Article Text

Abstract
Objective Aldosterone is associated with increased mortality in chronic heart failure patients and correlates with adverse outcomes after an acute myocardial infarction (AMI) in smaller cohorts. We evaluated the prognostic significance of plasma aldosterone in a large cohort of post-AMI patients in relation to major adverse cardiovascular events (MACE).
Design A prospective cohort study.
Setting University Hospitals of Leicester, UK.
Patients Consecutive 955 patients admitted with AMI. Plasma aldosterone levels were measured in these patients.
Main outcome measures During the 2 years follow-up, MACE which was a composite of all-cause mortality, myocardial reinfarction, and hospitalisation for heart failure as well as secondary endpoints (all-cause mortality and a combination of all-cause mortality and hospitalisation for heart failure), were ascertained.
Results MACE occured in N=261, 27.3%, all-cause mortality (N=114, 11.9%) and a combination of all-cause mortality and hospitalisation for heart failure (N=176, 18.4%). Patients with MACE had significantly higher median levels of aldosterone than those without (1150.1 vs 950.4 pmol/l, p=0.0118). The multivariate adjusted HR (95% CI) for log aldosterone on MACE was 1.26 (1.01 to 1.56), p=0.041; all-cause mortality 1.60 (1.13 to 2.27), p=0.008; and combination of all-cause mortality and heart failure 1.50 (1.14 to 1.97), p=0.003.
Conclusions The prognostic significance of aldosterone for a variety of endpoints in this large cohort of post-AMI patients is not new and adds to the findings by others. The magnitude of the increase in aldosterone secretion post infarction is higher than previously believed.
- Heart Failure
- Myocardial Ischaemia And Infarction (IHD)
Statistics from Altmetric.com
Introduction
Mortality from coronary artery disease (CAD) has declined over the past decades in developed countries. This is largely due to a decrease in incidence accounted for by primary prevention and a decrease in case-fatality rate accounted for by high-impact interventional, surgical and pharmacological therapies, other secondary prevention measures and improved coronary care facilities.1 ,2 Nevertheless the burden of disease remains high and CAD is still the leading cause of death in developed countries accounting for about 15–20% of all deaths, and its incidence is rising in developing countries.1–3
Risk stratification post acute myocardial infarction (AMI) with multiple risk predictors including biomarkers with pathophysiologically distinct pathways appear to be the way forward. Hormones acting on the mineralocorticoid receptor are associated with adverse cardiovascular disease (CVD) outcomes.4–7 Much evidence has accrued in the past two decades to support the deleterious effects of aldosterone and cortisol activation of this receptor, and the role of prereceptor enzymes which determine the relative concentrations of these two hormones available at different tissues for mineralocortocid receptor binding has emerged.4–12
Aldosterone is associated with hypertension,13 endothelial dysfunction,14 atherosclerosis,4 ,5 poor systemic vascular compliance, increased vascular tone and decreased baroreceptor sensitivity, and promotion of myocardial necrosis and increase in infarct size.5 ,15 Aldosterone is also associated with increased risk of death and acute ischaemic events in CAD patients with a preserved left ventricular function and no AMI,16 increased mortality post myocardial infarction.10–12 increased cardiac remodelling post myocardial necrosis17 ,18 and increased mortality in chronic heart failure patients.8 ,9 Plasma aldosterone/renin concentration ratio is strongly associated with blood pressure values in patients undergoing coronary angiography.19 Trials have shown that mineralocorticoid blockade in chronic heart failure (RALES),20 and post AMI with ventricular dysfunction (EPHESUS) reduced mortality and hospitalisation for heart failure.21
Recent studies have demonstrated that aldosterone correlates with poor outcomes in patients undergoing scheduled coronary angiography,22 and in post-AMI patients.10–12 Whether aldosterone is predictive of major adverse cardiovascular events (MACE) in a larger cohort of post-AMI patients remains to be clearly shown. Therefore our aim was to prospectively evaluate the prognostic significance of plasma aldosterone in a large cohort of post-AMI patients in relation to MACE. We also assessed whether it correlated with secondary endpoints which were all-cause mortality, and combination all-cause mortality and hospitalisation for heart failure.
Materials and methods
Study design and study population
In this prospective cohort study, 955 consecutive patients with AMI admitted to the University Hospitals of Leicester NHS Trust between 2003 and 2008 were recruited. Written informed consent was obtained from patients, and the study complied with the Declaration of Helsinki and was approved by the local ethics committee. AMI was diagnosed if a patient had a plasma cardiac troponin I level >0.1 ng/ml with at least one of the following: chest pain lasting >20 min or diagnostic serial ECG changes consisting of new pathological Q waves or ST segment and T wave changes. Exclusion criteria included malignancy or surgery in the previous month. Data on demographics, clinical treatment, laboratory and echocardiography were obtained. All patients received standard secondary prevention therapy for ischaemic heart disease, and revascularization was at the discretion of the attending physician.
Blood sampling
Blood samples were drawn at 3–5 days after admission with AMI. 10 ml of venous blood was taken from the antecubital vein into tubes containing EDTA (1 ml/10 ml blood) and aprotinin (500 international units/ml blood). The blood samples were centrifuged at 3000 rpm 4°C for 15 min. The plasma was aspirated and stored at −80°C until assayed.
Steroid extraction
Plasma samples were defrosted at room temperature. 100 µl of patients’ plasma was mixed with 1 ml dichloromethane. The mixture was left on a shaker for 2 h and then spun down using a centrifuge at 2000 rpm. Then 0.7 ml of the dichloromethane layer was aspirated, and dried down in vacuum centrifuge to leave the aldosterone extract.
Aldosterone immunoassay
Aldosterone was measured using a competitive immunoluminometric assay. Each well of the microlite-two plate was coated with 100 µl (10 ng per well) of sheep antibody (Abcam) and left overnight at room temperature. Then 50 µl of polyclonal aldosterone antibody (Abcam) was added into each well and the samples were left to incubate overnight at 4°C. Using the automatic washer, the plates were washed in wash buffer and 200 µl of bovine serum albumin (BSA) was pipetted into each well of the plate. The plates were left for 2 h in BSA at room temperature, and then washed in wash buffer to remove any unbound BSA. Following this, 100 µl of sample was pipetted accurately into the well, each sample done in duplicate format and 50 µl of aldosterone-biotin tracer was pipetted into each well. The plates were left for incubation overnight at 4°C and the plates were washed in wash buffer to remove any unbound tracer. Then 100 µl of MAE-streptavidin was pipetted into each well and the plates were left in the dark at room temperature to incubate for 90 min. The plates were washed in wash buffer to remove unbound MAE-streptavidin. The plates were read using chemiluminescence in a DYNEX MLX luminometer (Dynex Technologies, Worthing, West Sussex, UK) and plate readings were given in relative light units (RLU). A standard curve was constructed using Rodbard's quadratic equation regression analysis (Biosoft, Great Shelford, Cambridge, UK). The luminometer readings were plotted on the y-axis (RLU) against aldosterone concentration (pmol/l) on the x-axis. The patient's plasma aldosterone concentration was calculated by interpolation of the standard curve. The RLU values for the samples were plotted on the standard curve and the corresponding concentration in pmol/l was efficiently calculated. The reproducibility of the assay was assessed by calculating the coefficient of variation which was 4.1%.
NT-proBNP assay
Plasma NT-proBNP assay was measured using a non-competitive immunoluminometric assay as previously published.23 The lower limit of detection was 0.3 pmol/l.
Endpoints
Patients were reviewed 24 months after their initial admission with AMI, giving a censoring time of 730 days. The primary endpoint was MACE, which was a composite of all-cause mortality, myocardial reinfarction, and hospitalisation for heart failure. There were two secondary endpoints: all-cause mortality and a combination of all-cause mortality and hospitalisation for heart failure. Deaths were validated by reviewing the hospital record management systems and the Office of National Statistics Registry. Hospitalisation for heart failure was defined as a hospital admission for which heart failure was the primary reason, requiring treatment with high-dose diuretics, inotropes or intravenous nitrate with echocardiographic evidence of heart failure. New myocardial infarction was defined as a plasma cardiac troponin I level >0.1 ng/ml with at least one of the following: chest pain lasting >20 min or diagnostic serial ECG changes consisting of new pathological Q waves or ST segment and T wave changes. New myocardial infarction and heart failure endpoints were ascertained using computerised hospital patients records for University Hospitals of Leicester and validated by contacting each patient.
Statistical anlyses
Statistical analyses were done using STATA V.11. The two-sample t test was used to test for any statistically signifcant difference between the means of normally distributed continuous variables across the binary outcomes (presence or absence of MACE, all-cause mortality, and combination of all-cause mortality and heart failure). The median and IQR were used for serum aldosterone because its distribution was positively skewed and for other skewed variables. The two-sample Wilcoxon rank-sum test was used to test for any significant difference in the medians of continuous variables which were not normally distributed across the binary outcomes. The Pearson χ2 test was use to compare categorical variables. The χ2 test for trend was used to test the trend of event rate across ordered quartiles of serum aldosterone. Curves of Kaplan-Meier survival estimates were obtained and the Logrank test was used to compare survival rates between patients whose aldosterone levels were above the median value and those below the median. Univariate and multivariate HRs for the predictive impact of baseline serum aldoesterone on endpoints were estimated by the Cox proportional hazard model. Because aldosterone distribution was skewed to the right, its levels were log-transformed to base 10 before the Cox regression analyses were carried out. The Likelihood ratio χ2 test was used to test for statistical significance of each variable in the Cox regression model.
Results
Baseline characteristics
Table 1 shows baseline characteristics of the study participants in the total study population and stratified by MACE outcomes. Post-AMI patients who developed MACE were significantly older, and had significantly greater median levels of baseline serum aldosterone. Similar baseline distributions were seen when the baseline characteristics were stratified by presence or absence of secondary outcomes which which were all-cause mortality or combination of all-cause mortality and heart failure binary outcomes.
Baseline characteristics of the entire study population and according to the presence or absence of MACE, which was the composite endpoint
Major cardiovascular events rate
The mean outcome was MACE which was a composite of myocardial infarction, death and hospitalisation for heart failure. During the 2 years of follow-up of the 955 post-AMI patients, MACE were n=261, 27.3%. The secondary outcomes included all-cause mortality (n=114, 11.9%) and a combination of all-cause mortality and hospitalisation for heart failure (n=176, 18.4%).
Aldosterone and MACE
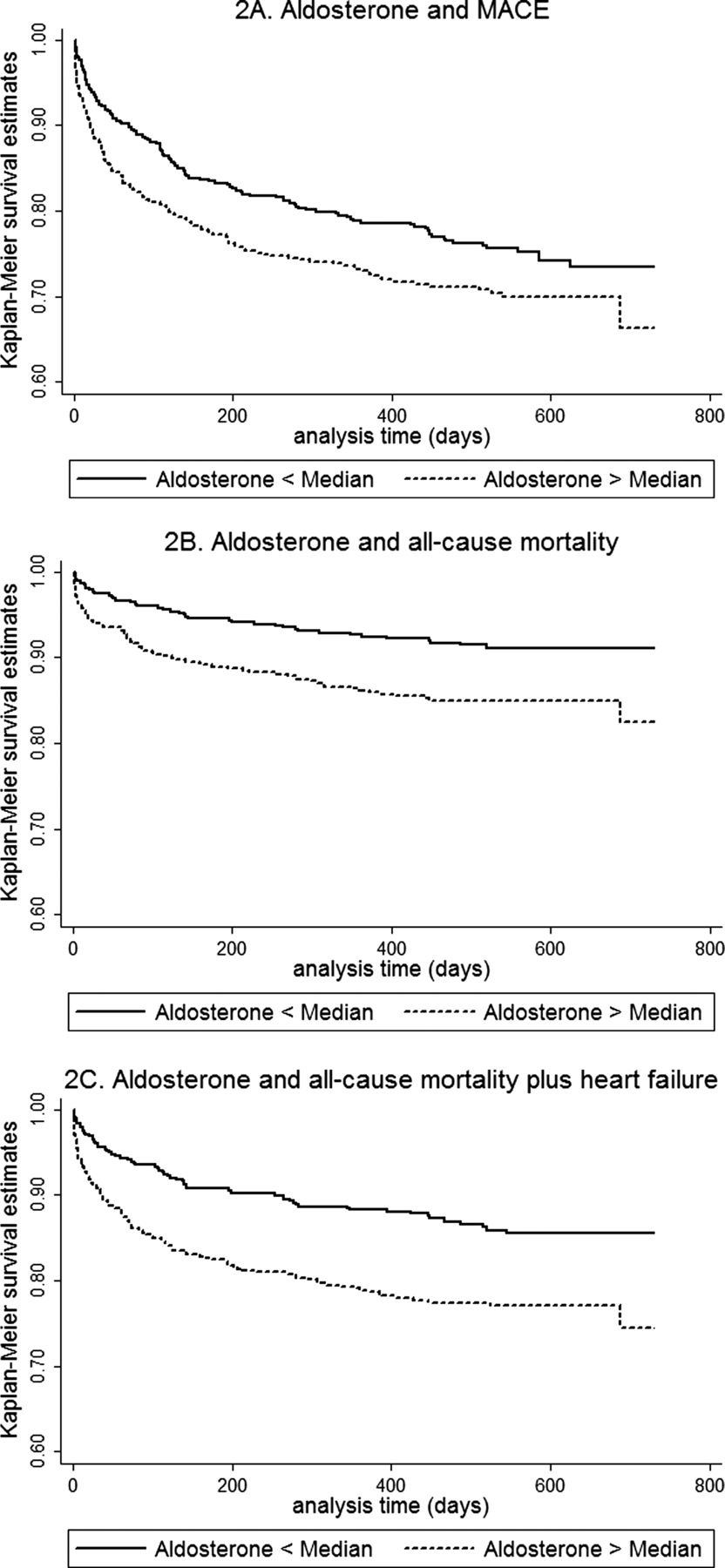
Patients with MACE had significantly higher median levels of aldosterone than those without (1150.1 vs 950.4 pmol/l, p=0.0118). As shown in table 2, log10-transformed aldosterone levels were independently predictive of future MACE after adjusting for covariates listed below the table. As shown in figure 1A, the MACE rate increased across ordered quartiles of baseline aldosterone (χ2 test for trend of survivor functions across aldosterone quartiles=9.17, p=0.0025). Patients in the highest quartile of aldosterone had signficantly more risk of MACE compared to those in the lowest quartile with a HR (95% CI) of 1.46 (1.01 to 2.12), p value 0.043 (table 2). Figure 2A shows statistically significant lower Kaplan-Meier survival estimates for MACE in patients with serum aldosterone above the median value compared to those below the median (Logrank test χ2 for adjusted survival=4.60, p=0.0320).
HRs (95% CI) from Cox regression for MACE, death, and death and heart failure, associated with Log aldosterone and upper quartiles compared to the lowest quartile of these variables, in post-acute myocardial infarction patients (N=955)
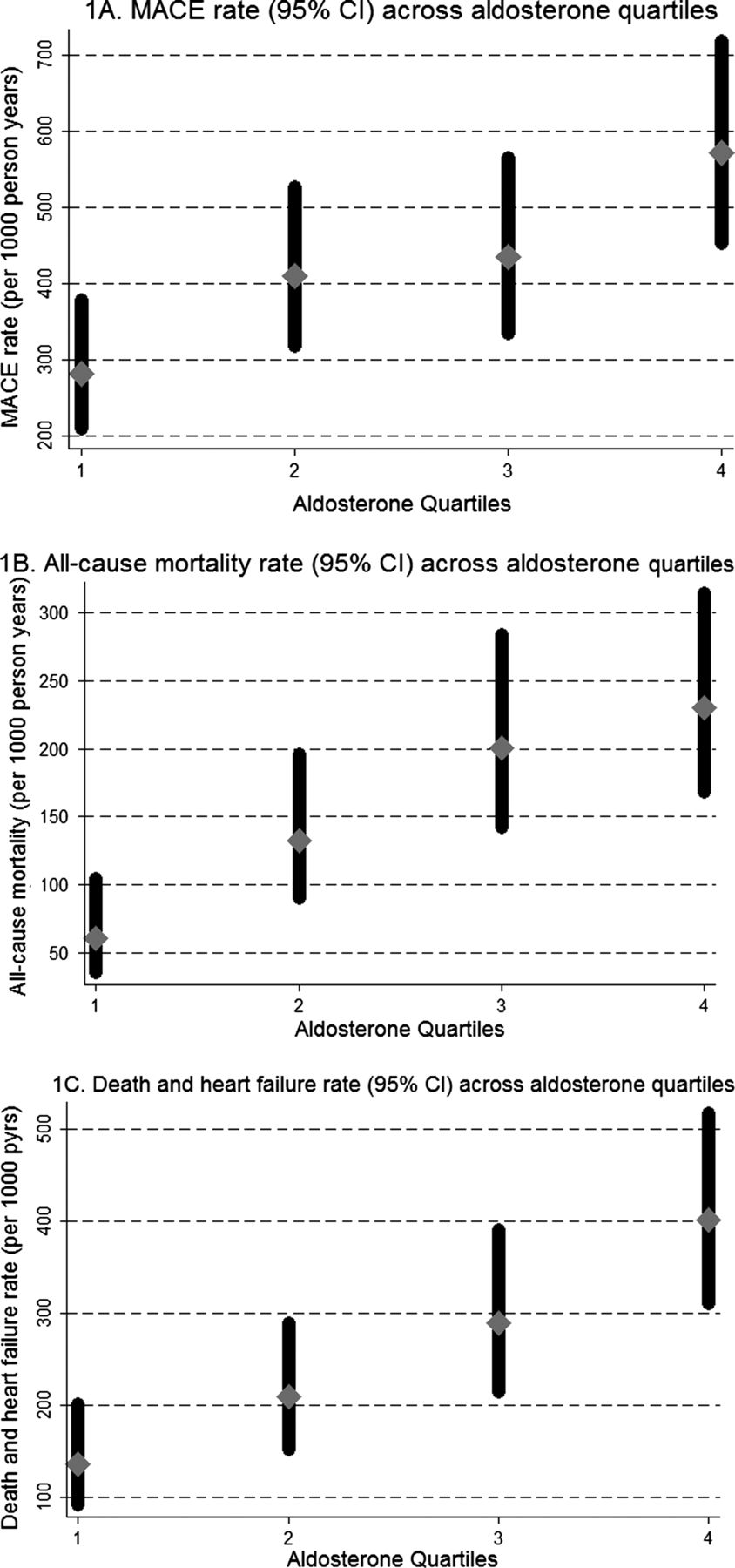
Outcomes across quartiles of plasma aldosterone major adverse cardiovascular events rate per 1000 person-years (A), all-cause mortality (B), and combination of all-cause mortality and hospitalisation for heart failure (C), across quartiles of aldosterone in post-acute myocardial infarction patients (N=955). χ2 test for trend of survivor functions across aldosterone quartiles for these three outcomes are respectively 9.17 (p=0.0025), 14.04 (p=0.0002), and 19.56(p<0.001).

{kind=link}
{kind=link}
Plasma aldosterone and Kaplan-Meier survival curves for major adverse cardiovascular events (MACE) (A), all-cause mortality (B), and combination of all-cause mortality and hospitalisation for heart failure (C) by ordered categories (below and above the median) of baseline plasma aldosterone in post-acute myocardial infarction patients (N=955). Logrank test χ2=4.60, p=0.0320 (MACE); 10.93, p=0.0009 (all-cause mortality); 14.98, p=0.0001 (combination of death and hospitalisation for heart failure).
Aldosterone and all-cause mortality
All-cause mortality was experienced at a higher rate (n=73, 15.3%) in patients with aldosterone levels above the median, compared to patients with aldosterone levels below the median (n=41, 8.6%), p=0.001. Looking at this from a different angle, patients who died had signficantly higher median levels (IQR) of serum aldosterone of 1298.1 pmol/l (722.8 to 2338.8), compared to those who survived 959.7 pmol/l (481.7 to 1706.9), p=0.0005. Figure 1B shows death rates across quartiles of aldosterone. Table 2 depicts that log10-transformed aldosterone levels were independently predictive of death in a multivariate Cox model, alongside age, N-terminal pro-B type natriuretic peptide, ACE inhibitors or angiotensin receptor blockers, β blockers, and statins, in the 955 patients with AMI. Compared with the lowest quartile of aldosterone, patients in the highest quartile were at a significant risk of mortality with a HR (95% CI) of 2.21 (1.21 to 4.03), p=0.010 (table 2). Kaplan-Meier survival estimates above and below median values of aldosterone are shown in figure 2B.
Aldosterone and combination of death and hospitalisation for heart failure
Median levels (IQR) of serum aldosterone were significantly higher in patients who experienced this combination (table 1). Looking at this from a different perspective, a higher rate (n=110, 23.0%) of this combined outcome was experienced by patients with serum aldosterone levels above the median compared to those below the median (n=66, 13.8%), p<0.001. As shown in table 2, log10-transformed aldosterone levels were an independent predictor of the combination of death and heart failure. There was an increasing trend of events rates across ordered quartile of serum aldosterone with χ2 for trend of 19.56, p<0.0001. Compared to the lowest quartile, patients in the highest quartile had HRs (95% CI) of 2.06 (1.29 to 3.28), p=0.002, after controlling for confounding variables. Figures 1C and 2C depict mortality and Kaplan-Meier survival estimates respectively across quartiles of serum aldosterone.
Discussion
Our study demonstrated that plasma aldosterone measured 3–5 days after occurence of myocardial infarction (ST elevation myocardial infarction (STEMI) and non-ST elevation myocardial infarction (NSTEMI) is independently predictive of MACE defined as all-cause mortality, reinfarction and hospitalisation with heart failure as well as secondary outcomes which were all-cause mortality alone and combination of all-cause mortality and hospitalisation for heart failure. These findings are similar to those observed in three previous publications,10–12 albeit in a larger cohort of patients and with different combinations of outcomes. Palmer et al had previously observed that plasma aldosterone levels post-AMI were independent predictors of survival and hospitalisation for heart failure over a 5-year follow-up in their cohort of >500 patients. Beygui et al had earlier observed that in STEMI patients referred for primary percutaneous angioplasty, high aldosterone levels correlated with an increase in rates of inhospital all-cause death, cardiovascular death, heart failure, ventricular fibrillation, resuscitated cardiac arrest and increased mortality after 6 months of follow-up >300 patients.11 They went further to demonstrate in the OPERA study that high plasma levels of aldosterone were independently predictive of the composite outcome of death, resuscitated cardiac arrest, recurrent myocardial infarction, heart failure and stroke in >400 post-AMI patients during hospitalisation and after 1 year of follow-up.12 Recently, Ivanes et al observed a significantly increased risk of death and acute ischaemic events in CAD patients with a preserved left ventricular function and no AMI with high levels of baseline aldosterone.16 More recently Weir et al showed that in post-AMI patients, levels of cortisol and aldosterone were independently predictive of cardiac remodelling defined as change in left ventricle (LV) end-systolic volume index, measured using contrast-enhanced cardiac magnetic resonance at baseline and after 24 weeks of follow-up.17 In patients undergoing scheduled coronary angiography in the large Ludwigshafen risk and cardiovascular health (LURIC) Study, variation in levels of plasma aldosterone concentration within the normal range was associated with increased risk of all-cause and CVD mortality independent of major CVD risk factors, and this risk persisted in a subgroup of patients who had suffered an acute coronary syndrome.22 The importance of aldosterone in the mediation of adverse cardiovascular outcomes has been underlined by two landmark trials, randomised aldactone evaluation study (RALES) and eplerenone post -acute myocardial infarction heart failure efficacy and survival study (EPHESUS).20 ,21 In the RALES trial, mineralocorticoid receptor blockade with spironolactone in addition to standard therapy substantially reduced the risk of both death and hospitalisation among patients with severe heart failure.20 In the EPHESUS trial, eplerenone added to optimal medical therapy reduced morbidity and mortality among patients with AMI complicated by left ventricular dysfunction and heart failure,21 and an earlier initiation of eplerenone was associated with a greater reduction in adverse outcomes.24
In both the studies by Palmer et al and Beygui et al, the mean level of aldosterone was about 100–120 pmol/l (which are within the normal range), whereas in our study the levels of aldosterone measured 3–5 days post infarction were significantly much higher, around the 1000 pmol/l mark and higher than the quoted normal range of 100–450 pmol/l in recumbent resting adults. Our data suggests that activation of aldosterone secretion post infarction may be more marked than previously believed, and underscores the importance of effective mineralocorticoid blockade in these patients.
Aldosterone is normally produced in the adrenal zona glomerulosa via activation of the renin angiotensin aldosterone system (RAAS) pathway. However, extra-adrenal aldosterone expression has been observed in cardiomyocytes,5 ,25 brain5 ,26 and vascular smooth muscle.5 ,27 Aldosterone acts on mineralocorticoid receptors which are expressed both on sodium-transporting epithelia and vascular endothelium, and non-epithelial tissues such as brain,28 myocardium5 ,29 and vascular smooth muscle cells.5 ,30 It has been reported that plasma aldosterone is extracted through the heart in patients with chronic heart failure and in post-AMI patients and that the transcardiac gradient of plasma aldosterone correlates with LV end-diastolic volume index and plasma levels of procollagen type III aminoterminal peptide, a marker of myocardial fibrosis and that administration of mineralocorticoid receptor blockade prevents this remodelling.18 ,31 Other studies have shown that aldosterone is predictive of mortality in chronic heart failure patients, alongside other neuroendocrine markers.9 It is well established that in the Conn's or primary aldosteronism, hypertension is induced.13
The possible mechanisms through which aldosterone adversely affects the cardiovascular system are legion. These include increased sodium retention associated with consequential fluid overload, hypertension and potentially arrhythmogenic potassium and magnesium depletion,6 ,32 the inhibition of nitric oxide,33 oxidative stress,34 endothelial dysfunction14 and atherosclerosis. Aldosterone has also been associated with poor systemic vascular compliance, increased vascular tone and decreased baroreceptor sensitivity,35 promotion of myocardial necrosis and increase in infarct size,15 cardiac fibroblast activation and collagen deposition,36 cardiac myocyte hypertrophy, myocardial fibrosis and overall remodelling,6 ,18 and arrhythmias and sudden cardiac death.12 ,21 Plasma aldosterone/renin concentration ratios are strongly predictive of blood pressure values in patients undergoing coronary angiography.19
Limitations
Plasma concentrations of aldosterone before and during the ischaemic event were unknown. The plasma levels were measured 3–5 days after the index infarction and we were therefore unable to observe any differences in aldosterone levels over the course of the event. However our data was representative of the acute phase of AMI, where early interventional therapies based on severity of disease would be most appropriate. During follow-up, we did not ascertain the number of patients in this cohort who needed target vessel revascularisation as an endpoint, which could have increased the number of MACE.
Conclusion
Overall, aldosterone has been shown to be predictive of MACE. These results are not new but add to recent findings by others, albeit in a larger cohort of patients. Consideration of trials of early initiation of aldosterone blocking agents in patients who have suffered an AMI irrespective of whether they developed ventricular dysfunction is warranted.
Acknowledgments
We thank all the patients who participated in the study, and members of the Pharmacology and Therapeutics Group for their contribution in patient recruitment and assaying.
References
Footnotes
-
Contributors Each author contributed fully to the work.
-
Funding This study was supported by the Leicester NIHR Biomedical Research Unit in Cardiovascular Disease and by the Van Geest Foundation.
-
Competing interest None.
-
Patient consent Obtained.
-
Ethics approval Local Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.