Article Text

Statistics from Altmetric.com
A 45-year-old man with a history of hypereosinophilic syndrome and bronchial asthma was admitted to our department for ischaemic heart disease examination. When he was 24 years old, he was diagnosed of hypereosinophilic syndrome with an extremely high (6517/μl) eosinophil count; however, the count gradually decreased in response to treatment with oral steroids and hydroxyurea. The patient had history of smoking.
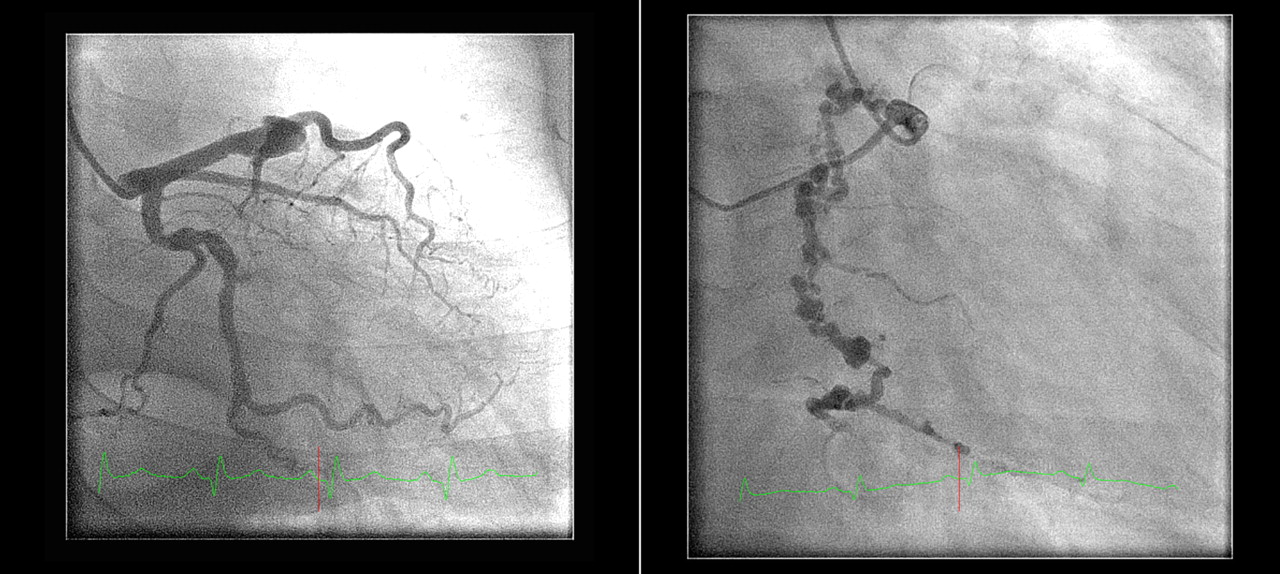
Electrocardiogram showed abnormal Q wave and flat T wave in leads II, III, aVF. Echocardiography showed hypokinesis and wall thinning at inferior, posterior and lateral wall of left ventricle, suggesting old myocardial infarction. Coronary angiography revealed diffuse moniliform formation of the entire right coronary artery, large aneurysm at the mid left anterior descending artery, ecstatic change at left circumflex artery, and occlusion at distal right coronary artery and diagonal branch of left anterior descending artery (figure 1). From multi-detector-row CT images, vessel diameter of coronary aneurysm at segment 6 was approximately 20 mm. Intra-vascular space was mainly occupied with thrombus, but no stenotic lesion was detected in the aneurysm (figure 2A). Systemic CT scan detected aneurysm of common hepatic artery, splenic artery and right superficial femoral artery (figure 2B–D, common hepatic artery was occluded). The patient met part of the diagnostic criteria for Churg-Strauss syndrome without any pathological material.1

{kind=link}
{kind=link}
Although Churg-Strauss syndrome is accompanied by vasculitis, hypereosinophilia per se reportedly causes coronary artery aneurysms.2 In addition to common atherosclerosis risk factors, long exposure to hypereosinophilia was suspected to contribute to advancement of arterial aneurysms via eosinophil cytotoxicity.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.