Article Text

Statistics from Altmetric.com
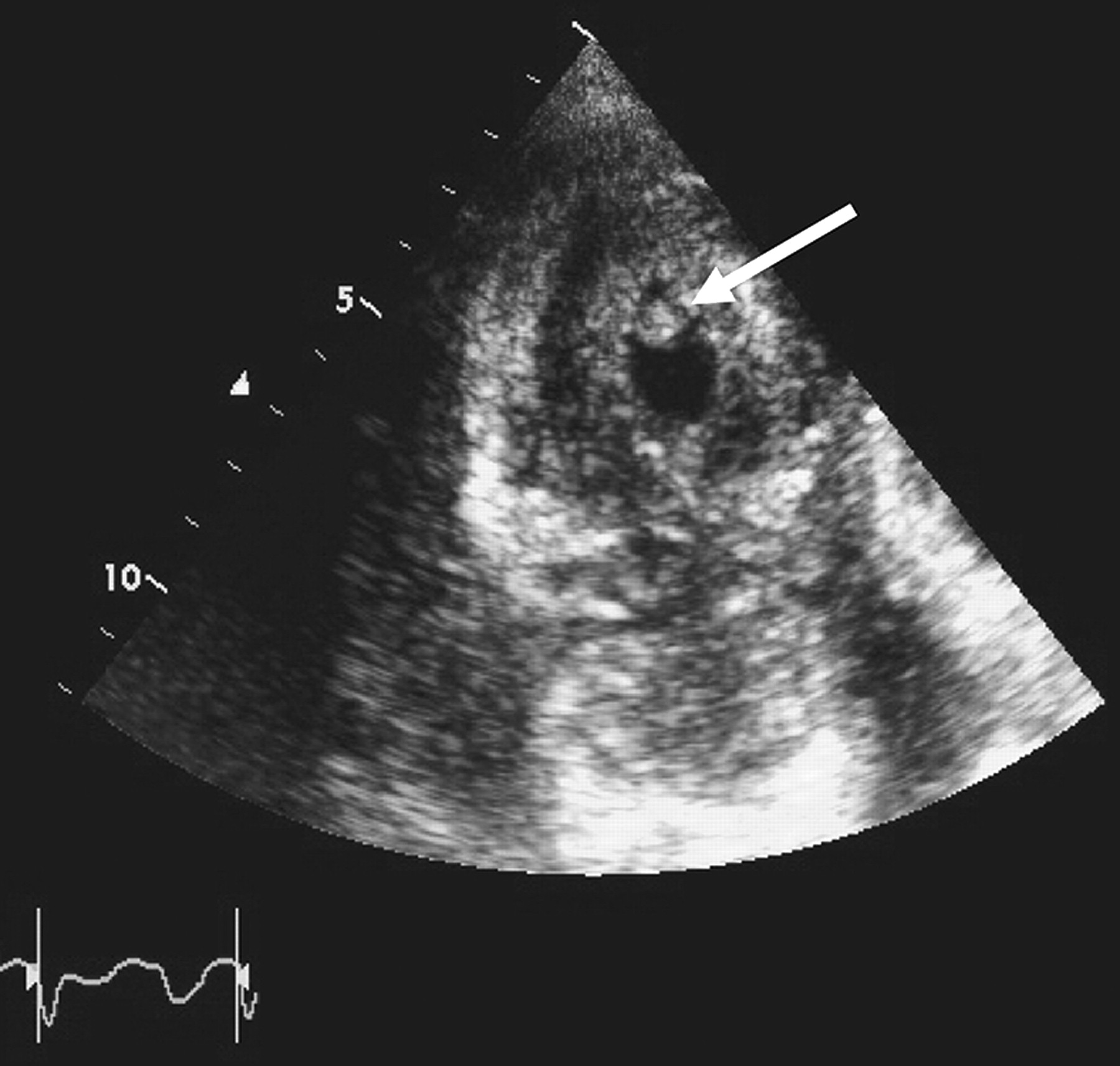
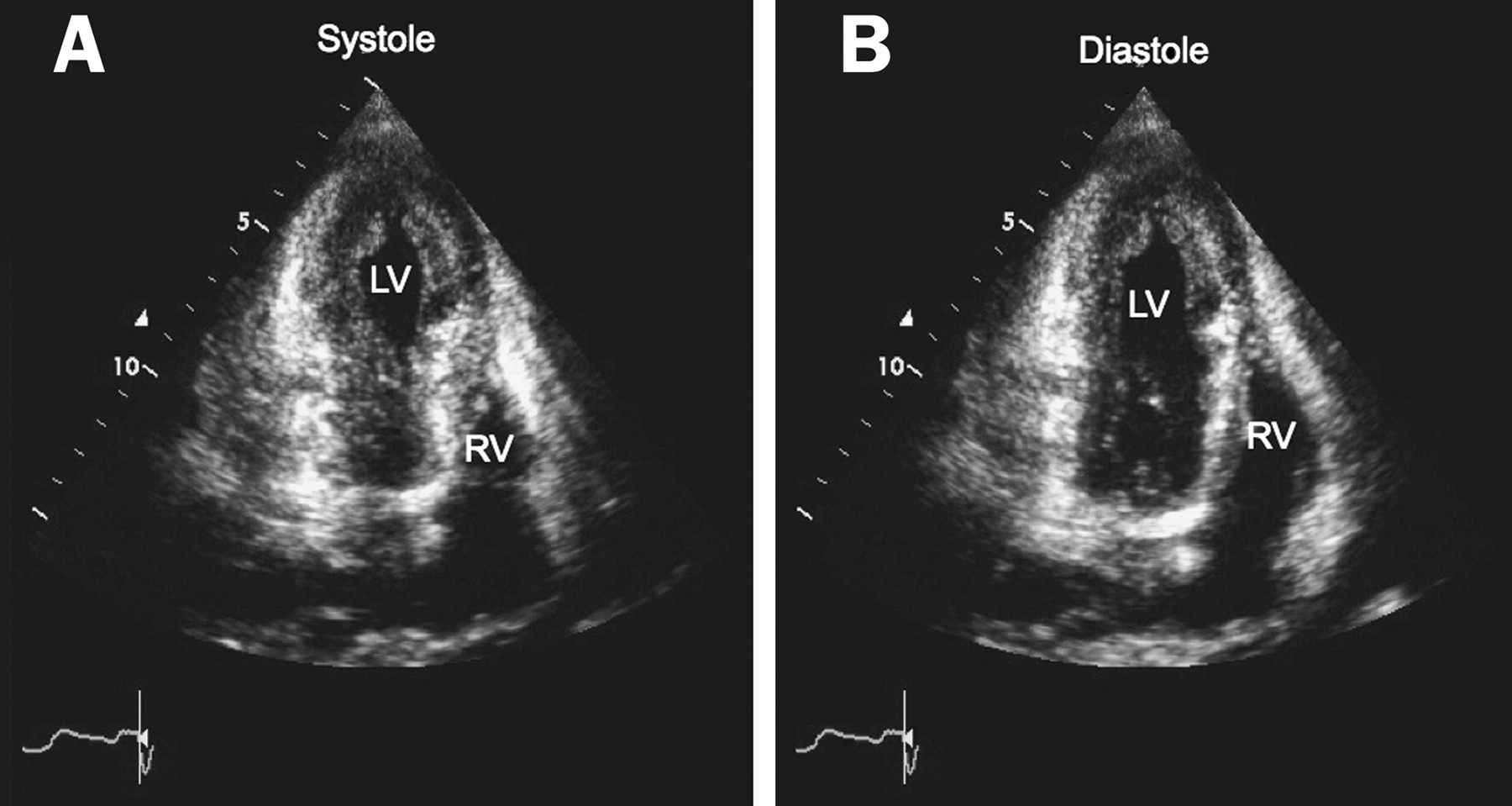
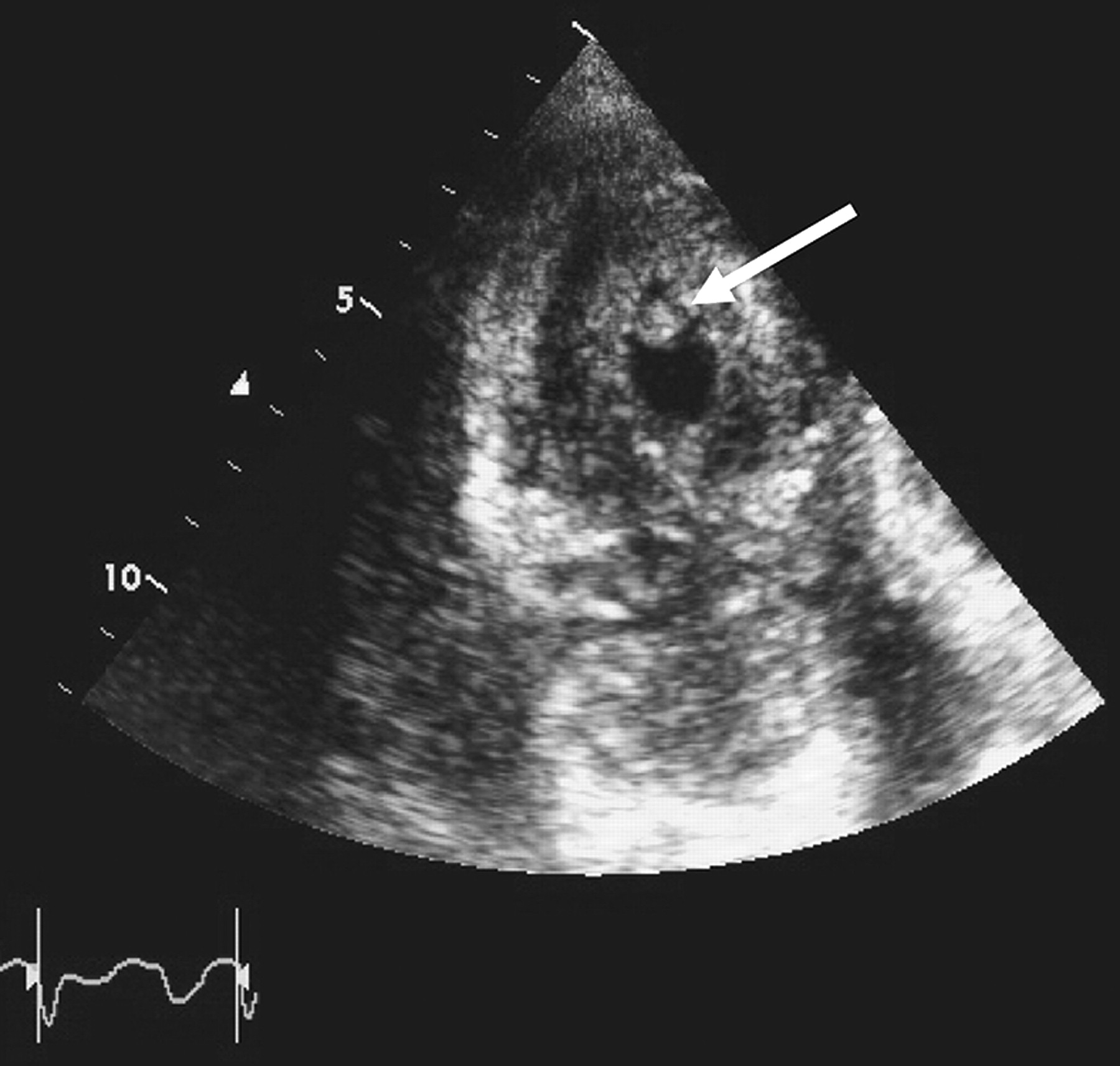
A 68-year-old woman presented with pneumonia and was found on chest radiographs to have bilateral lung nodules. She was very anxious because of the possibility of lung cancer. She underwent a CT-guided lung biopsy, which revealed squamous-cell carcinoma of the lung. On the same day, inferolateral ST elevation was noted on electrocardiogram. The patient denied any chest pain. Troponin T was elevated. Cardiac angiogram showed no coronary artery disease. Transthoracic echocardiogram revealed akinetic apex with preserved basal wall motion (figure 1, movie 1), mobile left-ventricle apical thrombus (figure 2, movie 2) and pericardial effusion. These findings were consistent with Takotsubo cardiomyopathy (TC). Anticoagulation was not administered owing to a high risk of bleeding. A subsequent thorax computed tomogram revealed extensive metastatic diseases, and the patient received palliative care. She died 3 days later.
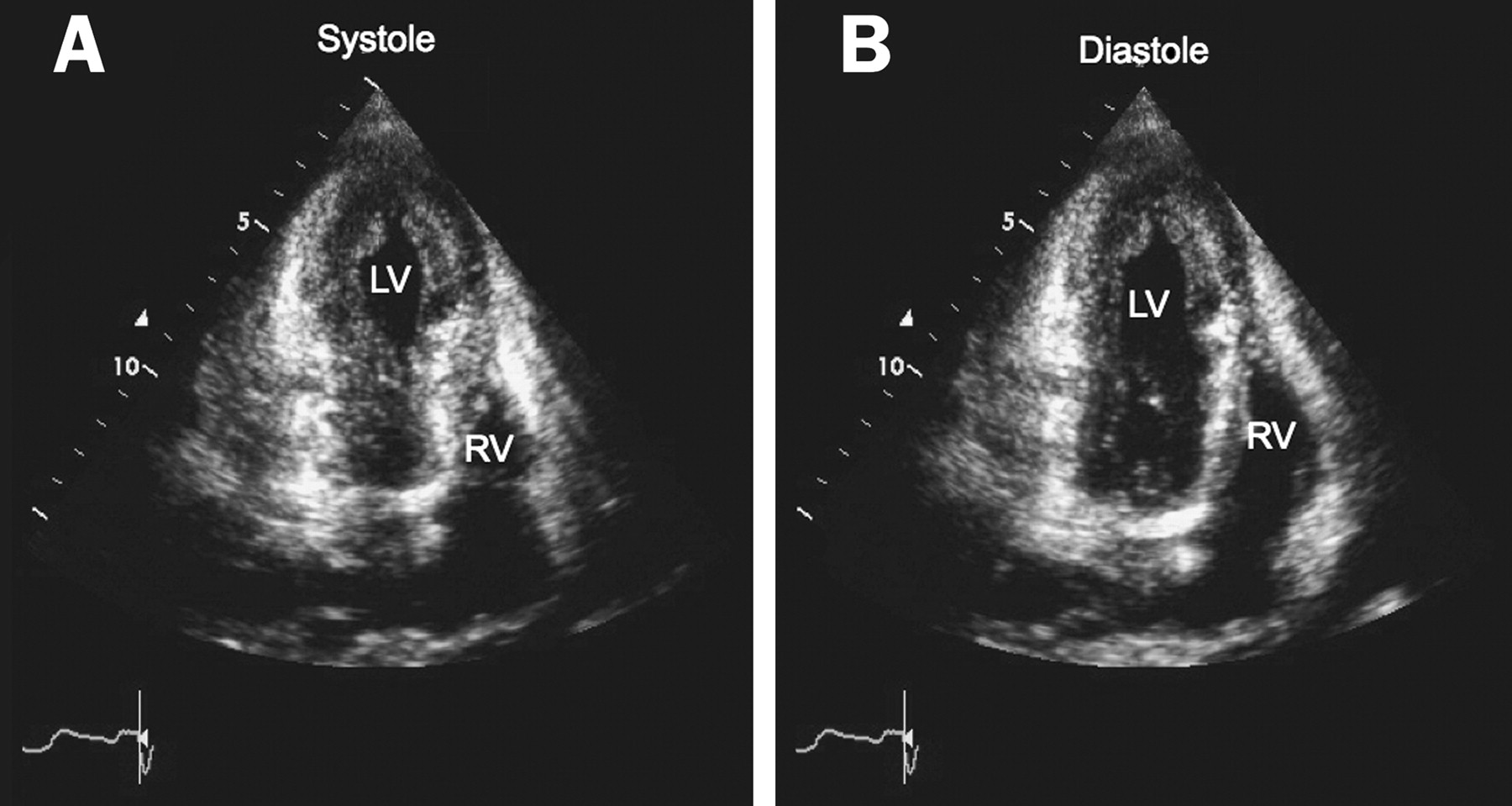
Apical four-chamber view of the left ventricle on a transthoracic echocardiogram in (A) systole and (B) diastole. Note the absence of left-ventricular apical contraction during systole; apical ballooning of the left ventricle can also be seen. LV, left ventricle; RV, right ventricle.
{kind=link}
{kind=link}
Modified apical long-axis view on a transthoracic echocardiogram of the left ventricle showing a large thrombus (arrow).
TC is a rare disease entity that occurs in 0.7–2.2% of patients with acute coronary syndrome, and it is often triggered by physical or emotional stress.1 Diagnostic criteria centre on acute and reversible left-ventricular apical ballooning of unknown cause.2 Most patients present with acute coronary syndrome-type symptoms, but without concomitant obstructive coronary artery disease.
Only a few case reports have suggested an association of TC with cancer. In our patient, apical thrombus could have occurred as a result of malignancy-associated hypercoagulability or akinetic apex, increasing the likelihood of thromboembolic events. Although apical thrombus is infrequent in TC, one needs to be aware of this possibility, evaluate the apical segments carefully and use contrast, if necessary, to exclude apical thrombus in patients with TC.
Footnotes
Competing interests None.
Patient consent Our patient is deceased, and we were unable to reach the patient's family for consent.
Provenance and peer review Not commissioned; not externally peer reviewed.