groups, old and young alike in this study. Data from other studies show similar results in that children and adolescents from affluent strata of society were mostly above the 85th percentile of the WHO weight for age growth charts.29 Data from India on obesity trends for the urban population are sparse. These findings provide appropriate and updated statistics, and could be considered as a major source of information for planning primary prevention strategies to prevent and control obesity. Results from previous studies show a lower risk of developing diabetes with just a 5% initial reduction in weight,30 thus showing opportunities for better awareness programmes on the drive against obesity.
The controversy about which measure is a better predictor of risk is of great interest and is yet to be settled. Many studies have drawn inconsistent results,31 while some have favoured waist circumference as a better risk-assessment tool,32 33 and others have shown BMI and the waist–hip ratio to be better predictors.34 35 Although the current study used BMI as a criterion for risk assessment, it was beyond the scope of the study to compare this with waist circumference, but all the risk variables showed significant differences between the groups. Nevertheless, obesity is a result of complex interaction between genetic and environmental factors.36 Recent research has identified more than 41 sites on the genome as possible links to the development of obesity in a favourable environment.37 Further research is recommended to explore the gene–environment–obesity relations to curb the obesity ‘epidemic’ effectively.
To conclude, the magnitude of increasing overweight and obesity is a serious issue for consideration, since it is significantly associated with glucose intolerance, dyslipidaemia, hypertension and metabolic syndrome, and is likely to be the largest contributor to non-communicable-disease-related morbidity and mortality. Rising levels of overweight and obesity are a growing public-health concern. Asians are known to have much lower obesity levels than the Caucasian population, but the clustering of cardiovascular risk factors at lower BMI is of great significance and has become an issue of utmost public-health priority.28 38–40 These findings highlight the urgent need for framing direct and indirect strategies to control the obesity epidemic in future, so as to minimise the burden from non-communicable diseases in India.
What is already known on this subject
India faces an enormous burden from non-communicable diseases, which is widely known.
What this study adds
This paper brings out the latest statistics on prevalence of all the cardiometabolic risk factors in relation to body mass index.
Acknowledgments
We extend our sincere thanks to all the subjects for participating in the survey. We greatly acknowledge the contribution of epidemiology team for data collection, analysis and entry. Our special thanks to D Arut Selvi for her assistance in literature search and preparation of tables and figures.
References
Footnotes
Funding This study was funded by the Diabetes Research Centre.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Ethics Committee of DRC.
Provenance and peer review Not commissioned; externally peer reviewed.