Article Text

Abstract
Objective To study the relationship among brain natriuretic peptide (BNP), cholesterol and lipoprotein.
Design A retrospective, cross-sectional study.
Setting Tokushima University Hospital area.
Patients A retrospective study of 46 patients (nine inpatients and 37 outpatients) with angina pectoris or arrhythmias who were seen at Tokushima University Hospital Cardiovascular Division and had measurements of their BNP, fatty acid and lipid profile. The average age of patients was 57±17 years, and 39% were male subjects.
Main outcome measures BNP, dihomo-γ-linolenic acid, arachidonic acid, eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), apolipoproteinA1, apolipoprotein A2 (ApoA2), apolipoprotein B (ApoB), apolipoprotein C2, apolipoprotein C3, apolipoprotein E, total cholesterol (TC), triglyceride, high density lipoprotein cholesterol and low density lipoprotein cholesterol.
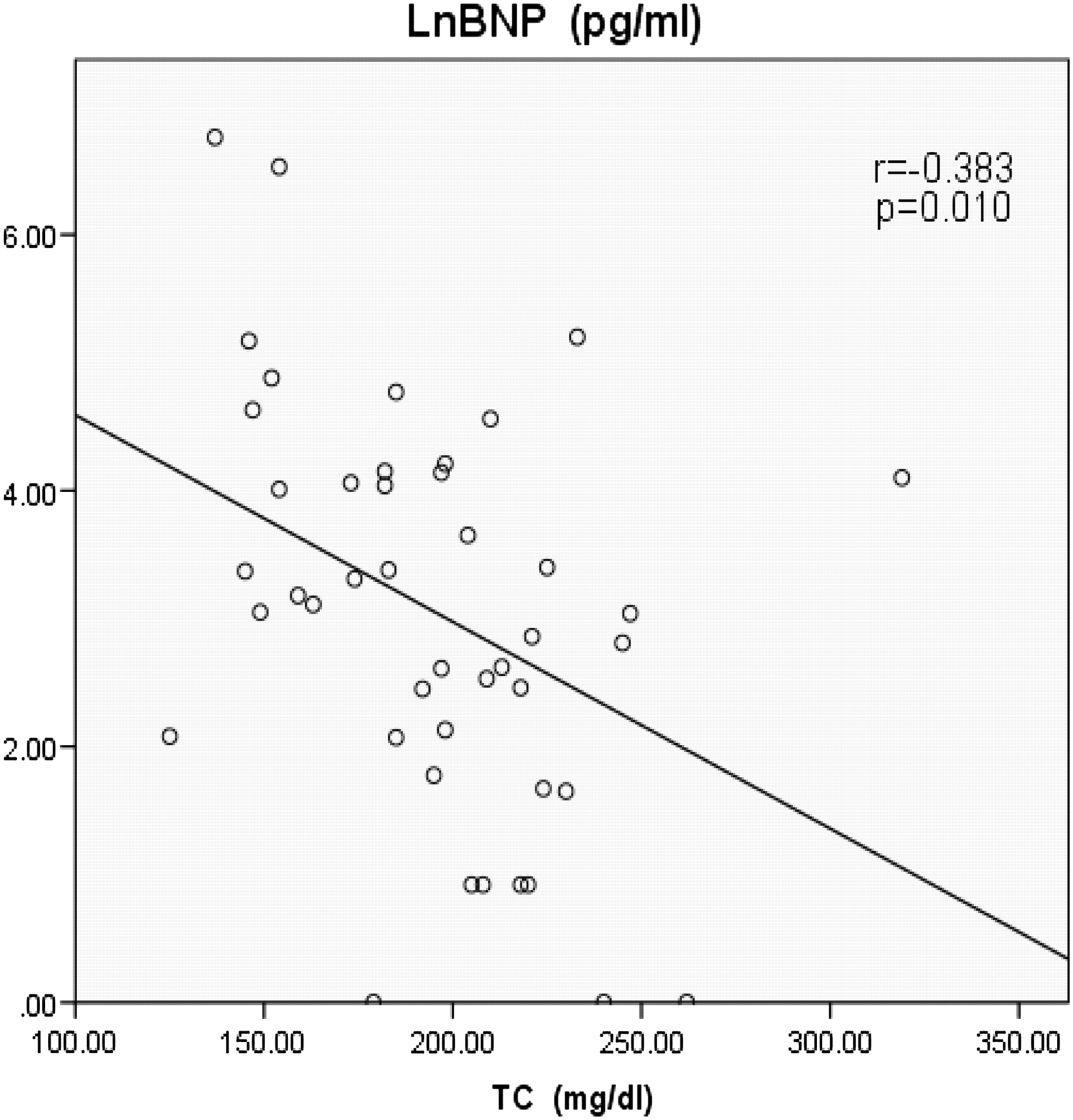
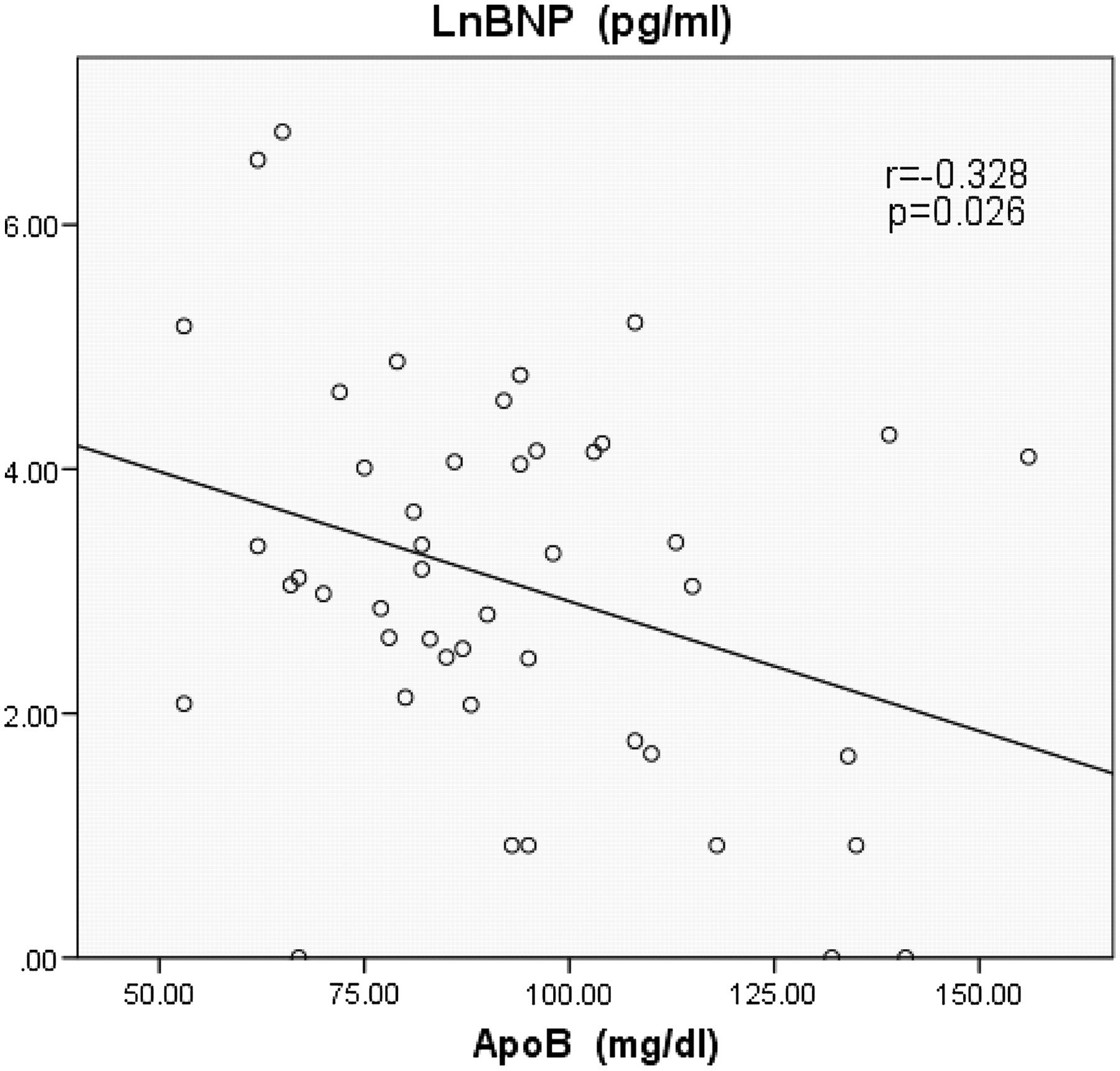
Results The baseline characteristics of the patients were shown in table 1 and the data of lipoprotein were shown in table 2. Table 3 shows the relationship among BNP, cholesterol and lipoprotein. The authors found significant negative correlation between serum levels of BNP and ApoA2 (figure 1; r=−0.458, p=0.001), serum levels of BNP and ApoB (figure 2; r=−0.328, p=0.026) and serum levels of BNP and TC (figure 3; r=-0.383, p=0.010). There is a possibility that dietary EPA and DHA may modulate cardiac mitochondrial and autonomic nervous system dysfunction via fatty-acids-PPARs-PTEN-PI3K/Akt-SREBPs system and affect serum BNP levels indirectly.
Conclusion BNP had significant negative correlation with ApoA2, ApoB and TC. The findings suggest that increasing serum levels of ApoA2, ApoB and TC may have an effect on improving heart function. But the mechanism is presently unclear.
- Heart failure treatment
- hypertension
- CT scanning
- gene expression
- coronary artery disease
Statistics from Altmetric.com
Background
Cholesterol and lipoprotein are important substances for body function and brain natriuretic peptide (BNP) is a marker of heart function. Increased serum BNP levels represent decreasing cardiac ventricular function.
BNP is produced mainly from the ventricle in response to volume expansion, pressure overload and elevated diastolic pressure,1 2 and modified by many factors including angiotensin 2, endothelin 1,3 neuron restrictive silencer element,4 hypoxia5 and cytokines.6 The serum level of BNP is correlated with the extent of ventricular dysfunction7–9 and coronary artery disease.10 11 And even in community-dwelling asymptomatic subjects, the serum level of BNP is correlated with a first cardiovascular event, heart failure and death.12
Cholesterol is an essential substance required for many functions, such as to maintain integrity of cell membranes, production of vitamin D on the surface of skin, and production of bile acid and steroidal hormones.13 14 While elevated plasma low density lipoprotein cholesterol (LDL-C) levels can result in plaque formation in the arterial wall, low plasma high density lipoprotein cholesterol (HDL-C) level is associated with progression of coronary atherosclerosis in the general population.15–19
Cholesterol is transported in the blood bound to apoproteins and phospholipids. Homeostasis of cholesterol is maintained by the metabolism of lipoproteins such as apoproteins and fatty acids, which mediate transport of the lipid to and from liver and tissues.
Fatty acids include n-6 polyunsaturated fatty acids such as arachidonic acid (AA) and dihomo-γ-linolenic acid (DGLA), and n-3 polyunsaturated fatty acids such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Although AA and EPA have the opposite effects, hepatic lipogenic gene expression is downregulated by both AA and EPA.20–22 The plasma DHA and EPA+DHA levels have been shown to correlate with the risk of coronary heart disease and fatal ischaemic heart disease.23–25 The Gruppo Italiano per lo Studio della Sopravvivenza nell'Insufficienza cardiaca (GISSI) heart failure study reported that when a low dose of EPA+DHA (0.85 g/day) was administered to heart failure patients for 3.9 years, mortality and hospitalisation were significantly decreased compared with placebo.26 The mechanisms by which EPA and DHA could prevent the development and progression of heart failure are unclear.
Apolipoproteins are the structural components of the lipoproteins. Most apolipoprotein A1 (ApoA1) are included in HDL and are produced within the small intestine and liver. ApoA1 controls activation of lecithin-cholesterol acyltransferase. Apolipoprotein A2 (ApoA2) is the second major protein component of HDL (25%), but its role in HDL metabolism is unclear.27 ApoA2 acts on lecithin-cholesterol acyltransferase and cholesteryl ester transfer protein.
Apolipoprotein B (ApoB) is the most abundant protein constituent of all lipoproteins except HDL. ApoB100 is produced in the liver and is the major component of the very low density lipoprotein (VLDL). ApoB48 is produced in the small intestine and is a major component of the chylomicron. HDL-C is composed of ApoA1, ApoA2, apolipoprotein E (ApoE) and cholesterol, and LDL-C is composed of ApoB100, triglyceride (TG) and cholesterol.
Apolipoprotein C2 (ApoC2) is a normal component of VLDL, where it plays an important physiological role as an activator of lipoprotein lipase, present in chylomicron and one of several members of the plasma apolipoprotein family that form amyloid fibrils. Apolipoprotein C3 (ApoC3) is present in HDL at the time of hunger and, with caloric intake, moves to chylomicron and VLDL. (ApoE) is present in HDL, chylomicron and VLDL mainly. ApoE participates in receptor-mediated uptake of these particles by liver.
There are few studies that have examined the direct relation among serum levels of BNP, cholesterol and lipoprotein in cardiovascular patients.
The aim of this study is to examine the relationship among serum levels of BNP and cholesterol and lipoprotein (apolipoprotein and phospholipid) in patients with cardiovascular disease.
Methods
We obtained blood samples from 46 consecutive patients (nine inpatients and 37 outpatients) with angina pectoris (AP), palpitation, arrhythmia such as atrial fibrillation and premature ventricular contraction of Tokushima University Hospital Cardiovascular Division between April 2010 and May 2011. The average age of patients was 57±17 years and 39% were male subjects. The mean value of BMI was 22.7±3.3 kg/m2 (range; 18.3∼32.9 kg/m2).
The diagnostic criteria for AP was >75% stenosis of at least one segment of a major coronary artery found on coronary angiography, which was performed because of clinical angina and exercise stress ECG changes with ST-segment elevation or depression of >0.5 mm or T-wave inversion in two or more leads accompanied by ischaemic chest discomfort.
Of the 46 patients, 25 patients had hypertension, 13 patients had AP, 24 patients had cardiac arrhythmias, two patients had hypertrophic cardiomyopathy and one patient had atrial septal defect. Although there were 19 hypertensive patients with a mix of AP or arrhythmias, there were no patients with a mix of AP and arrhythmias.
Patients who were included in the study had measurement of serum levels of BNP, DGLA, AA, EPA, DHA, ApoA1, ApoA2, ApoB, ApoC2, ApoC3, ApoE, TC, TG, HDL-C and LDL-C. Among 46 patients, nine (20%) were treated with statins. And among 46 patients, 14 (30%) were treated with EPA. Among those treated with EPA, two were treated with EPA (1800 mg), eight were treated with EPA (900 mg) and four were treated with EPA (640 mg)+DHA (432 mg). No patients were co-treated with statins and EPA.
Statistical analysis
Data were presented as means±SD. Correlation was analysed by Pearson's correlation coefficient. A probability value less than 0.05 was accepted as statistically significant. Statistical analyses were done with the statistical package for social sciences software (SPSS). We used the Japanese version of SPSS V.19.0 (SPSS Tokyo, Japan).
Results
The baseline characteristics of the patients were shown in table 1 and the data of lipoproteins were shown in table 2. Table 3 showed the relationship among BNP, cholesterols and lipoproteins.
Clinical characteristics of the patients
The data of lipoproteins
The relations among brain natriuretic peptide (BNP), cholesterols and lipoproteins (n=46)
We found significant negative correlation between serum levels of BNP and ApoA2 (figure 1; r=−0.458, p=0.001), serum levels of BNP and ApoB (figure 2; r=−0.328, p=0.026) and serum levels of BNP and total cholesterol (TC) (figure 3; r=−0.383, p=0.010). No significant correlation was found between serum levels of BNP and EPA (table 3; r=−0.241, p=0.107), serum levels of BNP and DHA (table 3; r=−0.280, p=0.060), serum levels of BNP and HDL-C (table 3; r=−0.218, p=0.155) and serum levels of BNP and LDL-C (table 3; r=−0.235, p=0.125).

Significant negative correlation between serum levels of brain natriuretic peptide (BNP) and apolipoprotein A2 (ApoA2) (r=−0.458, p=0.001). LnBNP, common logarithmic transformed serum levels of BNP.
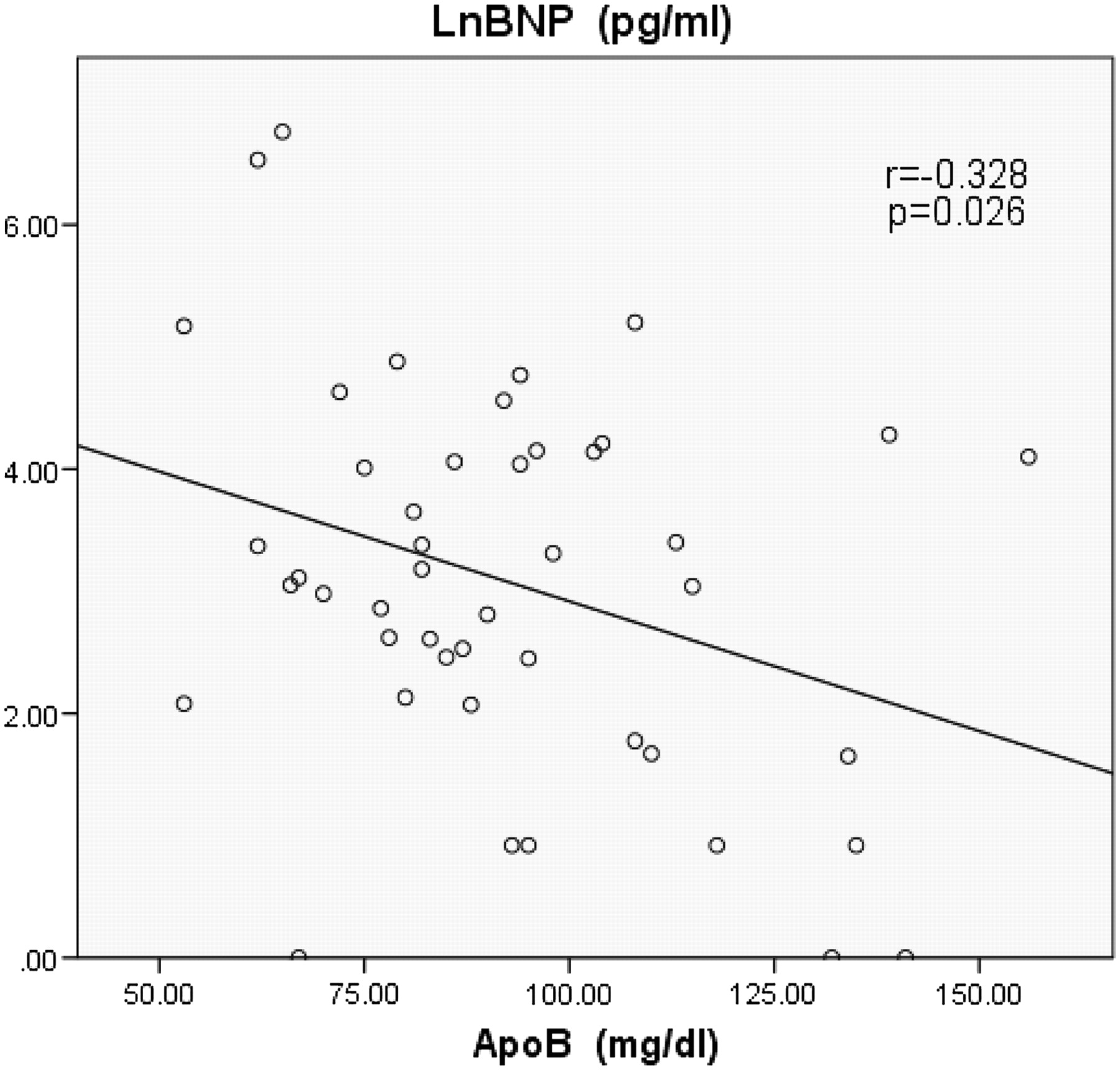
Significant negative correlation between serum levels of brain natriuretic peptide (BNP) and apolipoprotein B (ApoB) (r=−0.328, p=0.026). LnBNP, common logarithmic transformed serum levels of BNP.
{kind=link}
{kind=link}
{kind=link}
Significant negative correlation between serum levels of brain natriuretic peptide (BNP) and total cholesterol (TC) (r=−0.383, p=0.010). LnBNP, common logarithmic transformed serum levels of BNP.
Discussion
As far as we know, this is the first study to show that heart function, as represented by the biomarker BNP, was associated with plasma levels of cholesterol and apolipoprotein. The results of this study showed serum ApoA2 levels had the strongest negative relation to serum BNP levels. In addition, serum ApoB and TC levels had a significant negative relation to serum BNP levels.
There were a few papers that have reported a direct relationship between serum levels of BNP and HDL-C. Lupattelli et al28 reported that there was a ‘positive’ correlation between serum levels of BNP and HDL-C in the hyperlipidemic patients with serum BNP levels under 20 pg/ml (r=0.23, p=0.06).
But our results showed that there was no positive correlation but instead there was a trend towards a ‘negative’ correlation between serum levels of BNP and HDL-C (r=−0.218, p=0.155) even though it was not statistically significant. Although the range of serum levels of BNP was quite different, it was interesting that the relationship showed a trend that was opposite to previous studies.
In the GISSI heart failure trial, a low dose of EPA+DHA (0.85 g/day) administered to heart failure patients was correlated with a significant decrease in mortality and hospitalisation.26 The mechanisms of these effects of EPA+DHA on the heart were unclear. According to our results of the negative relations between the serum level of BNP and the serum level of ApoA2, ApoB and TC, a possible mediator may be alteration in serum apolipoprotein composition and TC levels; however, the administration effects of EPA+DHA were reviewed to make no definitive effects on the serum level of ApoA2, ApoB and TC in another paper.29
Our results showed serum levels of EPA and DHA had no significant negative relation to serum BNP levels, which might mean the effect of serum EPA and DHA level was weaker than ApoA2, ApoB and TC directly. In the GISSI heart failure trial, there was a possibility that dietary EPA and DHA may have good effects on heart via affecting mitochondria and autonomic nervous system directly. In previous studies, McMillin et al30 demonstrated that dietary fish oil favourably affected mitochondrial function. Sjoberg et al31 showed that dietary DHA, dose dependently, improved heart rate variability. However, the signalling mechanism remains elusive.
We will demonstrate one possible explanation of the signalling mechanism. First, fatty acids such as EPA, DHA and AA were well known to be identified as ligands of peroxisome proliferator-activated receptors (PPARs) by many studies.32–37
Second, Patel et al38 demonstrated PPARγ played a role in regulating phosphatidylinositol 3′-kinase (PI3K) and Akt (protein kinase B), which were signalling kinases involved in cell survival and proliferation, by modulating the phosphatase and tensin homologue (PTEN) tumour suppressor gene expression in inflammatory and tumour-derived cells. Lee et al39 showed that the administration of PPARγ agonists increased PTEN expression, which was correlated with decreased PI3K activity. PI3K pathway is downstream target pathway of PTEN,40 which plays a critical role in transmitting signals from growth factors to cell death and cell cycle machineries.41
Third, Fleischmann and Iynedjian 42 demonstrated that an activation of Akt causes the sterol-regulatory element-binding protein 1 (SREBP-1), master transcriptional regulators of lipid metabolism and mRNA accumulation in primary hepatocytes. In addition, the relation between the PI3K/Akt pathway and the sterol-regulatory element-binding proteins (SREBPs) has been studied extensively in many researches,42–46 in which PI3K seemingly activates SREBP function. Krycer et al47 reviewed the role of PI3K/Akt on SREBPs. They reviewed that recent evidence suggested PI3K/Akt activated SREBPs, but the precise molecular mechanisms were controversial and differed between SREBP isoforms.
Finally, some groups reported that SREBPs were associated with the gene regulation of mitochondria.48–50 And the relation between SREBPs and autonomic nervous system was recently discovered. Park et al51 reported a novel relationship between SREBP-1 and regulation of the cardiac parasympathetic response, and in another paper, Park et al52 demonstrated that SREBP-1 modulated parasympathetic response in type 1 diabetic Akita mice.
Therefore, dietary EPA and DHA might favourably affect the heart by ameliorating mitochondria and autonomic nervous system dysfunction via PPARs-PTEN-PI3K/Akt-SREBPs system, and so they improved mortality and hospitalisation.
Increased ApoA2 is obviously desirable for the reduction of cardiovascular disease including heart failure. It is known that increased LDL-C is associated with deteriorating atherosclerosis; however, not increased LDL-C but increased ApoB, which is main protein component of LDL-C, is associated with improved heart function.
Although it is not difficult to increase serum levels of EPA and DHA by food, it is difficult to increase apolipoprotein such as ApoA2 and ApoB by food directly. By understanding the regulation of ApoA2 and ApoB gene expressions, methods to increase ApoA2 and ApoB can be better understood. These interactions are important to understand the relation between heart function and cholesterol and lipoprotein.
Study limitations
The present study had several potential limitations because of the retrospective study nature and the number of patients was small, and so that it might not be representative of all patients. And the present study was of local patients who lived around Tokushima University Hospital (most patients live in Tokushima Prefecture), so that it might not be representative of all the patients globally. The people living in Tokushima eat more fish than Westerners, which may affect the results. In the future, a worldwide study is desirable.
Conclusion
This is the first reported study to show a direct correlation between serum levels of BNP and ApoA2, ApoB and TC. The findings suggest that increasing serum levels of ApoA2, ApoB and TC may have an effect on improving heart function. But the mechanism is presently unclear. In addition, the serum levels of DGLA, AA, EPA, DHA, ApoA1, ApoC2, ApoC3, ApoE, TG, HDL-C and LDL-C showed a trend towards negative correlation with serum BNP levels.
References
Footnotes
Competing interests None.
Patient consent Consent was not obtained but the presented data are anonymised and risk of identification is low.
Provenance and peer review Not commissioned; externally peer reviewed.