Article Text

Abstract
Objective To assess the sex difference in hospital mortality following ST elevation myocardial infarction (STEMI) in China.
Design Observational study of patients enrolled into a large trial, adjusting for age, presenting characteristics and hospital treatments using logistic regression.
Settings 1250 hospitals in China during 1999–2005.
Patients 42 683 STEMI patients, including 31 309 men and 11 374 women.
Intervention In the original trial, all patients received 162 mg of aspirin plus 75 mg of clopidogrel daily or matching placebo and metoprolol (15 mg intravenous then 200 mg oral daily) or matching placebo. All other aspects of patients' treatments were at the discretion of responsible doctors.
Major outcomes Hospital mortality from any cause during the scheduled trial treatment period (ie, up to 4 weeks in hospital).
Results Overall, 8% of the patients died in hospital, with the crude hospital mortality being twice as high in women as in men (12.6% vs 6.3%). After adjusting for age, the sex difference in hospital mortality attenuated but remained highly significant (OR 1.54; 95% CI 1.43 to 1.66). Further adjustment for other baseline characteristics and for the treatments given in hospital had little effect on the sex difference in hospital mortality (OR 1.50, 95% CI 1.38 to 1.62). The difference in hospital mortality was greater at a younger age, with the adjusted ORs being 2.14, 1.70, 1.48 and 1.18, respectively, for ages <55, 55–64, 65–74 and ≥75 years (p=0.0001 for trend).
Conclusion Compared with men of the same age, women had approximately a 50% higher mortality following hospital admission for STEMI, with a particularly higher excess risk at age <55 years.
- Coronary artery disease
- gender
- STEMI
Statistics from Altmetric.com
Introduction
In recent decades, population mortalities from ischaemic heart disease (IHD) have been declining in many Western countries such as the USA as a result of risk modification and advances in medical therapies.1 In China, IHD now accounts for more than 700 000 deaths each year,2 and population mortalities in some cities are approaching those in Western populations.3
Both in China and elsewhere, women are relatively protected against cardiovascular disease, with population mortality in middle age less than half that in men.1 2 Despite this, early hospital mortality following admission for an episode of acute myocardial infarction (MI) (ie, the case death rate) is higher in women than in men of a similar age.4–9 Some studies have attributed this to higher rates of comorbidity (eg, diabetes, hypertension and prior congestive heart failure) among women,10 11 whereas other studies have concluded that underuse of effective treatments in hospital (eg, revascularisation procedures) is an important cause.12–17 However, in some registry studies,4 10 14 18 the poor survival among women after acute MI was more striking at younger than at older ages, and persisted after adjustment for age, and for recorded disease severity and access to treatments.
Thus, there is evidence that women treated similarly for acute MI differ from men in several other important ways.6 19 20 Most of the previous studies of the relevance of sex were in Western countries. There is relatively little evidence about the relevance of sex to prognosis following hospitalisation for acute MI in developing countries such as China, where disease-onset rates and access to effective care differ significantly from Western populations.1 2 We examine the sex differences in early mortality following acute MI in a large study of 45 852 well-documented patients enrolled in COMMIT/CCS-2 study from 1250 hospitals throughout China, including 12 759 women and 33 093 men.21–23
Methods
Study population
The study population was all patients enrolled in COMMIT/CCS-2, a large placebo-controlled trial of the effects of dual antiplatelet therapy and of early beta-blocker in patients with suspected acute MI (ClinicalTrials.gov registration number NCT00222573).22 23 Before the start of the study, approval was obtained in writing from the Chinese Ministry of Health, the Chinese State Food and Drug Administration and the central ethics committee of the Chinese Academy of Medical Sciences. All collaborating hospitals also obtained approval from a local ethics committee or institutional research review board. In brief, 45 852 patients admitted to hospital within 24 h of onset of symptoms and/or signs of suspected acute MI and with definite ST-segment changes were enrolled into the study during 1999–2005. There was no upper age limit and, apart from randomised study treatments (clopidogrel/placebo and metoprolol/placebo) and background treatments of all patients with daily aspirin 162 mg, all aspects of patient management were at the discretion of the patient's own doctors. The study treatments started immediately after randomisation and continued for 4 weeks in hospital (or until prior discharge or death). After discharge from hospital, no further long-term follow-up was carried out. Overall, 1250 hospitals in 30 provinces of China participated in the study, 18% tier III (teaching or provincial hospital), 57% tier II (medium-sized city hospital) and 25% tier I (small county or district hospital).
Baseline characteristics
At randomisation, information was recorded on the entry form including sex, date of birth, prior history of disease, medication before symptom onset, hours since symptom onset, treatment already given after hospital admission (eg, fibrinolytic therapy) and current clinical characteristics (eg, blood pressure, heart rate, Killip class, ECG abnormalities). For each randomised patient, a diagnostic ECG was to be collected and sent to the study coordinating centre in Beijing for blinded review and verification. After entry into the study, information about the use of non-study treatments during hospitalisation was reported on the follow-up form.
Outcome measures
At hospital discharge (or death without discharge), the follow-up form recorded any major clinical events (such as death, reinfarction, stroke, heart failure, severe arrhythmia and pulmonary embolus) during hospitalisation, and these were investigated in more detail. Information was also collected about less specific adverse events (eg, bleeding, persistent hypotension and bradycardia). For the present analysis, the main outcome measure is death in hospital. In addition, we analyse a composite outcome of major vascular event (MVE), defined as death, non-fatal reinfarction or stroke (including both ischaemic and haemorrhagic stroke). Various other adverse events were also compared between women and men.
Statistical analysis
Means and prevalence were adjusted to the overall mean baseline age (61.3 years) using logistic or linear regression. Rates of adverse events in hospital were compared between women and men using logistic regression, yielding the OR and its 95% CI. Three different models were fitted: (a) without any adjustment; (b) adjusted for baseline age; and (c) adjusted for all baseline characteristics (as listed in table 1) and drug use prior to hospitalisation. Study treatments were not considered in the models because all patients enrolled received either the active drug or the placebo, and they were evenly distributed across sexes by randomisation.22 23 Apart from four continuous covariates (age at entry, systolic blood pressure, heart rate and time delay since disease onset), all variables were categorical or binary. Preliminary analyses indicated that non-linear terms for age and systolic blood pressure were required, so for these two variables quadratic and cubic terms were also included. Potential heterogeneity in the ratio of the female and male rate was analysed in various subgroups, using Wald t tests for interaction (and using 99% CI for the subgroup-specific death rate ratios to limit the effects of multiple comparisons). Analyses were carried out using SAS v 9.1.
Baseline characteristics among 12 759 women and 33 093 men
Results
Of 45 852 patients, 12 759 (27.8%) were women, and 33 093 (72.2%) were men. Their baseline characteristics are described in table 1. Women were significantly older than men (mean: 66.6 vs 59.3 years) and, after standardising for age, had a longer delay between symptom onset and admission, had a higher blood pressure and faster heart rate, and had a greater prevalence of ST depression and heart failure. Both aspirin and fibrinolytic therapies had been used somewhat less in women than in men, even after restricting the analysis to participants admitted within 13 h of symptom onset. During their stay in hospital, women were less likely to be given antiarrhythmic agents and angiotensin-converting enzyme inhibitors but more likely to be given diuretics (table 2).
In-hospital drug use among 12 759 women and 33 093 men
Overall there were more women diagnosed as having non-ST elevation MI or unstable angina (10.9% vs 5.4%). To increase the comparability of the male and female case series, our main analysis is of the 42 683 (93.1%) participants with confirmed ST-segment elevation myocardial infarction (STEMI), thus excluding 1784 men and 1385 women with other types of MI or with unstable angina.
Overall, 8% of patients who presented with confirmed STEMI died in hospital, and the death rate was twice as high in women (12.6%) as in men (6.3%). After adjustment for age, the sex difference in mortality was attenuated but remained highly significant (age-adjusted OR 1.54, 95% CI 1.43 to 1.66; table 3). Further adjustment for other baseline variables had little effect on this sex difference in mortality (fully adjusted OR 1.50, 95% CI 1.38 to 1.62). Compared with men, women also had a significantly increased risk of having an MVE, defined as death, reinfarction or stroke (fully adjusted OR 1.38; 95% CI 1.28 to 1.48; table 3). Women also had significantly more cardiogenic shock (fully adjusted OR 1.27; 95% CI 1.15 to 1.41; table 3) and presumed cardiac rupture (fully adjusted OR 1.94; 95% CI 1.59 to 2.37; table 3). There was, however, no evidence of excess risk among women of non-fatal reinfarction (fully adjusted OR 0.95, 95% CI 0.78 to 1.15), non-fatal stroke (fully adjusted OR 0.90, 95% CI 0.68 to 1.18) or heart failure (fully adjusted OR 1.05, 95% CI 0.98 to 1.12). Major non-cerebral bleeding was also lower in women (fully adjusted OR 0.75, 95% CI 0.51 to 1.10; table 3).
Comparison of early outcomes among 11 374 women and 31 309 men with acute ST elevation myocardial infarction (including bundle branch block) before and after adjustment for age and other variables
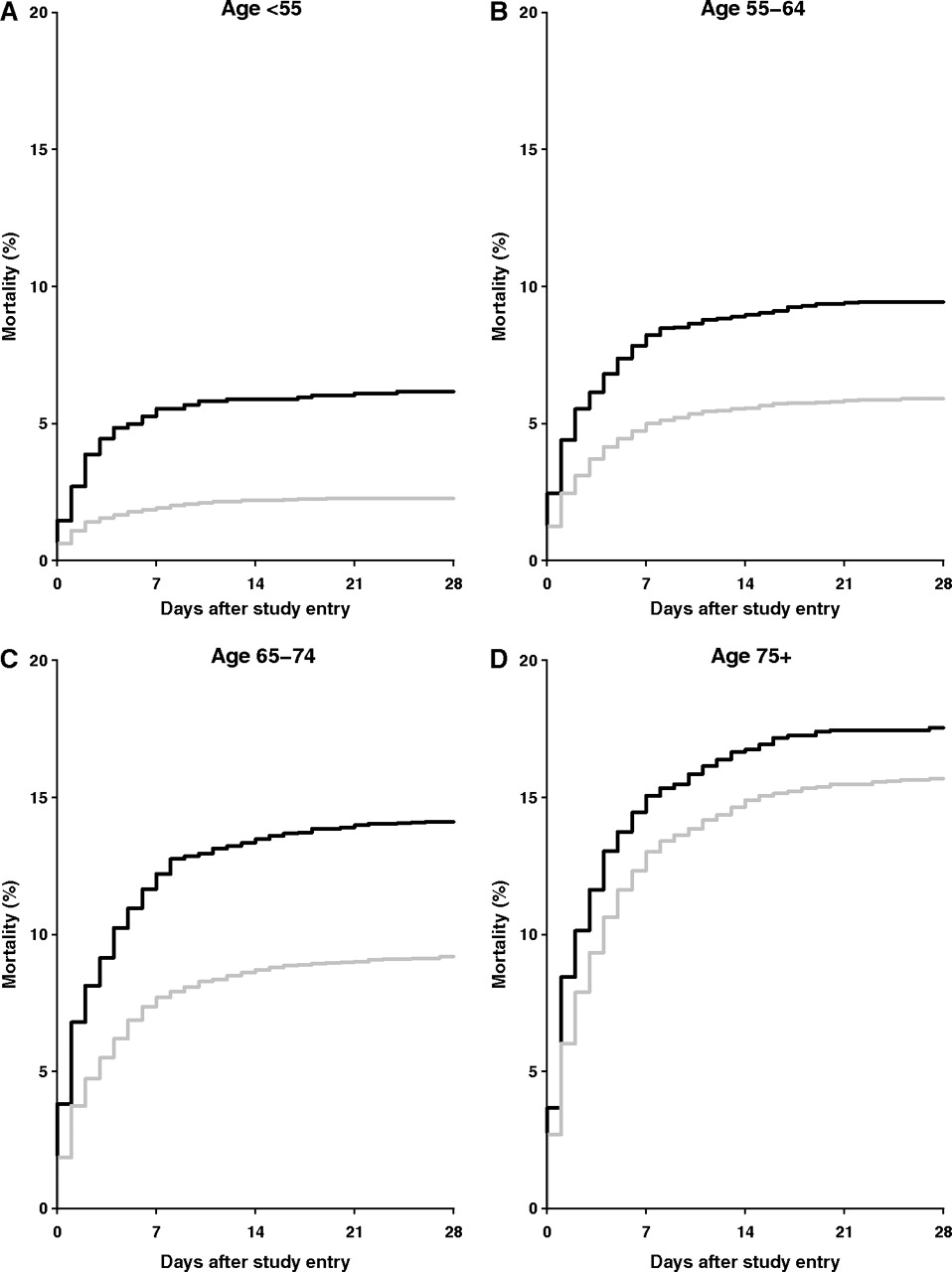
In both women and men, the absolute risk of death increased with age, but the sex mortality ratio decreased with age (figure 1), with the adjusted ORs being 2.14, 1.70, 1.48 and 1.18, respectively, for ages <55, 55–64, 65–74 and >75 years (p=0.0001 for trend test: figure 2). The excess mortality was the greatest in the first 24 h after admission (adjusted OR 1.76, 99% CI 1.52 to 2.04) and was non-significant during days 8–28 after admission (adjusted OR 1.17, 99% CI 0.91 to 1.50; p<0.0001 for trend test: figure 2). Among survivors, there was little difference in average length of hospital stay between women and men (mean: 15 vs 16 days). By the end of 28 days, only a very small proportion of surviving patients remained in hospital (7% in women and 9% in men). Among patients presenting with anterior MI, the mortality difference between women and men appeared to be more pronounced (adjusted OR 1.68, 99% CI 1.47 to 1.92) compared with infarct at other sites (adjusted OR 1.30, 99% CI 1.09 to 1.54; p=0.004 for interaction: figure 2). Apparent heterogeneities in sex mortality difference were also found with respect to Killip class (p<0.0001 for interaction: figure 2), heart rate at admission (p<0.0001 for interaction: figure 2) and prior history of MI (p=0.01 for interaction: figure 2). For these, the excess mortality in women was less extreme in those with a higher Killip class or who had had a previous MI at admission (figure 2). There was no evidence of apparent heterogeneity in sex mortality difference across different types of hospital. Further adjustment for the treatment given in hospital did not attenuate the sex difference in early mortality (fully adjusted OR 1.53, 95% CI 1.41 to 1.66).
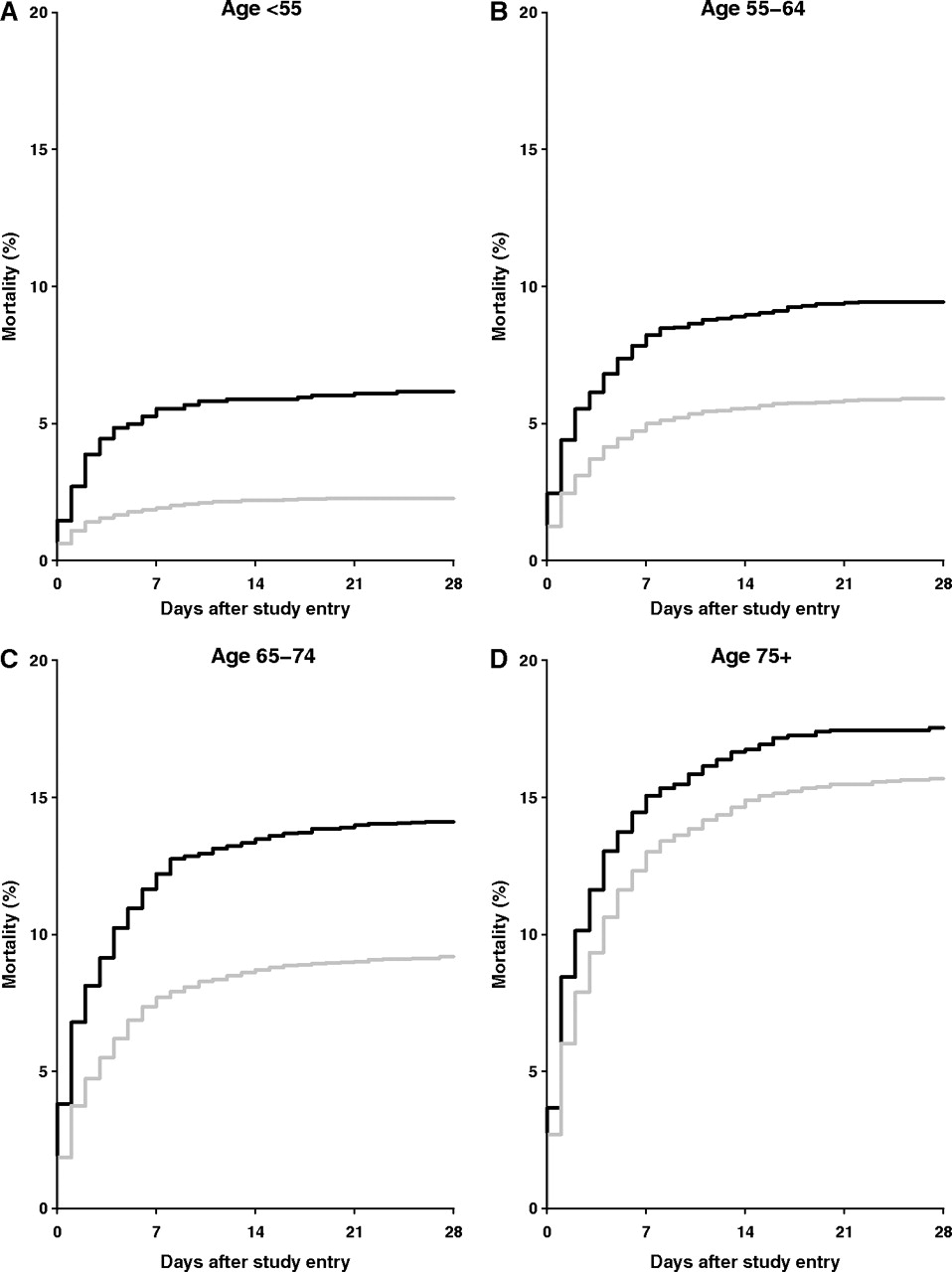
Kaplan–Meier plots of the cumulative probability of death in hospital within 28 days of admission for acute MI by age, in women (black lines) and men (grey lines). The time-to-event analysis was based on the first relevant event during the scheduled treatment period. The mean treatment duration in survivors was 15 days in women and 16 days in men. The flatness of the right-hand ends of the graph is because events after discharge were not included.

{kind=link}
{kind=link}
Adjusted ORs for death during the first 28 days of hospitalisation after acute myocardial infarction (MI), in women compared with men. ORs were adjusted for age and other baseline variables. Black squares represent the OR in each subgroup (with area inversely proportional to its variance) and 99% CI (horizontal line). The dotted line and diamond represent the overall OR and its 95% CI. SBP, systolic blood pressure.
For patients presenting with ST depression, there was, if anything, a lower mortality in women (adjusted OR 0.66, 99% CI 0.43 to 1.00), although the number of deaths involved (173 deaths) was extremely small (69 women and 104 men).
Discussion
This large nationwide study found that the risk of dying in hospital after admission for acute MI was about twice as high in women as in men. About half of that excess mortality in women could be attributed to age, but the residual excess risk could not be accounted for by age, other presenting characteristics and access to treatments. The difference in early mortality between women and men was particularly large at younger ages and during the first few days of hospitalisation. Although the present study is based on the data from a randomised trial, the entry criteria was very broad22 23 and it involved more than 1000 specialist and non-specialist hospitals throughout China so the findings should reflect real clinical settings.
Several studies in other populations have reported on the sex difference in early mortality following an acute MI. They ranged in design from hospital cases from national registries5 10 13 18 24 to large multicentre trials6 8 11 12 with varying selection criteria. Despite these large differences, most studies tended to show consistently that early hospital mortality is significantly elevated in women.6 8 10–12 18 24 25 A few studies have reported that the excess risk among women could be attributed almost entirely to advanced age of women,8 whereas others have reported that it cannot, even after adjustment for age and other baseline characteristics.6 7 11 18 24 A few studies have also suggested that the difference in access to effective acute care (eg, revascularisation procedures12–14 between men and women could contribute substantially to the sex difference in survival prognosis after acute MI. In the present study, patients who underwent primary PCI or CABG were excluded as part of the eligibility criteria, and even after study entry the use of elective revascularisation procedures was extremely rare in China between 2000 and 2004. As part of the study treatments, there was no difference between women and men in the use of antiplatelet therapy and beta-blocker therapy; nor was there any difference in compliance of the study treatments between women and men.22 23 Moreover, a sex-specific meta-analysis of all clopidogrel trials including COMMIT has found no differences in relative efficacy and safety of clopidogrel in women and men.26 The fully adjusted OR was not attenuated after adjustment for the differences in the use of other effective hospital treatments (such as fibrinolytic therapy and angiotensin-converting enzyme inhibitors).
In the present study, the excess mortality among women was greatest in those with anterior STEMI. There was, if anything, a lower mortality among women with NSTEMI, but the number of deaths involved was small. As in the present study, a few previous studies have also found that the sex difference in mortality was much more pronounced at a younger age than at an older age.5 10 14 18 24 The reasons for this apparent interaction with age are unclear: it cannot be explained by a difference in the prevalence of other conditions such as diabetes, heart failure or previous stroke. One recent study has reported a reduction since 1994 in the sex difference in early mortality and has attributed this to a general reduction in disease severity among hospitalised patients.5 In the present study, the information on prior disease history is limited, so the question cannot be examined fully. However, in contrast with previous claims,18 27 28 the sex difference in the present study was more pronounced among patients without heart failure (ie, Killip class I) than among those with it.
As with most previous studies, the present study was hospital-based rather than community-based, so it is not known how its findings are affected by differences between men and women in whether they seek emergency care after disease onset, and how late they arrive in hospital. Data from population-based disease registry studies show that many heart attack patients die before ever reaching hospital,1 so they are not represented in hospital-based series; likewise, many patients with an infarct that is not severe may never go to hospital, and if this is more true of women than of men, it could account for some of the higher in-hospital mortality among those who do reach hospital. (An obscure sex-related difference is that the ratio of shortness of breath to pain on the presenting symptoms is higher in women than in men.)29 Differences between men and women in symptoms, hospitalisation and outcome could be attributable to both non-biological and biological factors. It is, however, difficult to believe that non-biological factors alone could account for the extreme mortality difference at younger ages (figure 1); thus, biological factors are likely to be involved, but it is not known what they are, although women tend to have smaller and stiffer blood vessels than men,30 and there is evidence that oestrogen can decrease plasma levels of fibrinogen, antithrombin, protein S and plasminogen activator inhibitor.31
In the present study, the sex difference in early mortality is greater than in many other populations.6 8 10–12 18 24 25 For instance, in an overview of 11 clinical trials of various treatments for acute coronary syndrome,6 the sex mortality ratio was 1.2 after adjustment for many factors, while in the present study it was 1.5. This difference could be due chiefly to the residual differences between baseline characteristics of the women and men that cannot be adjusted fully. For instance, random errors in the measurement of the baseline characteristics may lead to systemic underadjustment for the differences in those characteristics (ie, regression-dilution bias).32 Also, some important prognostic factors that were not recorded at the time are not adjusted at all in the present study. Although we lacked information on various baseline factors such as angiographic disease severity, diabetes and BMI, perhaps our main limitation is that we did not have any information on smoking, which in China is far more common in men than in women.33 There is evidence from clinical studies that smokers tend to have a better survival prognosis following MI compared with non-smokers.34 A nationwide blood-based prospective study in 300 000 women and 200 000 men is, however, now in progress in China that is monitoring both hospitalisation and deaths from heart disease,35 and over the next few years, this will help clarify many of the remaining uncertainties about the large, and still unexplained, difference between men and women in the case-fatality rate of acute MI.
In summary, the present study in China has confirmed that following onset of acute MI, women have a worse survival prognosis compared with men. Although this apparent sex difference in prognosis could not be attributed entirely to potential confounding by age or other baseline characteristics, it is still possible that some of this difference could still be due to residual confounding by disease severity or other baseline characteristics. With an ageing population and rapid change of lifestyle and dietary patterns, the mortality from IHD in China is likely to increase further over the next few decades. Despite recent improvements in the general care of patients with acute MI in China, there is still substantial under-, over- and inappropriate treatment of many patients with MI in China, with large variations in management among different hospitals and regions. Further improvements will rely not only on better implementation of the established cost-effective treatments but also on better awareness of the risk profile in the general population and more targeted management of high-risk patients including women.
References
Footnotes
Funding The original trial was funded by Sanifo-Aventis and AstraZeneca. It was, however, designed, conducted, analysed and interpreted independently of the companies, in collaboration between the Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU) and Fuwai Hospital. The present report is supported only by the core funding to the CTSU from the UK Medical Research Council and British Heart Foundation. CTSU has a staff policy of not accepting honoraria or other payments from pharmaceutical industry, except for the reimbursement of costs to participate in scientific meetings.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Chinese Academy of Medical Sciences, Fuwai Hospital.
Provenance and peer review Not commissioned; internally peer reviewed.