Article Text

Abstract
Objective The aim of the study was to assess the differences in clinical and morphologic characteristics of culprit lesions among patients with unstable angina (UA) and non-ST-elevation myocardial infarction (NSTEMI).
Methods The authors included 174 consecutive patients who have been admitted due to UA or NSTEMI. All patients underwent coronary angiography during hospitalisation and angiographic characteristics were determined.
Results The mean age of study patients was 57±9 years, and the majority were men. The frequency of single, two and three vessel disease was 35.6%, 28.7% and 28.1%, respectively. There was no significant difference between UA and NSTEMI patients in terms of the extent of coronary artery involvement and culprit lesion morphologic features (p value: 0.99 and 0.67, respectively). The only significant difference was the incidence of definite and possible thrombus in culprit lesion (40.7% vs 16.5%, p value<0.001). The authors also did not find any association between Braunwald clinical/severity classification and lesion morphology in the studied population. In multivariate analysis there was a significant association between Braunwald class II–III and increased risk of NSTEMI (OR (95% CI): 13.43 (1.12 to 160.63), p=0.04, OR (95% CI): 14.08 (1.21 to 163.11), p=0.03, for Braunwald severity class II and III, respectively).
Conclusion Clinical characteristics of patients with acute coronary syndrome including enzyme rising cannot predict the extent of coronary artery involvement and the morphology of culprit lesions. The only exception was the higher incidence of intracoronary thrombus in patients with NSTEMI as compared with UA.
- Culprit lesion
- coronary angiography
- acute coronary syndrome
- coronary artery disease
- coronary physiology
- coronary flow
Statistics from Altmetric.com
- Culprit lesion
- coronary angiography
- acute coronary syndrome
- coronary artery disease
- coronary physiology
- coronary flow
Introduction
Acute coronary syndromes (ACS) including unstable angina (UA), non-ST-elevation myocardial infarction (NSTEMI) and ST-segment-elevation myocardial infarction (STEMI) are major causes of death, morbidities and hospitalisation worldwide.1 2 Compared with patients with STEMI, early mortality is somewhat lower in UA and NSTEMI (non-ST-elevation ACS; NSTE-ACS) but in the long-term, these patients have a higher chance for recurrent ischaemic events and cardiac death.3 Five mechanisms are responsible for development of NSTE-ACS including plaque rupture or erosion, dynamic obstruction, progressive growth of a stable plaque, inflammation and increased myocardial oxygen demand. Among them, the major aetiological mechanism is rupture and ulceration of an unstable plaque (culprit lesion) which initiates activation of platelets and coagulation factors and leads to development of a critical stenosis in the culprit vessel and subsequent ischaemic events.4
Patients can also be divided according to elevations of markers of myocardial necrosis. Patients with elevated creatine kinase isoenzyme-MB or cardiac-specific troponin T or I constitute the NSTEMI group and have an increased risk of events while those with normal cardiac enzymes are referred as UA and may have a more favourable prognosis in the short-term.
Braunwald has proposed a simple classification of NSTE-ACS based on clinical characteristics of the patients.5 This classification system has been shown to be correlated with prognosis and can also predict some angiographic features of the culprit lesion.6 Recent onset of angina (within 48 h), secondary angina and post-myocardial infarction (MI) status carry a higher risk of adverse events according to this classification. Another important factor in evaluation of NSTE-ACS patients is the extent of coronary involvement and morphology of lesions according to American College of Cardiology/American Heart Association (ACC/AHA) classification.7 Culprit lesions are generally eccentric, ulcerated and contain thrombus.8–10 It has also been shown that morphology of the culprit and other significant lesions is a major determinant of choosing the appropriate treatment strategy and could have a significant impact on the long-term prognosis.
This study aimed to evaluate the clinical characteristics, angiographic features and procedural outcomes of patients with UA/NSTEMI and assess the relationship between Braunwald clinical/severity classification and culprit lesion characteristics according to ACC/AHA classification system for both NSTEMI and UA.
Methods
Patient selection and study protocol
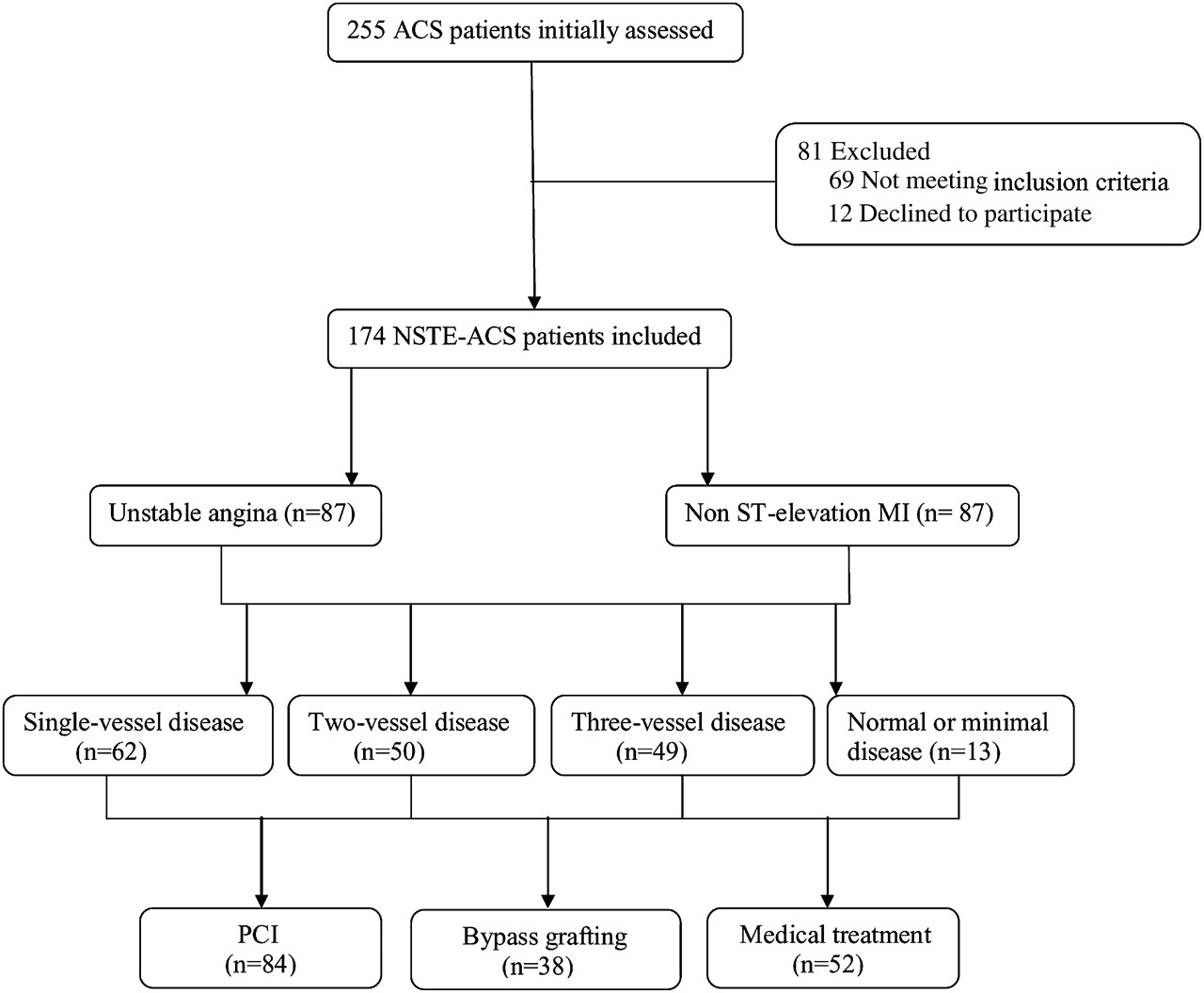
Of initially assessed 255 patients, we prospectively included 174 consecutive patients who had been admitted due to UA or NSTEMI if they were >18 years of age and underwent coronary angiography during the index hospitalisation based on an early invasive strategy. Exclusion criteria were: patients with STEMI except for those with post-MI angina; cardiogenic shock at the time of presentation; previous percutaneous coronary intervention (PCI) or surgical bypass graft; catheterisation beyond the first 48 h of admission; and pregnancy. All patients provided written informed consent. The patients were categorised according to Braunwald severity and clinical classifications. Coronary angiography was performed using a standard technique. Two experienced investigators blinded to the clinical data analysed the angiograms and angiographic characteristics such as number of vessels with significant (>50%) stenosis, thrombolysis in myocardial infarction (TIMI) flow in the culprit vessel, culprit lesion morphology and ACC/AHA lesion typing were determined. We also compared the angiographic characteristics between UA and NSTEMI patients. Agreement between investigators was satisfactory (Cohen's κ =0.86, 95% CI 0.79 to 0.92). In case of disagreement, the final decision was taken by consensus. In patients with single vessel disease, the most severe stenosis in involved artery was considered as culprit lesion. In patients with two or three vessel coronary artery disease, culprit lesion was attributed to the most significant lesion in the artery presumed to be responsible for dynamic electrocardiographic changes. In the absence of dynamic electrocardiographic changes, the severity and morphology of the plaques, reviewing events in the past, echocardiographic region of the most severe wall motion abnormality and possible previous angiogram were all taken into account to find responsible stenosis.
The treatment strategies based on the angiographic findings were also analysed. The patients would undergo PCI of the culprit lesion and other severe stenoses if lesion anatomy was suitable and full revascularisation was feasible. In the case of multiple stenoses, surgical bypass was preferred.
We also analysed the relationship between clinical classification of UA/NSTEMI and culprit lesion characteristics and optimal treatment option in the studied population.
Statistical analysis
Demographic and angiographic data were expressed as mean±SD or median. For comparison of left ventricular function, serum creatinine and culprit lesion stenosis in the UA and NSTEMI groups, Mann–Whitney U test was used. Comparing of other demographic factors in the two groups was done with Fisher's exact test or Pearson' χ2. Analysis of the relationship between Braunwald UA classification and angiographic factors such as number of diseased vessels, thrombus and TIMI flow and also procedural outcome of patients was performed using Kruskal–Wallis test. Multivariate analysis was also performed using logistic regression model.
Limitations
An important limitation of this study was the insufficient number of patients in some subgroups of Braunwald clinical or severity classifications. As discussed later, this may have a negative impact on the power of the study to predict a significant relationship between these classifications and angiographic features or procedural outcome of the patients.
Results
Patient characteristics
One hundred and seventy-four patients (46 women; mean age=57±9 years, range: 33–81 years) participated in the study. Hypertension was the most common risk factor in our patients (52.3%) followed by dyslipidaemia (42.5%). Mean left ventricular ejection fraction was 45%. Table 1 shows the demographic characteristics of the studied population. Fifty per cent of our patients (n=87) presented with UA and the remainder with NSTEMI.
Demographic characteristics in the whole patients and comparison between UA and NSTEMI patients
Regarding their clinical presentation, 69 patients (39.7%) were categorised as class II Braunwald severity classification (resting chest pain more than 48 h before admission) and 95 (54.6%) as class III (resting cheat pain <48 h). Only 10 patients (5.7%) had a class I presentation.
The patients were also classified according to Braunwald clinical classification. In all, 129 (74.1%) were in class B group (primary angina without recent MI) and 39 (22.4%) were in class C (post-MI angina). Only six patients (3.4%) were classified as secondary angina or Braunwald class A. Analysis showed no significant difference between UA and NSTEMI groups according to these classifications (table 2).
Number of patients in different UA classes in the overall patients and in UA versus NSTEMI separately
Procedural characteristics
Table 3 shows the result of angiographic study in the patients. The frequency of single, two and three vessel disease was 35.6%, 28.7% and 28.1%, respectively. Four patients (2.3%) had significant left main stenosis. The remainder of the patients (7.5%) had minimal CAD or normal epicardial coronary arteries in the angiography. The culprit lesion per cent stenosis was 88±12% in the overall study group. We did not find a significant difference between UA and NSTEMI groups regarding severity of stenosis but there was a trend towards higher degrees of diameter stenosis in NSTEMI patients (p value: 0.05).
Angiographic characteristics in the studied population and in UA versus NSTEMI separately
TIMI flow grading was performed for the culprit and other significant lesions. TIMI flow grade 0 or 1 was found in 10.6% of the culprit lesions, and TIMI grade 2 in 13.7%. Frequency of patients with abnormal TIMI flow grade was not different in the two groups (p value: 0.35).
The characteristics of the culprit lesions were also analysed. Out of 160 lesions, 12 (7.5%) were type A according to AHA/ACC lesion classification. Type B and C lesions were present in 64.3% and 28.1% of the culprit lesions, respectively (table 4). No significant difference was found between UA and NSTEMI patients in terms of AHA/ACC lesion typing.
Culprit lesion characteristics in the studied population
Thrombus was present in 28.8% of the culprit lesions in overall patients. Intracoronary thrombus was defined as definite if it was globular, partly separated from vessel wall or mobile. Possible thrombus was defined as linear and hazy irregularity lying on top of atheromatous plaque. Definite and possible thrombus were present in 8.7% and 20% of the patients, respectively. Thrombotic lesions in the NSTEMI group were significantly more prevalent than UA patients (40.7% vs 16.5%, p value <0.001). Significant calcification and tortuosity was detected in 5% and 4.3% of the culprit lesions in the whole study population.
Treatment strategies
Treatment recommendation was based on the angiographic findings (figure 1). Bypass surgery was performed in 21.8%. PCI on the culprit or other significant lesions was carried out in 48.3% of the patients in the hospitalisation index or later (table 5). Timing of the intervention was based on several factors such as: number of the vessels with significant stenosis, feasibility of PCI on the culprit lesion, baseline kidney function, symptomatic status and so on. Generally, it was preferred to revascularise the culprit lesion and if possible other significant lesions at the time of first angiography to reduce future events, but in some patients staged approach was selected due to specific clinical considerations.

{kind=link}
Treatment strategies in the studied population. ACS, acute coronary syndromes; NSTE-ACS, non-ST-elevation ACS; PCI, percutaneous coronary intervention.
Angiographic findings and procedural outcome in different clinical/severity classes of studied population
Stenting was performed in 100% of patients in the PCI group. Out of 84 patients in whom stenting was performed, 19 (22.6%) received one or more drug eluting stents. The rest of the patients (77.4%) received bare metal stent. Procedural success was 97.7% in the PCI group. TIMI 0, 1 after the procedure was present in one patient. Analysis showed no significant difference between UA and NSTEMI groups with regard to treatment strategy and procedural success during PCI.
The association between clinical classification of UA/NSTEMI and angiographic findings has also been evaluated (table 5). There was no significant association between Braunwald clinical/severity classifications and angiographic findings such as number of diseased vessels, TIMI flow, thrombus and calcification in the culprit lesion.
We also did not find any significant association between Braunwald classification and procedural outcome in the population studied (table 5).
Multivariate analysis
Multivariate analysis using logistic regression model showed a strong association among the presence of thrombus (OR (95% CI): 3.7 (1.47 to 9.22), p=0.005), Braunwald class II (OR (95% CI): 13.43 (1.12 to 160.63), p=0.04), Braunwald class III (OR (95% CI): 14.08 (1.21 to 163.11), p=0.03) and smoking (OR (95% CI): 2.71 (0.87 to 8.43), p=0.08) with NSTEMI (table 6). Also, there was a weak association between high degree stenosis of culprit lesion and NSTEMI (OR (95% CI): 1.08 (1.01 to 1.15), p=0.01).
Multivariate logistic regression model
Discussion
As mentioned above, in our study there was no significant difference between NSTEMI and UA patients in terms of demographic or angiographic characteristics except for thrombus in the culprit lesion. Although myocardial injury is more extensive in NSTEMI, it is not necessarily due to the presence of more extensive coronary artery involvement or more severe stenosis in the culprit lesion. In fact, the extent of myocardial injury is influenced by many factors such as dynamic obstruction, myocardial preconditioning, microvascular dysfunction, presence of collaterals and extracardiac factors such as anaemia, infection and hypoxaemia.11–14 On the other hand, even moderate lesions may cause acute injury in the subtending region if they get complicated by rupture, fissuring or vasospasm. So, the degree of culprit lesion stenosis is not the sole determinant of extent of myocardial injury and subsequent enzyme rising. Increased frequency of intracoronary thrombus—either definite or possible—in the NSTEMI group reflects higher degrees of acute complications in the culprit lesion and can increase the chance of myocardial necrosis in several ways, including:
creating temporary thrombotic occlusion of the culprit vessel
distal embolisation of thrombotic material
thrombin-mediated vasoconstriction in the epicardial or intramyocardial arteries.15
The rate of intracoronary thrombus in this study was lower than the previous studies. For instance, TIMI IIIA study reported definite intracoronary thrombus in 47% and 29% of patients with NSTEMI and UA, respectively. This difference may be due to more frequent use of medications such as enoxaparin, clopidogrel and GPIIb/IIIa receptor antagonists in contemporary practice or may relate to the duration of anticoagulation therapy before angiographic study. Whatever the absolute frequency of intracoronary thrombus in these patients, it seems that NSTEMI patients have an increased rate of thrombotic lesions in diagnostic angiography.
Multivariate analysis showed a significant association between smoking and NSTEMI. This association is in accordance with previous studies that demonstrated an increased risk of ischaemic adverse events in smokers.16 17 In multivariate analysis there was also a significant association between Braunwald class II–III and increased risk of NSTEMI. This finding confirms the role of this classification in risk stratification of patients with ACS.
The association between clinical classifications of UA/NSTEMI and morphologic features of culprit lesion and procedural outcome was also evaluated in this study. No significant association between the above mentioned items was noticeable. On the other hand; it seems that this study does not have enough power to assess all aspects of this relationship. In fact, subgroups such as class I or class A patients were low in number because many of such patients underwent non-invasive tests before angiography and significant ischaemia was ruled out. As a result, only a few patients of these types were included in the study and this may have a negative impact on the power of the analysis. Despite these limitations, the p values for association analysis are in a range that any significant relationship seems to be unlikely even if the numbers of patients in the subgroups are increased. In other studies, Braunwald classification was an independent predictor of intracoronary thrombus in the culprit lesion.
Clinical implication of the study
Apart from the association with coronary thrombus, this classification has not been shown to predict lesion morphology or the number of vessels with significant stenosis. Likewise, the treatment strategy could not be predicted using this clinical classification. The main purpose of this classification, evidently, is clinical risk stratification and not prediction of morphology or treatment strategy. So, if a patient is classified as high-risk according to Braunwald classification, early angiography is recommended to delineate the anatomy of coronary arteries and direct the treatment strategy.
Conclusion
ACS constitutes a heterogeneous group of patients. Braunwald classification has been used to classify these patients for better clinical risk stratification. No significant association was found between this classification and ACC/AHA lesion typing or treatment strategy after angiography. On the other hand, patients with NSTEMI had a higher incidence of intracoronary thrombus in this study as compared with UA. Larger studies are needed for a better assessment of the association between culprit lesion morphology and clinical characteristics in patients with ACS.
Acknowledgments
The authors would like to thank Dr Hooman Bakhshandeh for his critical review of the manuscript.
References
Footnotes
Competing interest None declared.
Patient consent Obtained.
Ethics approval This study has been approved by the ethical committee of Rajaie cardiovascular medical and research center.
Provenance and peer review Not commissioned; externally peer reviewed.