Article Text

Abstract
Increasing myocardial contractility has long been considered a big help for patients with systolic heart failure, conferring an augmented haemodynamic profile in terms of higher cardiac output, lower cardiac filling pressure and better organ perfusion. Though concerns have been raised over the safety issues regarding the clinical trials of different inotropes in hearts with systolic dysfunction, they still stand as a main therapeutic strategy in many centres dealing with such patients. They must be used as short in duration, low in dose and stopped as early as possible. Evidence-based guidelines have provided clinicians with valuable data for better applying inotropes in heart failure patients. In this paper, the authors address clinical trials with different agents used for increasing cardiac contractility in heart failure patients. Furthermore, the authors focus on recent guidelines on making the most out of inotropes in heart failure patients.
- Inotropic agents
- heart failure
- phosphodiesterase inhibitors
- β agonists
- ventricular tachycardia
- congenital heart disease
- Fallot's tetralogy
- coronary artery disease
- risk stratification
- heart failure with normal ejection fraction
- artificial heart
- rejection
- transplantation
Statistics from Altmetric.com
- Inotropic agents
- heart failure
- phosphodiesterase inhibitors
- β agonists
- ventricular tachycardia
- congenital heart disease
- Fallot's tetralogy
- coronary artery disease
- risk stratification
- heart failure with normal ejection fraction
- artificial heart
- rejection
- transplantation
Increasing myocardial contractility has long been considered a big help for patients with systolic heart failure, conferring an augmented haemodynamic profile in terms of higher cardiac output, lower cardiac filling pressure and better organ perfusion. Though concerns have been raised over the safety issues regarding the clinical trials of different inotropes in hearts with systolic dysfunction, they still stand as a main therapeutic strategy in many centres dealing with such patients. What is understood from major clinical trials is that longer event-free survivals, fewer hospitalisations, milder symptoms and improved exertional capacity are apparently more common in patients receiving β blockers. The aim is basically to block sympathetic pathways by which inotropes perform their effects. It implies that there is no benefit in forcing an exhausted heart to pump more vigorously. Yet, inotropes are undoubtedly helpful in many clinical scenarios, and they should be targeted for correctly selected heart failure patients if certain issues are to be addressed.
Agents used for increasing cardiac contractility act in different ways. The following is a brief description of those agents employed frequently in heart failure.
Dobutamine, the most commonly used inotropic agent worldwide, is a non-selective β1- and β2-adrenergic receptor agonist with variable activities on the α1 receptor.1 Prevalent β1- and β2-adrenergic receptor activation results in reduced afterload and increased stroke volume, heart rate and cardiac output at low doses. An increasing dose will add arterial and venous constriction due to α1 adrenergic receptor activation. Generally, severe tachycardia hinders clinicians in further upescalating the dobutamine dose. Clinical trials have documented excess mortality in heart failure patients receiving intermittent or continuous dobutamine infusion in spite of its beneficial effects on increasing the cardiac output and decreasing the pulmonary capillary pressure.2–6 Most heart failure specialists now agree to use dobutamine in decompensated heart failure patients with pulmonary congestion and presence of low cardiac output (hypotension, disturbed mentation and cardiorenal syndrome) and make the duration and dosage as low as possible.1 2 Precautions should also be taken when it is utilised in the elderly as well as in the presence of significant left ventricular outflow obstruction (eg, aortic stenosis), atrial fibrillation, recent β blocker use which necessitates an increase in dose, concomitant MAO inhibitor use and state of hyperthyroidism.4–6 The 2008 European Society of Cardiology (ESC) guideline on heart failure management recommends that dobutamine be generally started at 2–3 μg per kilogramme per minute (mcg/kg/min) without a loading dose and increased by 2–3 mcg/kg/min not exceeding 15 mcg/kg/min.7
Dopamine is one example of different dose-dependent effects due to the activation of different types of receptors. Dopamine primarily binds to vascular D1 receptors in the coronary, renal and mesenteric beds at low doses (≤2 mcg/kg/min) and leads to vasodilatation and natriuresis.1 It has been shown that this dopaminergic dose range might vary individually. Investigators of dopamine in acute decompensated heart failure (DAD-HF) trial have shown that adding a low dose (5 mcg/kg/min for 8 h) dopamine to reduced dose diuretics might provide as much diuresis as full dose diuretics on their own in patients with acute heart failure, without the potentially kidney-damaging and the potassium-draining effects of loop diuretics.8 9 This effect appears to be due to the dilation of both large conductance and small resistance renal blood vessels.10 Dopamine may exert this effect without significantly improving creatinine clearance.11 This effect is not generally affected by chronic β blocker use, which is the case in most decompensated heart failure patients,12 but may be blunted by haloperidol and other butyrophenones.13 Ibopamine, a dopamine agonist that stimulates the dopaminergic-1 and dopaminergic-2 receptors resulting in peripheral and renal vasodilatation, improved heart failure symptoms during a short-term use,14 but was associated with increased mortality in the PRIME-II trial, which evaluated 1906 patients with severe (New York Heart Association (NYHA) class III and IV) heart failure who were already receiving maximal medical therapy (25% vs 20% for placebo at approximately 1 year).15 Intermediate doses result in the activation of myocardial β1 receptors, with positive inotropic effects.1 Dopamine usually increases the systolic blood pressure and heart rate, with no or minor changes in diastolic pressure and peripheral vascular resistance.1 At high doses (5–15 mcg/kg/min), dopamine also binds to α1 receptors and triggers vasoconstriction.1 The usual dose range for dopamine is 2–20 mcg/kg/min, although doses as high as 130 mcg/kg/min have been employed.16 Dopamine is most often used in hypotension due to sepsis or cardiac failure, where it should be started at 2 mcg/kg/min and then titrated to a desired physiologic effect rather than a predicted pharmacologic range. Such titration is necessary because a weight-based administration of dopamine can achieve quite different serum drug concentrations in different individuals.17
Epinephrine has potent β1 adrenergic receptor activity and moderate β2 and α1 adrenergic receptor effects. Clinically, low doses of epinephrine increase the cardiac output because of the β1 adrenergic receptor inotropic and chronotropic effects, while the α adrenergic receptor-induced vasoconstriction is prominent in higher doses,18 making epinephrine a titratable vasoactive agent to support hypotension due to low cardiac output or generalised vasodilatation, which occurs not infrequently after cardiopulmonary bypass pump. Clinical trials of safety and efficacy of epinephrine in heart failure patients are lacking.
Norepinephrine acts on both α1 and β1 adrenergic receptors, thus producing potent vasoconstriction as well as a less pronounced increase in cardiac output.19 A reflex bradycardia usually occurs in response to the increased MAP, such that the mild chronotropic effect is cancelled out and the heart rate remains unchanged or even decreases slightly. In a multi-central, randomised trial on patients with shock, 1679 patients were randomly assigned to receive dopamine or norepinephrine. A subgroup analysis showed that dopamine, as compared with norepinephrine, was associated with an increased rate of death at 28 days among the patients with cardiogenic shock but not among those with septic or hypovolemic shock. There were more arrhythmic events among the patients treated with dopamine.20 Norepinephrine should be administered only through a central venous line because extravasation may cause tissue necrosis.1
Milrinone, a phosphodiesterase 3 inhibitor, inhibits the breakdown of cyclic AMP in both cardiac and vascular smooth muscle cells and acts as a powerful inotrope and pulmonary vasodilator agent with little effect on systemic arterial blood pressure.21 Initial uncontrolled observations suggested that prolonged outpatient therapy with intravenous milrinone, either continuous or weekly, could improve functional status and reduce hospitalisation.22–24 However, this was not the case in the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-HF), a controlled trial in 949 patients admitted to the hospital with an acute exacerbation of chronic heart failure and a mean left ventricular ejection fraction of 23%; patients requiring inotropic support were excluded. Milrinone therapy was associated with significant increases in hypotension, requiring intervention and atrial arrhythmias, and with non-significant increases in mortality in hospital (3.8% vs 2.3%) and at 60 days (10.3% vs 8.9%) (figure 1). It is worthy of note that patients with ischaemic cardiomyopathy did significantly worse with milrinone in terms of the primary end point of days of hospitalisation and the combined end point of hospitalisation plus death25 26 (figure 2). The Acute Decompensated Heart Failure national registry, though putting sicker patients on milrinone and dobutamine, showed clear increased mortality with these agents compared with nitrate or nesiritide.27 Milrinone should be confined for those advanced heart failure patients with low cardiac output state and intolerable congestion. Pulmonary vasodilator effects give the opportunity of better tackling left-sided pulmonary hypertension. Acting distal to and independently of the β receptors might provide the chance of adding milrinone to chronic β blocker therapy. The possible long-term benefit of combined therapy was evaluated in a series of 30 patients with refractory NYHA class IV heart failure who were treated with a combination of enoximone and metoprolol: this regimen was well tolerated by 80% of patients. After a mean follow-up of 21 months, significant benefits included an increase in left ventricular ejection fraction (28% vs 18% before therapy) and improvement in NYHA class (2.8 vs 4). Approximately, half of the patients were able to discontinue enoximone. The estimated probability of survival at 1 year was 81%, a value higher than would have been expected from the results in large trials of similar patients.28 Although preliminary trials with oral milrinone, like other phosphodiesterase inhibitors, have been associated with increased mortality compared with placebo (which was best demonstrated in the PROMISE trial, in which patients with NYHA class III or IV heart failure who were randomly assigned to oral milrinone faced a significant 28% increase in all-cause mortality (30% vs 24% with placebo), 34% increase in cardiovascular mortality, a greater incidence of hospitalisations, more adverse cardiovascular side effects (syncope and hypotension) and higher drug discontinuation rate),29 30 investigations considering milrinone inhalation are grabbing attention as a useful non-invasive route of administration.31 32 Intravenous milrinone is generally prescribed at 0.375–0.75 mcg/kg/min without a loading dose, especially in those with baseline lower blood pressure.1
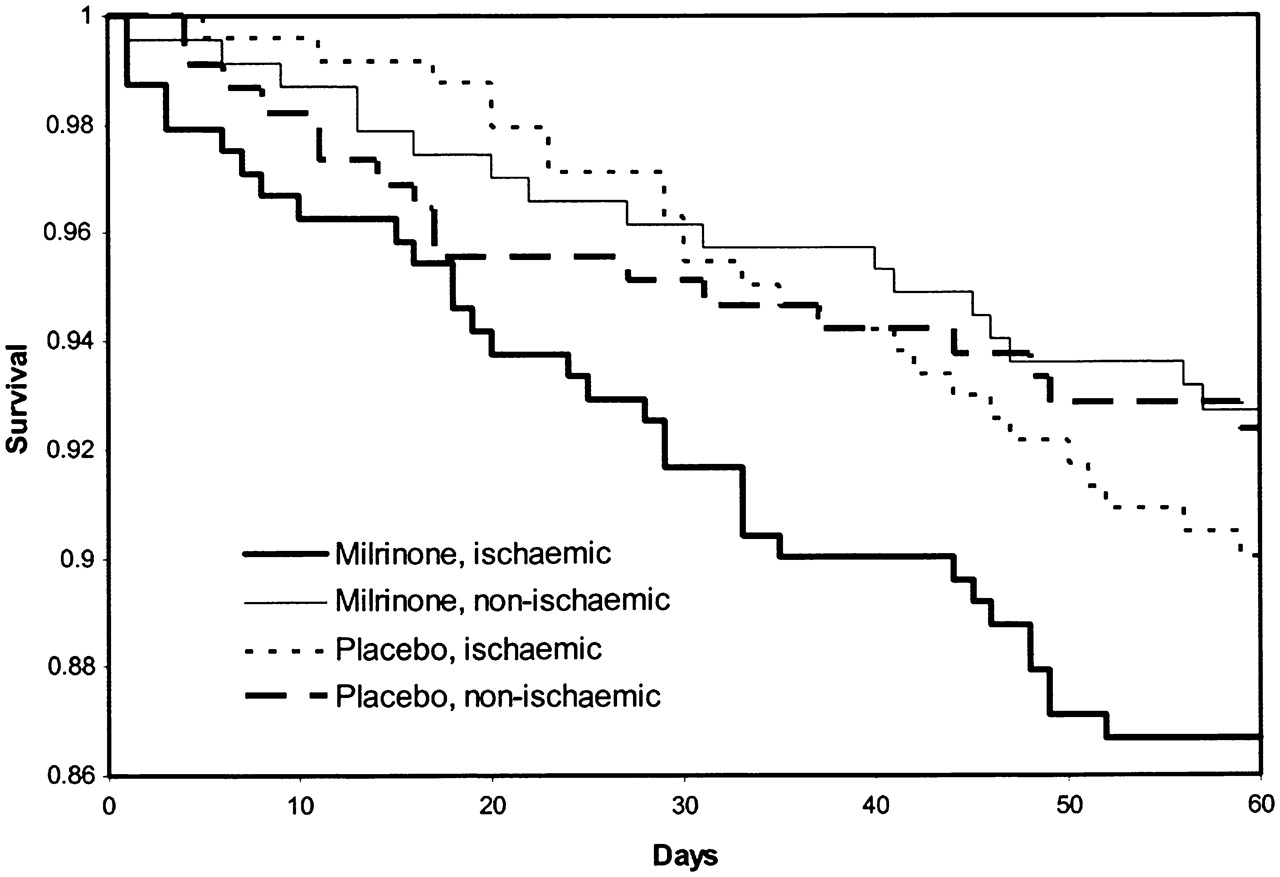
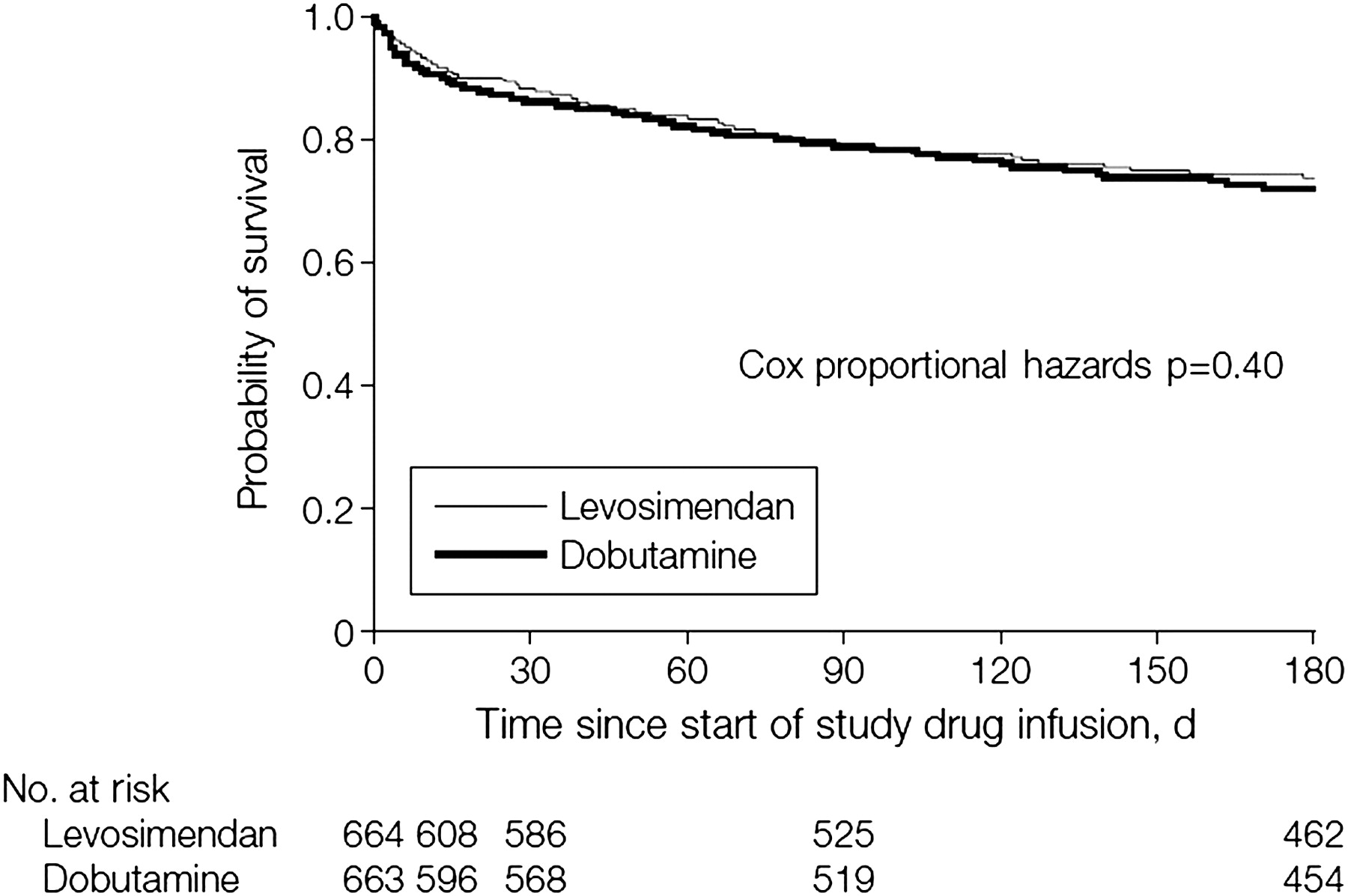
Levosimendan is a calcium sensitiser and ATP-dependent potassium channel opener with mild phosphodiesterase inhibitory action (ESC) that has positive inotropic and vasodilatory effect, resulting in a reduction in cardiac filling pressures and an increase in the cardiac index. In a report of 146 patients with severe heart failure, 6 h of intravenous levosimendan produced an increase in stroke volume and cardiac index of 28% and 39%, respectively, and a dose-dependent reduction in pulmonary capillary wedge pressure, right atrial and pulmonary artery pressures, and symptoms of dyspnoea and fatigue.33 The LIDO trial compared the short-term haemodynamic effects of a 24 h intravenous infusion of levosimendan with dobutamine in 203 patients with severe, deteriorating heart failure, acute heart failure or heart failure after coronary artery bypass grafting; patients with cardiogenic shock were excluded.2 The haemodynamic end point (35% increase in cardiac index and ≥25% reduction in pulmonary capillary wedge pressure at 24 h) was more frequently achieved with levosimendan than dobutamine (28% vs 15%) (figure 3). The effects of levosimendan were not attenuated by concurrent therapy with a β blocker in contrast to dobutamine.2 The SURVIVE trial randomly assigned 1327 patients with acute decompensated heart failure and a left ventricular ejection fraction of ≤30% to intravenous levosimendan or dobutamine. After 24 h of therapy, there was no difference between the groups assigned to levosimendan or dobutamine in the percentage of patients who reported more than a mild improvement in dyspnoea (82% vs 83%) or a global assessment (80% vs 81%). Patients assigned to levosimendan did have a significantly greater reduction in plasma BNP compared with patients assigned to dobutamine (631 vs 397 pg/ml). However, levosimendan use was associated with more atrial fibrillation and hypokalemia34 (figure 4). In the REVIVE II study, an improvement in patient self-assessment, a decrease in levels of BNP and a shorter hospital stay were noted in response to levosimendan when it was added to standard therapy in patients admitted with heart failure and reduced ejection fraction. Be that as it may, compared with placebo, levosimendan use was associated with more hypotension (50% vs 34%), ventricular tachycardia (25% vs 17%) and atrial fibrillation (9% vs 2%). A trend towards increase in early mortality was also observed in the levosimendan-treated patients.35 The ESC guidelines recommend levosimendan to be administered as a bolus dose (3–12 mcg/kg) during 10 min, followed by a continuous infusion (0.05–0.2 mcg/kg/min for 24 h). The infusion rate may be increased once stability is confirmed. In patients with a systolic blood pressure of <100 mm Hg, the infusion should be started without a bolus dose to avoid hypotension.7 A randomised clinical trial (the Pimobendan in Congestive Heart Failure (PICO) trial) employed pimobendan, another calcium sensitiser, added to conventional failure treatment in 317 patients with stable symptomatic heart failure improved exercise duration (bicycle ergometry) by 6% (p=0.03 and 0.05) after 24 weeks of treatment with no significant effects on oxygen consumption and on quality of life. Nonetheless, pimobendan use was associated with an increased hazard of death, 1.8 times higher than that in the placebo group.36
Vesnarinone is a mixed phosphodiesterase 3 inhibitor and ion-channel modifier that has modest, dose-dependent, positive inotropic activity, but minimal negative chronotropic activity. A beneficial effect on survival in severe heart failure was shown in a small placebo-controlled clinical trial at a dose of 60 mg daily associated with a trend towards an adverse effect on survival when the dose was 120 mg per day.37 Vesnarinone (30–60 mg daily) was compared with placebo in 3833 patients with NYHA class III and IV heart failure in the VEST trial. The trial was terminated prematurely due to a dose-dependent increase in mortality (12% and 23% in patients receiving 30 and 60 mg/day, respectively), primarily secondary to sudden cardiac death38 (figure 5).
Digoxin, the only safe and effective oral positive inotropic agent, acts by inhibiting the Na-K-ATPase pump, leading to a rise in the intracellular calcium concentration and also exerts an antiadrenergic action by inhibiting the sympathetic outflow and augmenting the parasympathetic tone.39 40 Digoxin withdrawal in chronic heart failure patients on digoxin and other antifailure therapies, as investigated in the PROVED and RADIANCE trials, resulted in clinical deterioration.41 42 Ever since, the DIG (Digoxin Investigators' Group) trial has been the largest survey addressing the effect of digoxin on heart failure survival.43 After 3 years, there was no difference in the overall mortality rate. Patients assigned to digoxin therapy had a non-significant reduction in mortality from worsening heart failure, counterbalanced by a significant increase in non-heart failure cardiac deaths, which included death from arrhythmia. Though modest, patients assigned to digoxin enjoyed a significant decrease in hospitalisation and a significant reduction in the combined end points of death from heart failure and hospitalisation. Post hoc analyses showed a correlation between the digoxin level and patient survival,44 45 such that death and hospitalisations were reduced in patients with a serum digoxin level between 0.5 and 0.9 ng/ml, regardless of the ejection fraction or gender. It is noteworthy that digoxin did worse in women in terms of all-cause mortality and heart failure mortality and hospitalisation than in men.46 Digoxin can be used orally or intravenously. The dose should be adjusted according to renal function and should result in a trough serum concentration of <1 ng/ml.1 In patients with a reduced ejection fraction who continue to have signs and symptoms of heart failure, digoxin therapy should be continued in addition to other therapies during hospitalisation and after discharge. Ischaemia, hypokalaemia and hypomagnesaemia may increase the likelihood for the development of digitalis intoxication, even at the therapeutic doses.1
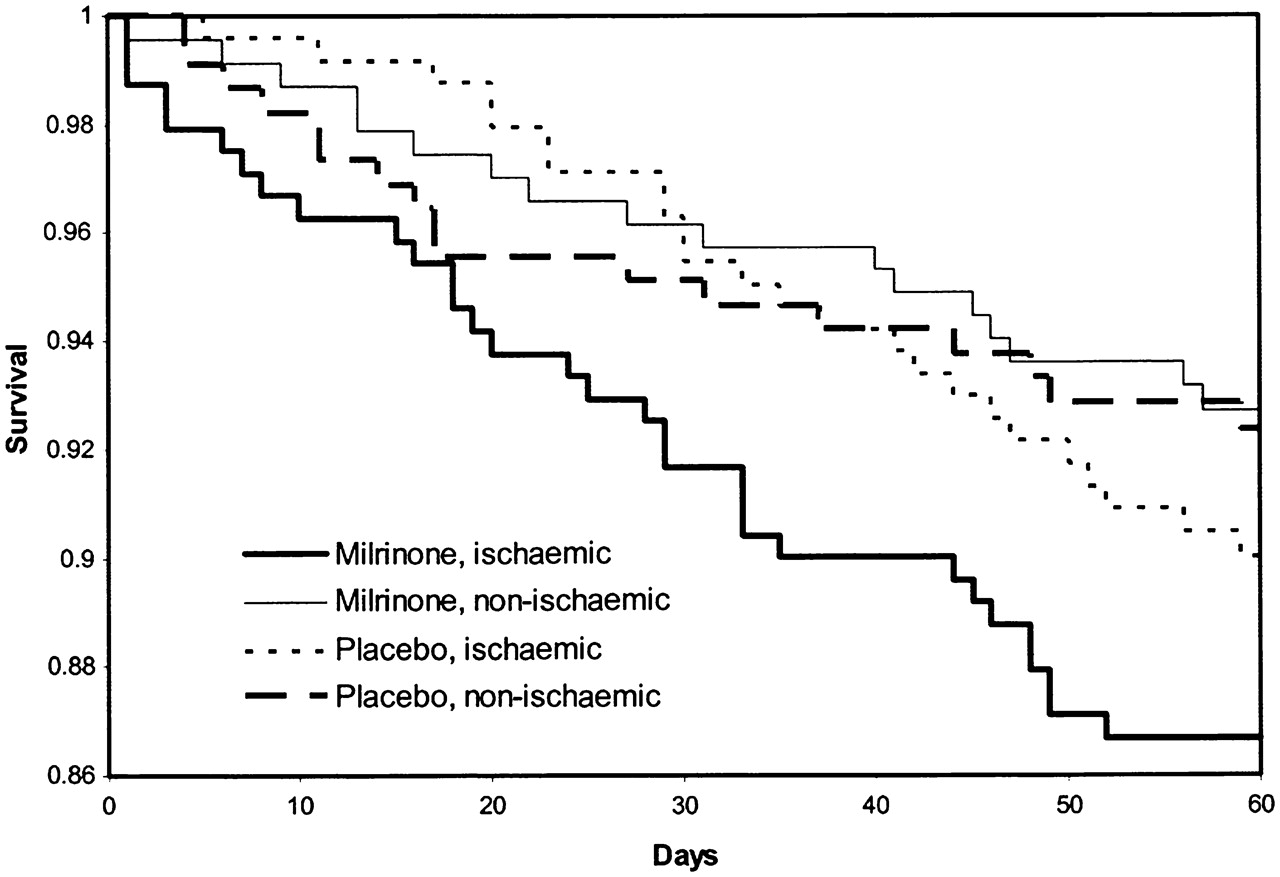
Kaplan–Meier survival curves to 60 days by heart failure aetiology and treatment assignment (outcomes of a prospective trial of intravenous milrinone for exacerbations of chronic heart failure (OPTIME-CHF) study).25
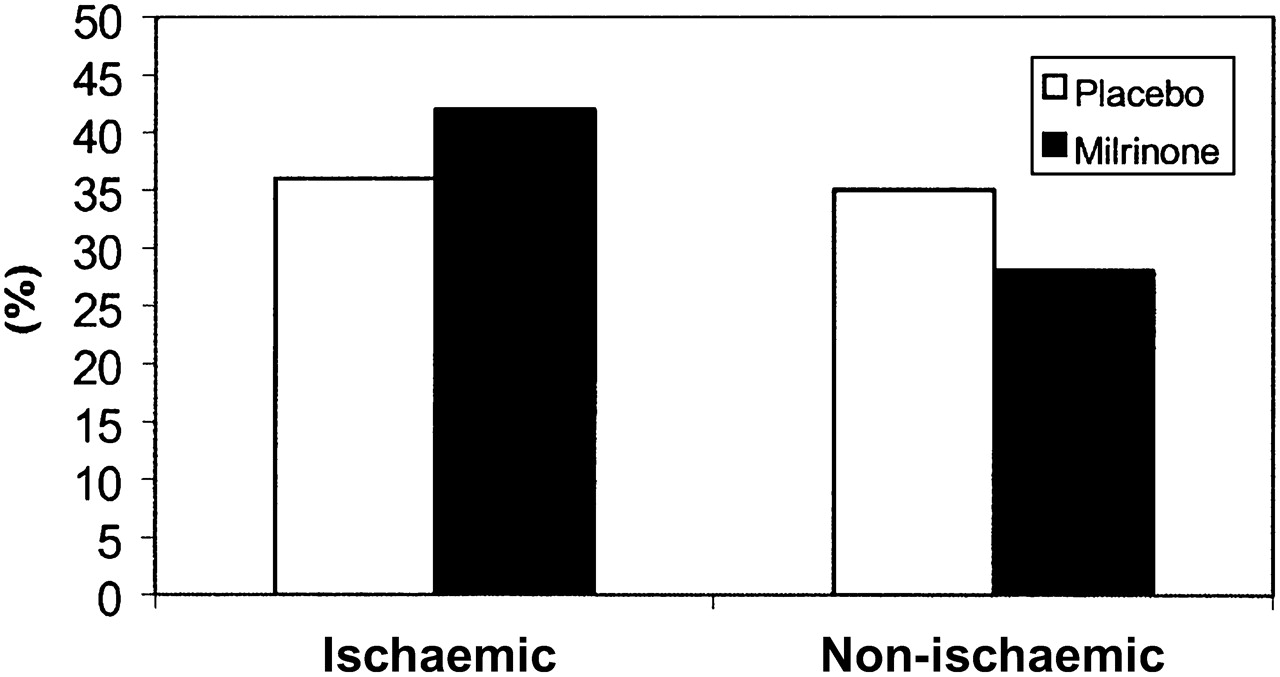
Composite end point of death + rehospitalisation by heart failure aetiology and treatment assignment. p Value=0.01 for aetiology–treatment interaction (OPTIME-CHF Study).25

Kaplan–Meier estimates (analysis of time to first event) of risk of death during first 180 days after randomisation (based on the intention-to-treat analysis) (Levosimendan Infusion versus Dobutamine study).2

Effect of dobutamine and levosimendan treatment on all-cause mortality during 180 days following the start of study drug infusion (Survival of Patients With Acute Heart Failure in Need of Intravenous Inotropic Support study).34

Kaplan–Meier estimates of survival in three groups of treatment (Vesnarinone trial study).38
Apparently, data from both registries and trials of heart failure patients suggest that even the short-term use (hours to a few days) of intravenous inotropes (except for digoxin) is associated with significant side effects such as hypotension and atrial or ventricular arrhythmias, and possibly an increase in long-term mortality.1 Enhanced contractile state and increased heart rate result in increased myocardial oxygen requirement, yielding deleterious effects in patients with ischaemic and hibernating myocardium. Besides, vasopressors and inotropic agents have the potential to cause a number of significant complications, including organ hypoperfusion (because of excessive vasoconstriction in response to vasopressors which can produce inadequate perfusion of the extremities, mesenteric organs, or kidneys), dysrhythmias (via stimulation of adrenergic receptors) and marked hyperglycaemia (possibly due to the inhibition of insulin secretion).1 Excessive vasoconstriction with inadequate perfusion commonly occurs in the setting of inadequate cardiac output or inadequate volume resuscitation. The initial findings are dusky skin changes at the tips of the fingers and/or toes, which may progress to frank necrosis with autoamputation of the digits. Compromise of the renal vascular bed may produce renal insufficiency and oliguria, while patients with underlying peripheral artery disease may develop acute limb ischaemia. Inadequate mesenteric perfusion increases the risk of gastritis, shock liver, intestinal ischaemia or translocation of gut flora with resultant bacteraemia. Despite these concerns, maintenance of MAP with vasopressors appears more effective in maintaining renal and mesenteric blood flow than allowing the MAP to drop, and maintenance of MAP with vasopressors may be life-saving despite evidence of localised hypoperfusion.47 48
What can be learnt from clinical trials on inotropes is actually parallel to the clinical observations of applying these agents for patients in need. Many patients, though showing decreased actuarial event-free survival, enjoy short-term better haemodynamic profile with improvement in exercise tolerance and overall well-being. Apart from the detrimental effects on survival, inotropes still help refractory heart failure. A few clinical observations have shown beneficial effects of inotropes in this group, either as a bridge to their next step (ie, cardiac transplantation or ventricular assist device (VAD) implantation) or as a destination therapy (home inotrope infusion therapy for cardiac transplantation/VAD ineligible patients). Though many centres have certain conditions to declare a heart failure patient appropriate for home inotrope infusion therapy, indications are yet to be defined since issues of infusion system-related complications and insurance coverage should be addressed.
Regarding these considerations, indications for administering inotropes in heart failure have been reviewed to incorporate the results of the aforementioned studies alongside the life-saving benefits of inotropes. The latest guideline from the ESC recommends that inotropic agents be administered only in patients with low systolic blood pressure or a low measured cardiac index in the presence of signs of hypoperfusion (cold, clammy skin, significant acidosis, renal impairment, liver dysfunction or impaired mentation) or congestion (Class IIa, Level of Evidence B).7 Table 1 summarises the dose and class of recommendation according to the ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008. The 2009 Focused Update into the American Heart Association/American College of Cardiology 2005 guidelines for diagnosis and management of Heart Failure recommends that clinicians should not use a specific blood pressure value that might or might not mean hypotension to dictate the use of inotropic agents. Rather, a depressed blood pressure associated with signs of poor cardiac output or hypoperfusion (eg, cold clammy skin, cool extremities, decreased urine output, altered mentation) should prompt a consideration for more aggressive therapy.49
Inotropic agents used in heart failure, dosings, class of recommendation and level of evidence for recommendation according to the European Society of Cardiology 2008 guidelines on diagnosis and management of acute and chronic heart failure7
The Heart Failure Society of America has issued a number of recommendations regarding the usage of inotropes in acute heart failure setting (table 2).50 51
Direct haemodynamic monitoring by right heart catheterisation has been advocated in the management of hospitalised patients with advanced heart failure to: (1) guide therapy by permitting direct tracking of filling pressures and systemic vascular resistance until certain specific haemodynamic goals are reached and (2) assist in understanding volume status and tissue perfusion by direct determination of the extent and type of haemodynamic abnormalities present.51 52 Despite the neutral results of the ESCAPE trial, which did not confirm the beneficial effects of haemodynamically-guided therapy in terms of short- and long-term survival,53 invasive haemodynamic monitoring will undoubtedly give clinicians invaluable information as to when to start inotrope and how to manage a patient on inotrope. Complications associated with use of intracardiac catheters include ventricular arrhythmias and line-related infection. Incorrect interpretation of haemodynamic data or overtreatment based on data may also lead to adverse outcomes.54 55
There have long been controversies as to which inotrope should be selected once the indications are met. Though the expertise of the medical team, availability and price are of great importance in this regard, there are certain issues to be considered.
According to Bristow et al, inotrope-requiring subjects with decompensated heart failure who are undergoing long-term therapy with β-blocking agents should be treated with a type III-specific phosphodiesterase inhibitor (eg, milrinone), not a β-agonist agent.59 The plot thickens when different β blockers are used. It was shown that patients with congestive heart failure on a non-selective β adrenoreceptor blocker or β1 selective blocker responded differently to the inotropic drug dobutamine: the β1 blockade caused by metoprolol could be counteracted by dobutamine, whereas with carvedilol a low dose of dobutamine increased cardiac output, and a higher dose of dobutamine caused a pressor effect.57 Another study on chronic heart failure patients on carvedilol showed statistically significant increase in left ventricular ejection fraction, significant decrease in pulmonary arterial pressure and improvement of echocardiography-derived indices with levosimendan but not with dobutamine.58 Interestingly, ß-adrenergic blockade blunted the inotropic action of both dobutamine and milrinone but not that of istaroxime in a study on chronic heart failure patients.59 Contrary to this, some observational studies have stated that concomitant use of a β-blocking agent may actually enhance the response to phosphodiesterase therapy while reducing the arrhythmia induced mortality.60
Inotrope agents can have different effects on cardiovascular system with regard to their pharmacodynamics. Dobutamine, phosphodiesterase inhibitors and lower doses of dopamine cause a prominent vasodilation of the peripheral vasculature. They can be referred to as ‘inodilators’ and best fit a heart failure setting since they help the failing heart pump against a reduced afterload, while increasing the contractility. Epinephrine, norepinephrine and higher doses of dopamine exert a more prominent vasoconstriction of the peripheral vasculature (so-called ‘vasopressors’) and are meant to increase the blood pressure in shock patients to maintain a better organ perfusion. Inodilators should be applied cautiously in heart failure patients with significant hypotension (figure 6).
Phosphodiesterase inhibitors have a special pharmacokinetic profile and need adjustments in the presence of renal insufficiency. Their actual effect may be maintained hours after discontinuation which may erroneously be interpreted as stabilisation of the clinical condition.
Though there are currently no definitive studies comparing the efficacy of combination of one inotrope or combination of inotropes over one another in terms of survival, they are sometimes used in combination with the purpose of augmenting their effects.60 There are recommendations to use combination of inotropes in immediate post open heart surgery settings; for instance, The International Society of Heart and Lung Transplantation has announced in its latest task force on Peri-Operative Care Of The Heart Transplant Recipient that continuous infusion of an inotropic agent should be used to maintain haemodynamic stability for the first 3–5 days postoperatively. Isoproterenol, isoproterenol+dopamine, dobutamine+dopamine or milrinone alone are suggested to be used at lowest effective dose and weaned as soon as possible.61

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
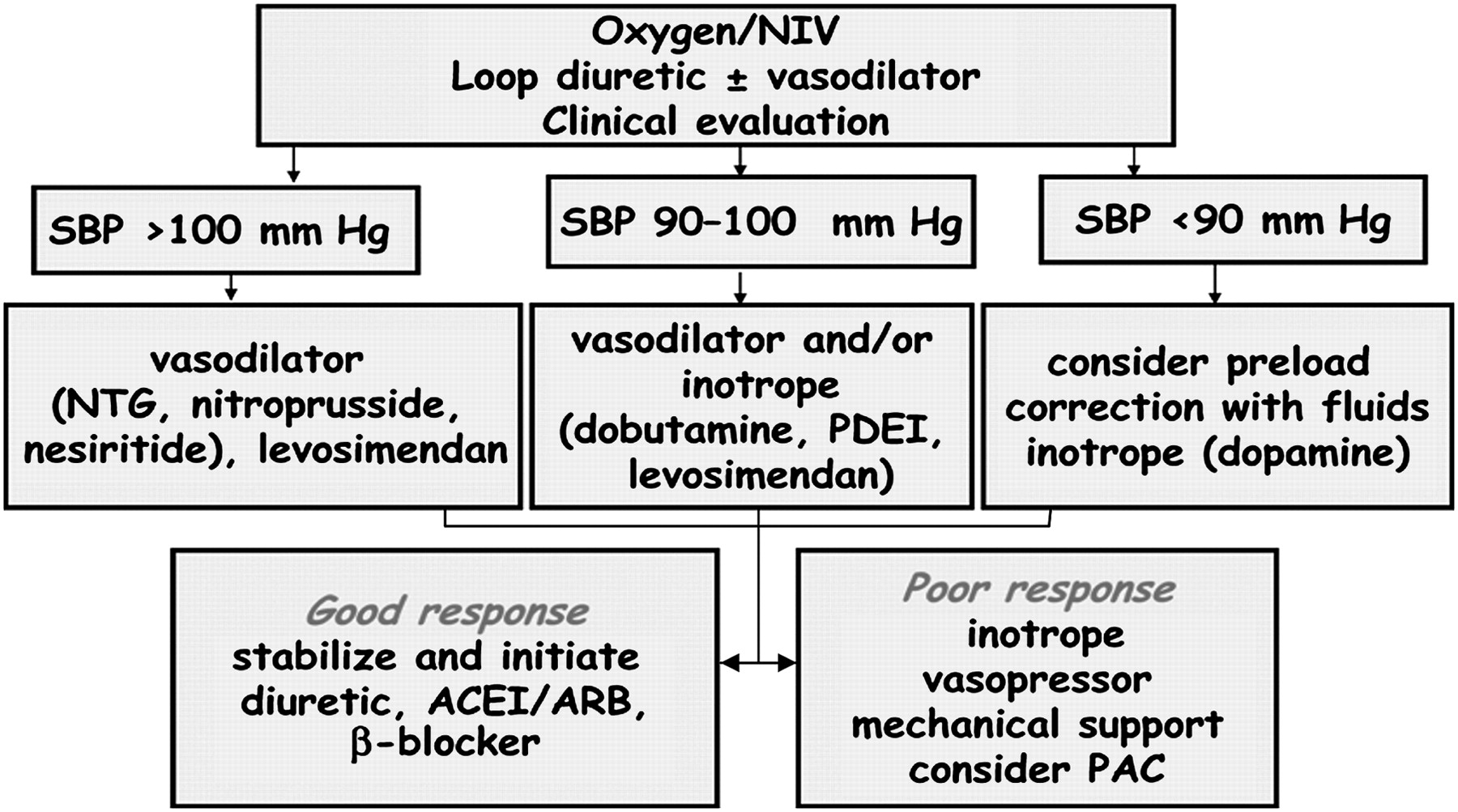
AHF treatment strategy according to systolic blood pressure as recommended by the European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic heart failure 2008.7 AHF, acute heart failure; ARB, angiotensin receptor blocker; ACEI, angiotensin converting enzyme inhibitor; NIV, non-invasive ventilation; NTG, nitoglycerine; PAC, pulmonary artery catheterization; PDEI, phosphoDiesterase inhibitor; SBP, systolic blood pressure.
In summary, positive inotropes have long been considered promising in the management of patients with heart failure; however, certain study results have highlighted their potential side effects. In order to have fewer such detrimental effects, clinicians should address those heart failure patients who would benefit most from these agents. They must be used as short in duration and as low in dose as possible. Heart failure guidelines have provided clinicians with valuable data for better applying inotropes in heart failure settings. Implementing their recommendations will, therefore, increase the advantages and reduce the side effects.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.