Article Text

Abstract
Atrial fibrillation is the most commonly encountered clinical arrhythmia and continues to grow in incidence. Current management involves highly individualised therapies based on underlying concomitant disease processes and symptoms. Moreover, there are numerous therapeutic permutations involving anticoagulation, rate-limitation and antiarrhythmic strategies. This review serves to update the clinician with a practical approach to each patient population and on current advances in management.
- Atrial fibrillation
- clinical arrhythmias
Statistics from Altmetric.com
Atrial fibrillation (AF) is the most common sustained heart rhythm abnormality in clinical practice, and its presence alone is associated with increased mortality.1–5 Moreover, the impact of AF on hospital admissions and morbidity is substantial.6 The prevalence of this arrhythmia increases significantly with age, reaching close to 1 in 10 individuals with reported AF in those over the age of 80—an epidemic which will continue to grow as the population as a consequence of an ageing society, a growing census and other factors independent of age.7 Moreover, in the majority of patients with AF, particularly older people, the arrhythmia should be considered as a manifestation or surrogate of a more widespread systemic process involving the cardiac, vascular, and inflammatory and renin–angiotensin systems. For these reasons, therapy remains highly tailored to the individual, and no single treatment strategy has been proven to be superior.6 8 The more common associated comorbidities include hypertension and ventricular dysfunction (diastolic and systolic), coronary disease, valvular disease, hyperthyroidism, obesity and sleep apnoea. Control of these individual conditions has the potential to reduce the burden of AF,9–13 although additional studies are needed in order to clarify the cause-and-effect relationships, as opposed to an association, of obesity and sleep apnoea.
Beyond this focused strategies, the essential aims of AF management are: to minimise symptoms, prevent thromboembolic consequences and mitigate against the development of a tachycardia-mediated cardiomyopathy, and the most crucial of these is to prevent the devastating complication of stroke.14–18
Initial evaluation
A practical approach to the management of AF involves an initial critical assessment of its contribution to any haemodynamic instability due to a rapid ventricular response or loss of the atrial systolic contribution to cardiac output. If this is deemed clinically important, DC cardioversion using biphasic or monophasic waveforms should be performed immediately. The ‘synchronised’ mode should obligatorily be utilised to avoid a shock on the T wave and subsequent ventricular fibrillation.6
Outside the acute decompensated situation, the initial encounter should be used to clarify several broad issues: (1) type and duration of AF; (2) severity of symptoms; (3) presence of associated disease or reversible factors; (4) risk of thromboembolism and bleeding on anticoagulant therapy; and (5) treatment goals. A patient with a first-documented episode of AF who is haemodynamically stable does not require hospitalisation, and the assessment and initial work-up should be done on an outpatient basis.
The diagnosis and documentation of AF are possible with a 12-lead electrocardiogram or any single lead recording such as a telemetry strip, Holter or event recorder. The 12-lead electrocardiogram is also critical to ascertaining whether pre-excitation or a prior MI may have been overlooked—as well as to obtain baseline R-R, QRS and QT intervals for monitoring potential antiarrhythmic response The onset, frequency and duration of AF are fundamental to tailoring therapy and, moreover, the subsequent assessment of the degree of functional impairment brought about by the rhythm disturbance. As will be discussed in more detail, current strategies in managing AF (over and above the use of anticoagulation) do not appear to have any long-term outcome superiority with regards to mortality and are driven primarily for symptom management.6 Patients with AF have been shown to have lower quality-of-life indices compared with patients in sinus rhythm, and although still somewhat controversial, the restoration of sinus rhythm does result in an improvement in functional well-being.19–22 The choice of strategy is based not on this alone, but also on the presence or absence of underlying cardiovascular disease, and the prior use of any antiarrhythmic drugs for AF. At the initial visit, transthoracic echocardiography is also of primary importance to assess for associated valvular disease together with left and right atrial size. LV size and function is also part of the initial assessment, whereas LA thrombus should be looked for—despite the low sensitivity with this technique in a transthoracic study.6 At this visit, thyroid, renal and hepatic function should be assessed, and our practice usually also entails an assessment of rate variance/control with either a Holter or exercise test.
Reversible causes
Whether AF is being addressed as a first episode, paroxysmal (self-terminating) or recurrent (two or more episodes), a reversible cause needs to be sought. This becomes less likely when dealing with longstanding AF (longer than a year) or permanent AF, where cardioversion has failed or not been attempted. Atrial fibrillation that is reversible usually is secondary to a primary problem, and treatment of the underlying issue more often results in sustained control of this rhythm abnormality. Reversible causes include hyperthyroidism, myocarditis, pericarditis, myocardial infarction, cardiac surgery, pulmonary embolism, pneumonia, chest malignancy, excess alcohol or caffeine use, atrial septal defect, pheochromocytoma, stroke and Wolf–Parkinson–White Syndrome.
Anticoagulation
Acute anticoagulation
As mentioned above, electrical cardioversion should be used immediately if AF—with a rapid ventricular response—is deemed responsible for haemodynamic deterioration and instability. The impact of converting a fibrillating left atrium to sinus rhythm (whether electrical, pacing or antiarrhythmic drug (AAD) methods are used) leads to a degree of postcardioversion stunning—regardless of the preceding duration of AF, resulting in stasis in the LA and LAA, and the potential for systemic embolism. This mandates that all cardioversion be followed by subsequent heparinisation (intravenous bolus with an infusion to prolong the activated partial thromboplastin time (aPTT) to 1.5 to 2 times the control value until oral anticoagulation has been established with warfarin (international normalised ratio (INR)≥2.0)—and maintained at these levels for 4 weeks after the procedure. Planned cardioversion should be pre-empted by 3 weeks of therapeutic INRs (≥2.0), unless a transesophageal echocardiogram is performed to exclude a left-sided atrial thrombus. If thrombus is not detected a bolus intravenous heparin should be administered prior to cardioversion, and then followed with the combination of intravenous heparin and warfarin until therapeutic INR levels are achieved—and then maintained for 4 weeks. If an atrial clot is found, the cardioversion should be abandoned, and intravenous heparin plus oral anticoagulation initiated for at least a 4-week period be reattempting cardioversion. It is recommended that a repeat TEE prior to cardioversion be performed at this stage, given the resolution of thrombus is variable.23
Chronic antithrombotic therapy
It is likely that antithrombotic therapy may provide thromboembolic protection against other causes of stroke, yet its utility in the long-term management of chronic or paroxysmal AF remains without question22 24–26 and should be prescribed to most patients with AF (with the exception of Lone AF) (table 1). It has been repeatedly shown that both antiplatelet and vitamin-K antagonists remain vastly underutilised,27–30 and should be prescribed regardless of whether paroxysmal for >24 h or persistent/chronic. Anticoagulation with vitamin K antagonists is not without risks, and not all patients are at similar risk. In addition, not all risk factors have the same degree of association with stroke, and all these issues in addition to the risk of bleeding need consideration when initiating oral anticoagulation therapy. Each patient would need an individual assessment of their risk, and anticoagulation should be prescribed based on this—and not on whether strategy of restoring and maintaining sinus rhythm or rate-control is chosen. If sinus rhythm is restored, the potential for thromboembolism persists, as recurrences may be clinically ‘silent’ and unrecognised by the patient and physician. The seminal risk factors for stroke risk in non-valvular/non-rheumatic AF can be crystallised by the mnemonic CHADS2,31 which allocate a point for a background history of Congestive heart failure (or impaired LV systolic function (EF<35%)), Hypertension, Age≥75 and Diabetes mellitus, while a history of a prior thromboembolic Stroke will accrue 2 points (table 2). Patients with two or more points experience greater benefit in stroke prevention with vitamin K antagonists such as warfarin, than the risks of these agents, and greater benefit than with aspirin alone. It is recommended that patients with no CHADS2 risk factors (or a contraindication to warfarin, such as gastrointestinal or intracranial bleeding) be managed with 81–325 mg of aspirin daily. The patient group that falls in between these clear cut margins—those with a CHADS2 score of 1, can be managed with either warfarin or aspirin, and the decision remains clinically individualised. Warfarin should be given in all instances to maintain an international normalised ratio (INR) of 2.0–3.0, yet new data have suggested a target INR of 3.0.32 It is also important to note, however, that the efficacy of aspirin alone in the SPAF trials was modest and less consistently observed than warfarin.33 34
ACC/AHA/ESC guideline summary: antithrombotic therapy for patients with atrial fibrillation
CHADS2 score and risk of stroke
Newer agents, such as the direct thrombin and anti-XA inhibitors, are under investigation and may turn out to be more convenient and with less fluctuation in dosage than Warfarin, and this is currently the objective of several clinical trials. The disadvantages of Warfarin are well known and criticised by patients and physicians, but in practice Warfarin is highly effective in reducing stroke, and the search for an alternative is proving to be a long and difficult road.35 36
Interruption of anticoagulation for procedures
For most patients with AF, the annual incidence of clinical thromboembolism is of such a minor degree that stopping warfarin for a week to 10 days while a procedure with haemorrhagic potential is performed is generally accepted practice.6 Bridging with low-molecular-weight heparin (LMWH) or unfractionated intravenous heparin should be performed if there is a history of prior thromboembolism, left atrial thrombus or prosthetic mechanical heart valves—LMWH in the context of prosthetic valves still remains controversial.37
Clopidogrel
Although better than aspirin alone, the combination of aspirin and clopidogrel is associated with more serious bleeding,38 and not as effective as warfarin.39 The combination of warfarin, aspirin and clopidogrel is associated with higher risks of bleeding,40 and consideration should be given to using the combination of only warfarin and clopidogrel if an antiplatelet agent is necessary after intracoronary stent placement or in chronic ischaemic heart disease.41 42
Anticoagulation in older people
Older people, by virtue of the higher incidence of chronic diseases in this group—are more frequently subject to polypharmacy. Justified concerns about the potential interactions of these drugs with warfarin, and fears of falls and intracranial bleeds both contribute to significant undertreatment with vitamin K antagonists.43 44 Interestingly, the actual incidence of an intracerebral bleed is quite low in this population,45 such that an individual with AF and an average risk of stroke of 5%/year would have to fall around 300 times in a year for the bleeding risk of warfarin to outweigh its antithromboembolic benefits.45 46 It is also important to note that in older people, INRs less than 2.0 have not been shown to be associated with lower risk for intracranial haemorrhage compared with INRs between 2.0 and 3.0.47 48
Left atrial appendage occlusion
Thrombus is frequently identifiable in this chamber in those who sustain a thromboembolic stroke.49–52 Low velocities and spontaneous echo contrast53 in patients with AF are echocardiographic markers of those at higher risk of left atrial thrombus and subsequent thromboembolism.54 These findings have driven the development of device closure of the appendage as a strategy to lower thromboembolic events,55 particularly for those patients who cannot take warfarin. Studies of the PLAATO56 and WATCHMAN devices suggest less cerebral embolic events with the implant than that predicted by CHADS2 scoring or warfarin use.57 Longer-term follow-up is necessary to clarify actual risk in the community involving implantation and later events.
Cardioversion
For new-onset AF, cardioversion—using either electrical or pharmacological methods—is highly effective in the first 24 h (90% and up to 84% respectively).58 Despite this high efficacy, most patients (half to two-thirds) would have reverted to sinus rhythm without any intervention, and at 1 year up to as few as 30% of patients may still be in sinus.58 There is a much higher incidence of maintenance of sinus rhythm if a reversible cause for the AF has been addressed or if cardioversion is performed with adjunctive class I or III AAD administration.59–61 The risks with cardioversion by either means relate to thromboembolic complications (discussed separately) and bradyarrhythmias which may be unmasked by the absence of atrial dysrhythmia.62 In this regard, the pre-emptive use of a pacemaker should be considered as a temporary or permanent strategy if this is a clinical concern in a patient with a history of prior bradycardia.
Rate control versus rhythm control
Several large randomised trials have examined the merits of rhythm control over rate control.20–22 63–65 Despite the potential haemodynamic benefits of sinus rhythm, it is evident and at first glance somewhat surprising that our current strategies aimed at maintaining atrioventricular synchrony have demonstrated no survival benefit over rate control, and even in patients with heart failure.66 Importantly, anticoagulation is necessary with both approaches—with a trend towards more ischaemic stroke found in the rhythm control arms—likely due to inadequate anticoagulation. In addition, more hospital admissions and adverse drug reactions were also more common with AADs.20 22 Several caveats exist to the mantra that rate control is equivalent or superior to rhythm control (figure 1), and it is critical to recognise that most patients enrolled in the large studies referenced were mostly over the age of 65—and importantly were able to tolerate symptoms to the extent that they were amenable to randomisation. As such, patients with severe symptoms and patients with CHF or non-compliant left ventricles were under-represented in these trials. Another contributory factor is the relative inefficacy of current antiarrhythmic drugs. Hence, younger patients who develop AF have not been systematically studied, and there may be a long-term advantage to a trial of AAD therapy in this group. If there is concomitant advanced ventricular or atrial disease, this may not be feasible.
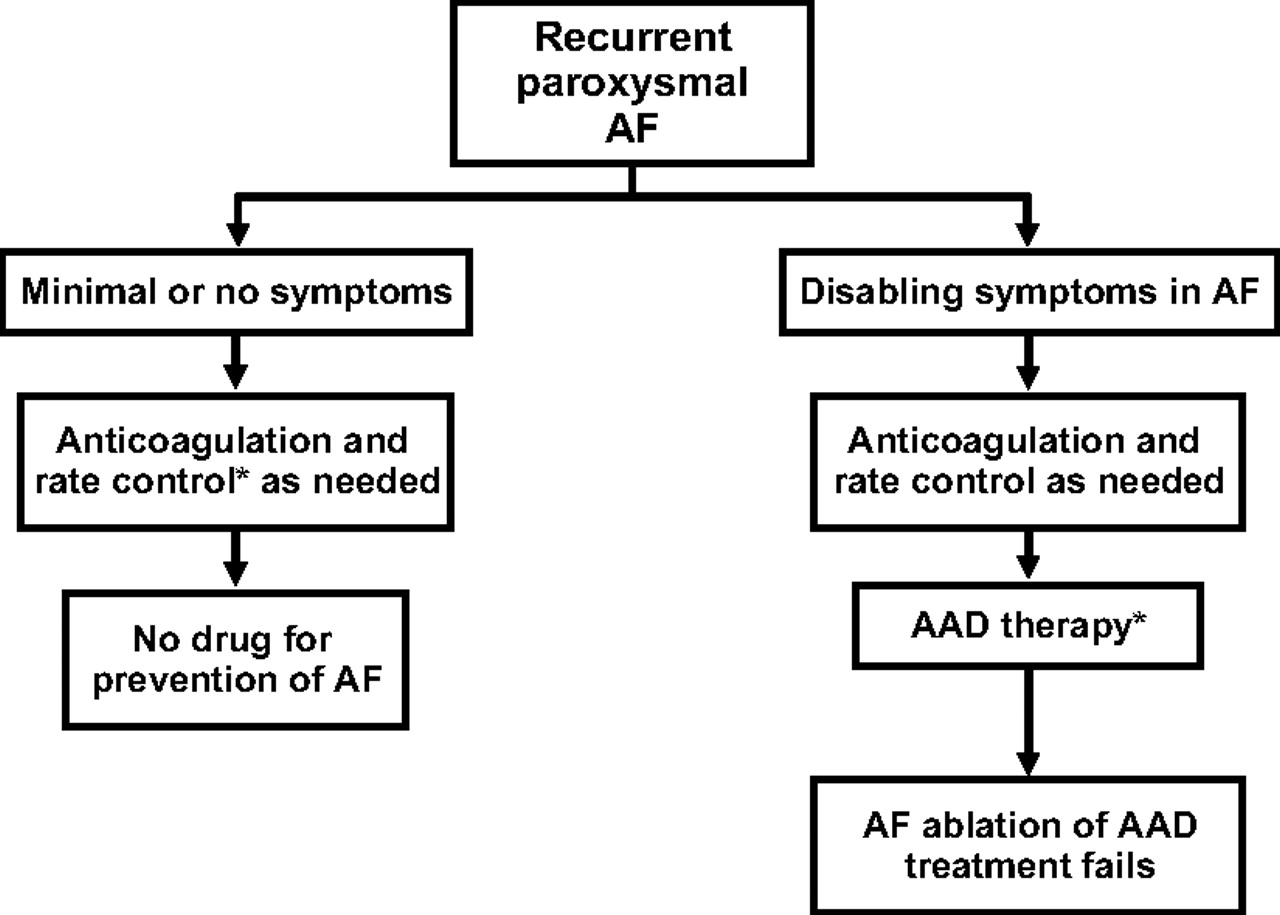
ACC/AHA/ESC guideline summary: recurrent paroxysmal atrial fibrillation. AAD, antiarrhythmic drug; AF, atrial fibrillation.
In light of these findings, there remain several main clinical situations where rhythm control may be pursued: control of symptoms; inability to control rate; patient preference and in patients with LV dysfunction in whom the development of AF resulted in haemodynamic decompensation (figure 1).
Rate control
This can be generally achieved by the use of AV nodal blocking agents such as beta-blockers, non-dihydropyridine calcium-channel blockers (diltiazem, verapamil) or a combination of the two. These two groups can be used in concert and are synergistic if utilised in that manner,67 yet the risk of significant bradycardia and heart block increases—especially in older people. Digoxin can also be used as an adjunct to this approach and, due to its rate-limiting effects being predominantly at rest, is more effective in concert with beta-blockade.68 Both digoxin and amiodarone are particularly useful intravenous rate-limiting agents in the critically ill patient, where negative inotropic effects may prove deleterious.69 Whether a policy of stricter rate-control based upon Holter or stress testing is better than a more lenient approach is the subject of the ongoing RACE II trial,70 but our policy is to maintain an average heart rate of approximately 70–80/min over a 24 h period and under 100 during the waking hours. Exercise testing to assess for excessive increases in rate, and also chronotropic incompetence may be helpful in selected patients.
Patients with symptomatic AF that is refractory to medical therapy may undergo ablation of the atrioventricular node and implantation of a permanent pacemaker to conclusively control rate.6 The survival of this group of patients appears similar to those receiving medical therapy for rate control,71 yet this approach is not ideal for all groups. Younger patients are hence exposed to the lifelong complications of permanent pacing, and patients who rely on atrioventricular synchrony are liable to have persistent symptoms after the procedure (diastolic dysfunction, congenital heart disease, hypertrophic cardiomyopathy). Another important and practical management step in the adoption of this strategy involves addressing the potential (2% risk) for sudden cardiac death in the early phase after the procedure.72 73 This appears to occur predominantly in patients with underlying heart disease, yet our approach and that of the AHA/ACC/ESC Guidelines is to programme an initially high nominal rate of around 90 beats per minute, and gradually reduce the rate over a period of 2–3 months.6
Maintenance of sinus rhythm
Antiarrhythmic therapy
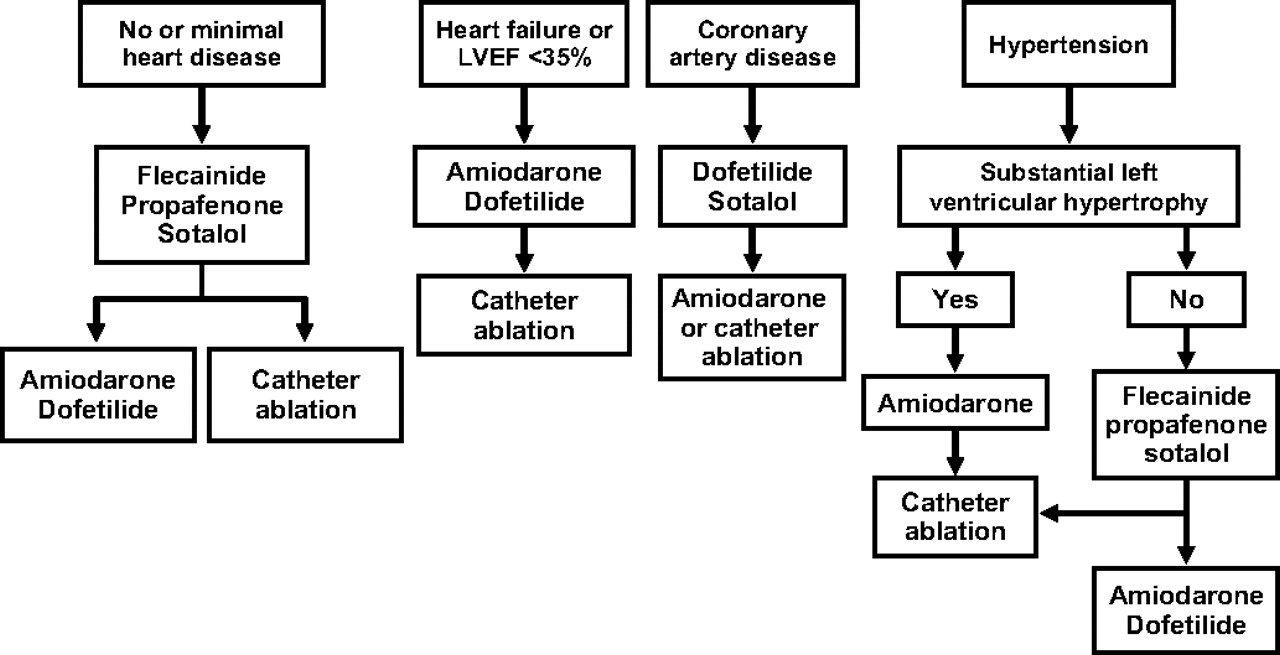
The choice of an antiarrhythmic agent is governed primarily by the underlying cardiovascular substrate and potential adverse effects of the AAD (figure 2). Amiodarone remains the most effective drug at maintaining sinus rhythm with an efficacy of 50–65% at 1 year.19 74 75 Outside its potential to block both the sinus and AV node, amiodarone confers very little pro-arrhythmic effect76 and can be used as a first line agent in patients with and without structural heart disease.6 Even with the advent of lower dose (200mg/day), therapy is frequently discontinued in light of the potential toxicities of amiodarone. Attentive follow-up on a 6 month to annual basis is clearly outlined by the Heart Rhythm Society,77 and involves routine tests of renal, hepatic, thyroid and pulmonary function, in addition to electrocardiogram and chest x-ray.

{kind=link}
{kind=link}
ACC/AHA/ESC guideline summary: antiarrhythmic drug therapy to maintain sinus rhythm in patients with recurrent paroxysmal or persistent atrial fibrillation. LVEF, left ventricular ejection fraction.
Sotalol is less effective than amiodarone, yet can be used in both organic heart disease and in those without overt evidence of cardiac disease.19 74 It is probably effective in maintaining sinus rhythm in around 50% of patients,78 and its beta blockade effects can be useful in ischaemic heart disease, especially when AF recurs—limiting the rapid ventricular response. Dofetilide also remains a first-line AAD6 in patients with and without organic heart disease—and is moderately effective from 40 to 60% depending on dose.79 This class III agent was not found to increase mortality in heart failure, yet does have a risk of Torsades de Pointes of around 3%—necessitating in-hospital initiation and mandatory prescriber training in the USA. Most provoked ventricular tachycardia episodes occur within the first 3 days.80 Dofetilide is not available in Europe, and potential drug interactions need to be thoroughly evaluated.
Dronedarone and the class IC agents (flecainide and propafenone) should not be used with underlying heart failure, as they may aggravate the disease process or promote arrhythmia.81 82 These drugs provide useful alternative strategies in managing symptomatic AF in patients without evidence of underlying heart disease. All agents appear to be less effective than amiodarone and are usually chosen based on adverse effect profile and underlying myocardial substrate. Unfortunately, the proarrhythmic effects are not negligible, and this has curbed their widespread use.83 84 Both may cause a more rapid ventricular rate by organising the AF into atrial flutter or an atrial tachycardia, and this should be considered if the patient develops progressively worsening symptoms.81
For patients with AF for less than 7 days, pharmacological cardioversion can be pursued with many of these agents. Flecainide and propafenone can similarly stabilise the atrial rhythm forming flutter with rapid atrioventricular conduction—and hence should be used with adjunctive AV nodal blockade.6 Ibutilide is only available as an intravenous preparation and is used exclusively in this setting. It should not be administered to patients with heart failure or significant myocardial disease because of the risk of inducing Torsades de Pointes (of around 4%).85 86 The procedure should be performed with full resuscitation equipment present and the patient should be monitored for 4 h thereafter.
With the exceptions of dronedarone and low-dose amiodarone, all AADs should be begun in hospital with continuous cardiac monitoring in lieu of the arrhythmic potential.6 87 Daily ECGs should be performed to assess excessive QRS (Class I agents) or QTc (Class III agents) prolongation.
Digoxin is of no proven utility in maintaining sinus rhythm and is not recommended.6 Beta blockers are used as rate-control agents but also help to maintain sinus rhythm in the occasional patient with exercise-induced AF.
Catheter ablation
Several non-atrial triggers of AF were identified in the 1990s,88 and the targeted ablation and electrical isolation of these sources have proved highly effective in addressing this arrhythmia.89 90 At 18 months’ to 2 years’ follow-up, this intervention remains effective in up to 70%. This usually improves to around 80% after a second procedure or the addition of an AAD—required in around 10–40% of patients.89 91 92 At 5 years, the efficacy does deteriorate to some degree and remains best in paroxysmal cases of AF.93
It is important to note that this procedure should not be followed by discontinuation of anticoagulation, as the incidence of late recurrence is unknown—and may go unnoticed. This procedure remains reserved in our practice for patients with highly symptomatic (particularly paroxysmal AF, who have failed other therapies, are contraindicated from other therapies or do not wish to pursue lifelong drug therapy for their rhythm problem. At this stage, no controlled data exist on any mortality or thromboembolic benefit from catheter ablation of AF, yet studies are under way to examine this relationship (CABANA—Ablation vs Drug Therapy for Atrial Fibrillation). The risks of AF ablation are not insignificant, as ablation chiefly involves ablation on the systemic side of the circulation with a 0.5–4%94 (depending on age)95 incidence of CVA and potential injury to the oesophagus, aorta and vagus nerve.94 96 97 Although more data are needed, it would appear that success rates decline with increasing duration of AF, marked left atrial enlargement and in patients with left ventricular dysfunction.
Cox maze
Prior to the advancements in the electrophysiological understanding of the venous triggers of AF, Cox and colleagues developed a surgical approach to deal with the atrial substrate that perpetuated the multiple wavelet theory behind this arrhythmia.98 Modified approaches of this procedure have proved to be the most effective therapy for this rhythm abnormality and remain widely practised as an adjunctive step to open heart surgery for coronary, valvular or congenital disease.99 The necessity for open heart surgery, however, limits its use, and it is still unclear precisely how this procedure affects atrial function in the long term.
Minimally invasive maze
Multiple modifications of the original MAZE approach using radiofrequency energy, cut-and-sew and cryoablation have been utilised by different surgical groups.100 Although able to restore sinus rhythm in over 90% of patients undergoing this procedure as lone surgery as opposed to an adjunct to concomitant procedures,101 it is rarely utilised in this context.100 It remains controversial whether effective atrial mechanical function is restored despite electrical synchrony, and is under investigation as a prophylactic strategy to pre-emptively address atrial dysrhythmias in susceptible patient groups.
Specific clinical situations
Lone AF
This term refers exclusively to those patients who have no clinical or echocardiographic evidence of cardiopulmonary disease or hypertension and are under the age of 60 years102—and identifies a group who is at low risk of thromboembolic complications. This group has little evidence of atrial disease itself, and AF appears to be primarily driven by abnormal triggers in the pulmonary and thoracic veins.89 90 Many of these patients have a genetic component to their rhythm disturbance, are young and active, and may be highly symptomatic. A minority will progress from paroxysmal or chronic AF over time,103 and the presence of Lone AF and limiting symptoms identifies the subgroup most likely to benefit from RFA. It is widely agreed that aspirin (75–325 mg/day) is adequate, as antithrombotic management and choice of rate or rhythm strategies can be based on symptomatology alone.
Patients with LV dysfunction
Left ventricular dysfunction provides a nidus for the development of AF, and as the degree of heart failure worsens so does the prevalence within this group. The presence of AF in this setting leads to symptomatic and functional deterioration and is associated with higher mortality.104 This adverse association was present in the SOLVD trial105 despite adequate rate-control and regardless of the duration and frequency of AF—fundamentally questioning whether AF simply identifies a higher-risk group among those with LV dysfunction. Fortunately, for clinicians, the optimal management of heart failure has a synergistic impact on limiting the development of AF. Through several putative cellular and haemodynamic effects, the use of angiotensin-converting-enzyme (ACE) inhibitors (ACE-i), angiotensin-receptor blockers (ARB) and β-blockers is associated with a lower but only modestly reduced risk of developing AF,106–108 but irrespective of this, these drugs are a first-line therapy for heart failure, with and without AF. As evidenced by the Euro Heart Survey on Atrial Fibrillation, and despite these observations, it appears that many patients with both the comorbidities of AF and heart failure remain inadequately treated—with only 32% of eligible patients receiving the full complement of an ARB/ACE-I, β-blocker, oral anticoagulant combination.109 Calcium-channel antagonists should be used with caution for rate control in this group, because of the potentially negative impact on myocardial function,106 and digoxin remains an appropriate adjunctive medication, particularly in decompensated patients—favourably impacting both inotropism and rate control.6 The addition of an antiarrhythmic medication to this basic regimen has been widely shown in subgroup analyses to reduce hospital admissions80 110 and even to improve symptoms19—yet concurrent improvements in mortality are not apparent. The lack of mortality benefit was confirmed in the large randomised AF-CHF trial, which also demonstrated no impact on heart failure or stroke.66 Patients with severely decompensated heart failure may, however, benefit acutely from the off-label use of intravenous amiodarone as a temporising rate-control measure—usually via the intravenous route.69 Together with the not-insignificant potential pro-arrhythmic hazards, the AADs remain fairly poor at maintaining sinus rhythm,80 with the newer-generation AAD (Dronedarone) aggravating heart failure.82 Hence, it appears that this strategy should be reserved for those that fail rate-control—with amiodarone, sotalol or dofetilide being the drugs of first choice.
Postsurgical AF
Cardiac surgery leads to the development of AF in 20–50% of patients in the early postoperative phase (usually beginning day 2–5) and terminating in 90% of patients by the second month after the procedure. Perioperative AF has been shown to increase hospital stay and the risk of stroke. This common postoperative arrhythmia has been shown to be modestly reduced in its frequency by maintenance of or initiation of perioperative beta-blockade.111 112 In addition, the risk of AF in this setting can potentially be managed by prophylactic amiodarone or sotalol.113 Alternatively, biatrial pacing in the immediate postoperative period has also been shown to mitigate against the development of AF.114 Since the arrhythmia is generally self-limiting in the majority, a strategy of rate control and short-term anticoagulation is widely used. Whatever strategy is chosen, reassessment at 2–3 months postoperatively would be recommended, as the inflammatory milieu has dissipated.
Pregnancy
AF in this group rarely occurs outside the setting of congenital heart disease or native or prosthetic valvular disease, especially mitral stenosis, and as a result there may be additional reasons for mandatory anticoagulation. Low-molecular-weight heparin has not been studied, and it is recommended that unfractionated heparin be used either intravenously or subcutaneously to prolong the aPTT by 1.5–2-fold normal. Exposure to warfarin in the first and last trimesters may result in teratogenicity or fetal haemorrhage respectively; warfarin can be used in the middle trimester.115 116 All antiarrhythmic drugs cross to the fetus and should only be prescribed if necessary to maintain haemodynamic stability. Rate control can be safely achieved with digoxin, a β blocker, or a non-dihydropyridine calcium-channel blocker. Cardioversion in the context of acute haemodynamic embarrassment is safe and also recommended.6
Hypertrophic cardiomyopathy
Thromboembolic complications appear to be more frequent in those patients with AF and with the additional burden of hypertrophic cardiomyopathy.117 We strongly recommend routine warfarin anticoagulation regardless of CHADS2 risk stratification. In addition, this patient group tolerates this atrial dysrhythmia poorly from a clinical standpoint—putatively with the need for atrioventricular synchrony because of higher filling pressures.117 Hence, the maintenance of sinus rhythm can potentially ameliorate the haemodynamic compromise118 and should be more aggressively targeted in this group.6 Somewhat surprisingly, reasonable success rates have been reported with RFA.119 In patients undergoing surgical myectomy, an adjunctive Maze procedure can be considered, although long-term effects of left atrial function are lacking.
Accessory pathways
Wolf–Parkinson–White also deserves a separate mention in that its management is slightly different from other reversible causes. It is a Class I AHA/ACC/ESC recommendation to proceed to radio-frequency ablation of the accessory pathway if symptomatic AF develops in this context. This is done primarily to ward of the rare event of AF promoting ventricular fibrillation. Interestingly, the disruption of the pathway also reduces the incidence of AF in the future, and it is postulated that the atrial dysrhythmia results from degeneration of an initial supraventricular tachycardia. In the event that AF recurs following pathway ablation, this facilitates the use of more conventional agents for the management of the atrial dysrhythmia.120 The acute management of AF with a wide and rapid ventricular response should involve cardioversion if haemodynamically unstable but, as importantly, should not involve the use of AV-nodal-blocking agents to gain control of the rate. This may cause preferential blockade of the node and thereby accelerate the ventricular rate. (More rapid conduction down the pathway can potentially develop in light of its non-decremental and shorter refractory properties.) Intravenous procainamide, ibutilide or amiodarone can be administered in this context of WPW, which is haemodynamically stable.6
Congenital heart disease
The lack of sinus rhythm in this population is poorly tolerated from a haemodynamic and symptomatic point of view—with AF or flutter being a primary cause of morbidity and hospital admission.121–123 Hence, the achievement of sinus rhythm with either drug or ablative therapies is very often given higher priority than rate-control alone, although these success rates are often suboptimal due to the underlying disease substrate involving ventricles and atria. The clinician should be acutely aware that atrial dysrhythmias in congenital heart disease may be an early harbinger of deteriorating haemodynamics, such as a failing Fontan circulation. Patients with a prior atriotomy may present with an atypical atrial flutter—most commonly an intra-atrial re-entrant tachycardia—which is scar-mediated and amenable to ablation.
Rheumatic heart disease
A history of rheumatic mitral disease places patients at increased risk for thromboembolic complications by up to 17-fold,16 and the CHADS2 score is not applicable. These patients should routinely receive warfarin if AF is to develop.124 To prolong the diastolic filling period in those with mitral stenosis, treatment of AF should be aimed at heart-rate control with β blockers as first-line agents.125
Atrial flutter
Patients with atrial flutter retain the same thromboembolic risk as those with AF or both, and should be treated similarly—based on their individual CHADS2 risk scores and clinical background. Typical/classical atrial flutter is evident on the 12-lead ECG as a saw-tooth pattern, with the flutter or F waves being dominantly negative in leads II, III and aVF, without an isoelectric baseline, and positive in lead V1. This arrhythmia is driven by a macro-re-entry circuit anticlockwise around the right atrium and involves the tissue of the cavo-tricuspid isthmus. The slower atrial rates give a greater opportunity for AV node recovery, and subsequently may be more difficult to rate-control than AF. Also, although these two atrial dysrhythmias most commonly coexist in the same individual, radiofrequency catheter ablation has emerged as a safe and effective first-line treatment for typical atrial flutter.126 In this group, focused atrial flutter ablation may be successful, yet the recurrence of AF is around 50%.127
In summary, AF is a major public health problem, and its management provides a challenging clinical dilemma that requires a thorough knowledge of the patient and an individualised approach. Advances in our understanding of medical and catheter-based approaches have vastly altered the treatment approach over the last decade, and this review serves as an update in contemporary and practical management.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.