Article Text

Statistics from Altmetric.com
Images in cardiology
A 77-year-old man was investigated following three episodes of unexplained transient loss of consciousness (TLoC) over 8 months. According to eyewitnesses, each episode would start suddenly with blank facial expressions, followed by rapid onset of pallor. Loss of consciousness would ensue, associated with twitching of the limbs for several minutes. On regaining consciousness, the patient would be incoherent and amnesic. There was no history of incontinence or tongue biting. Routine blood tests, 12-lead electrocardiogram, ambulatory cardiac monitoring and EEG were normal. Magnetic resonance brain imaging showed old cerebral infarcts.
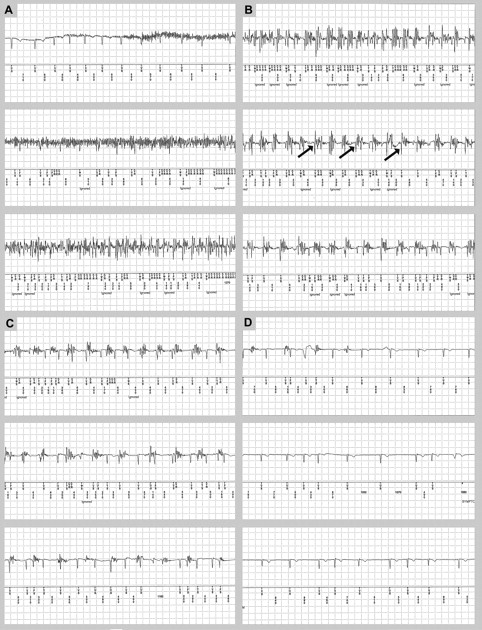
The patient underwent loop recorder implantation (ILR) (Reveal®DX9528, Medtronic Inc, Minneapolis, MN, USA) following which, within 6 months, he experienced two further TLoC episodes. ILR tracings showed sinus rhythm (80 bpm), accelerating to sinus tachycardia (120 bpm) (figure 1A) followed by 18 s of sustained, rapid, high-frequency myopotentials characteristic of a tonic phase. This was followed by 39 s of periodic bursts of high-frequency myopotentials, with decreasing burst frequency, characteristic of a clonic phase (figure 1B,C). Normal ventricular activation (QRS complexes) were seen within the clonic artefacts (arrows) (figure 1B). Based on these appearances, which were typical of tonic-clonic seizures, an absence of arrhythmias and the rarity of tonic-clonic seizures with ‘convulsive’ syncope, a diagnosis of generalised epilepsy was made. The patient was commenced on lamotrigine, and after 9 months follow up, has had no further episodes.
{kind=link}
Continuous implantable ECG loop recorder tracing showing features of generalised tonic-clonic epilepsy during an episode of transient loss of consciousness, paper speed 25 mm/s. Sinus rhythm (80 bpm), accelerating to sinus tachycardia (120 bpm) (A) followed by 18 s of sustained, rapid, high-frequency myopotentials, characteristic of a tonic phase, followed by 39 s of periodic bursts of high-frequency myopotentials, with decreasing burst frequency, characteristic of a clonic phase (B, C). (B) Normal QRS complexes were seen within the clonic artefacts (arrows). (D) Sinus rhythm with no artefacts following resolution of the tonic-clonic seizure.
An ILR is known to be valuable in diagnosing arrhythmias causing unexplained TLoC, but as our image demonstrates, unexpectedly and rarely, it can also help in diagnosing epilepsy.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.