Article Text

Statistics from Altmetric.com
- Cardiac imaging
- echocardiography (three-dimensional)
- echocardiography (transoesophageal)
- thromboembolism
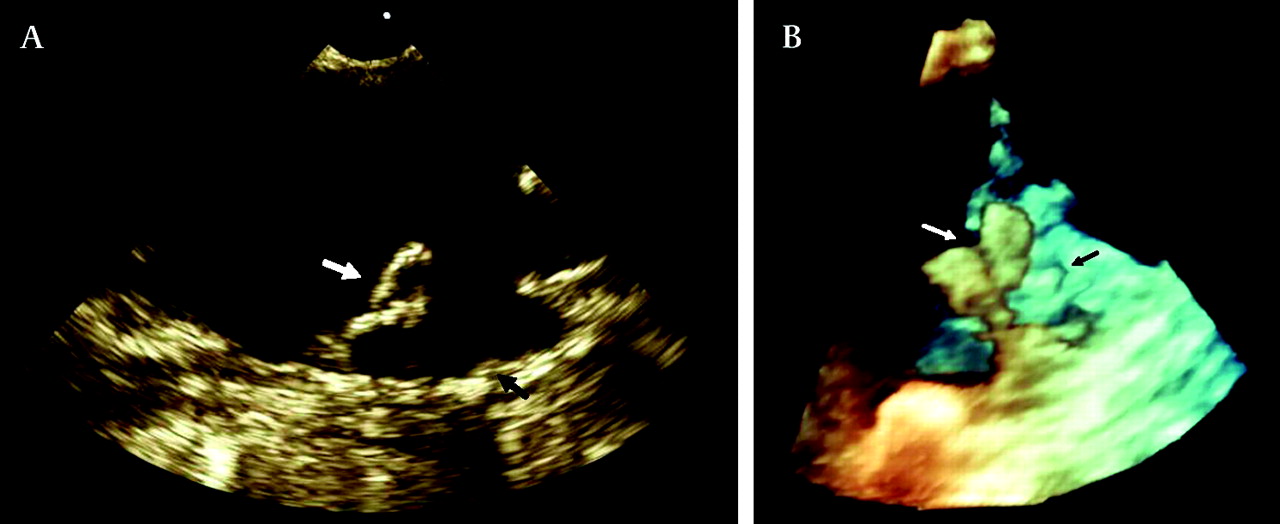
A 68-year-old man with previous multiple transient ischaemic attacks presented with 3 days of worsening abdominal pain and subsequently developed septic shock. An emergency laparotomy revealed a perforated small intestine secondary to infarction of the terminal ileum. Transthoracic echocardiography showed normal left ventricular systolic function during sinus rhythm, satisfactory valvular function, no evidence of intracardiac thrombus and no interatrial shunting on colour Doppler analysis or with agitated saline contrast study. Transoesophageal (TOE) two-dimensional (figure 1A) and three-dimensional (figure 1B) echocardiography demonstrated extensive, severe distal aortic arch and descending thoracic aortic atheroma (black arrow). A large, mobile protuberant bilobed atherothrombus measuring 1.4 cm (white arrow) was identified in the distal descending thoracic aorta (video 1). Pathological examination confirmed small bowel infarction secondary to atheromatous emboli.

{kind=link}
Two-dimensional (A) and three-dimensional (B) transoesophageal echocardiography demonstrating a large, mobile bilobed atherothrombus in the distal descending thoracic aorta with extensive distal aortic arch and descending thoracic aortic atheroma.
Comprehensive TOE with attention to the thoracic aorta should be considered for patients with acute bowel ischaemia, despite negative results on transthoracic echocardiography. Two-dimensional TOE with high frequency multiplane probe may evaluate size, location and mobility of the thrombus as well as visualise intimal thickness of the thoracic aorta. Real-time three-dimensional (3D) TOE facilitates the spatial definition of complex aortic atherothrombus as well as imaging the atheromatous surface, which may have implications for planning surgical excision. This modality can be performed at the bedside with rapidly available results, which is especially important in unstable patients who may be intubated and unable to tolerate transfer for computed tomography (CT) or magnetic resonance imaging. Mobile thoracic aortic thrombus diagnosed with TOE may not necessarily be readily visible on conventional angiograms or CT scanning.1 TOE may also be used for serial monitoring after treatment, particularly for thrombus recurrence.
Management of atherosclerotic aortic thrombi is not well established. Treatment should be based on the nature and aetiology of the thrombus. Options include thrombolysis and anticoagulation with Warfarin; however, the risk of partial lysis, haemorrhage and further distal embolisation, especially from thrombi which have a friable appearance, must be considered.2 3 Surgical thrombectomy1 and thoracic aortic stent graft placement via an endovascular approach have been described.4
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; not externally peer reviewed.