Article Text

Abstract
Background Anatomical obstructions are the bane of radial access site for coronary procedures for inexperienced operators. The availability of better hardware in the performance of procedures by this route has mitigated this problem. Arteria lusoria (AL) is a congenital anomaly which predisposes to access site crossover during the early phase of the learning curve. We present our experience in the performance of radial access site coronary angiographies of these patients, which is the first such study reported in literature.
Materials and methods Retrospective analysis of 5879 patients from August 2006 to August 2012 was done with special attention to preprocedural and peri-procedural parameters in patients with AL. Analysis of the angle made by the aberrant vessel with the arch of aorta is also noted. Comparisons were made with timings of radial angiography as reported by Looi et al. Comparison was made of the time taken to complete the procedure by the operator vis-a vis the time taken during earlier performance of the procedure in these patients by the same operator.
Results The incidence of AL is 0.5%. The total time taken for the procedure is 18.1+6.9 min and the total fluoroscopy time needed is 4.0+2.7 min. Comparisons with the study conducted by Looi et al reveal no statistical significance between the times (p>0.05). When stratified with respect to the experience of the performing operator, there was significant difference (p<0.001) in the total time taken and the total fluoroscopy time required for the procedure when performed with experience of previous angiographies via the radial route. The aberrant vessel made an angle of 45° on an average with the arch of aorta. With experience, the number of guiding catheters needed for the procedure decreased from four to one and the operator was able to perform the procedure with the same catheter. Peri-procedural complications of vasospasm and minor bleeds were the only ones to attain statistically significant increase in these patients (p<0.05) and were related to higher duration of the procedure and unrelated to the age and sex of the patient.
Conclusions AL is not a contraindication to the performance of coronary angiography. Experience of the operator helps in achieving procedure and fluoroscopy times akin to that of routine radial angiography.
- Coronary Artery Disease
Statistics from Altmetric.com
Introduction
Radial artery interventions have been acquiring increasing importance in the field of interventional cardiology since their inception in the year 1989 after the ‘first in man attempt’ by Campeau.1 The use of this procedure in various aspects of interventional cardiology has expanded since and has only been limited by the presence of anatomical variations which preclude the use of routine hardware used via the femoral route.2 ,3 These anatomical variations have had a 2.9% failure rate for the procedure causing a shift to the femoral route.
We present a case series of 31 such patients in our experience of 5789 patients over 6 years of radial artery interventions. These patients, owing to the rare anomaly of arteria lusoria (AL), an arterial variant of the branches of the aortic arch occurring in 0.2%–1.7% of the population, had to have a shift over to the femoral route for further intervention despite having successful angiograms. Of late, the advent of specialised radial hardware has facilitated the performance of angioplasties also via the same route. However, data comparing the femoral and radial route in this group of patients are not available.
Materials and methods
Study patients
From August 2006 to August 2012, a total of 5789 consecutive patients with normal Allen's test underwent radial angiography at our centre with percutaneous transluminal coronary angioplasty and stenting done in those patients when indicated. A retrospective study of the angiograms of these patients was carried out to evaluate for the presence of AL and an analysis was made regarding the complications faced by the operator as regards the performance of the angiograms in these patients. An analysis of the route taken when faced with this arterial anomaly was also done.
Definition of AL
The anomaly of AL was determined on angiography of the aortic arch during difficult radial angiography procedures, as evidenced by the origin of the right subclavian artery from the aortic arch after the origin of the left subclavian artery.
Parameters evaluated in patients with AL
In patients whose aortic angiograms were suggestive of AL, further parameters were evaluated. History related to the additional evidence of alternative site atherosclerosis like transient ischemic attacks, peripheral arterial disease or coexistent diabetes was acquired. Any history of dysphagia in the patient was noted. Precatheter echo parameters and ECG findings, procedural parameters in the form of time taken for the procedure, time for fluoroscopy, number of catheters used, angle between the aberrant artery and the aortic arch, associated upper limb arterial tortuosity, vasospasm of the arterial tree up to the aorta and postprocedural parameters like major and minor bleeds, Volkmann's ischaemia/contracture, and forearm haematomas. Definitions of major and minor bleeds were used as in the RIVAL study.4 If there was a presence of vasospasm during the procedure, the duration of the same and method used to treat it was noted.
Data analysis
Calculations regarding the angle of the aberrant artery with the aortic arch were done on the recorded angiogram.
The baseline characteristics of the patients were noted. The prevalence was calculated among the total procedures performed. For data analysis, the patients having AL were classified into six groups depending on the experience of the performing operator at the time of performing the procedure, in slabs of 1000 procedures, and all further analysis of the time taken was performed on this model. The mean and the SD of the total time taken and the total fluoroscopy time were calculated. Unpaired t test was used for the calculation of the significance of effect of the operator's experience on the total time and the fluoroscopy time on the procedure as well as comparison with standard radial angiography procedure and fluoroscopy time as given by a study conducted by Looi et al5 in 2011 in the American Journal of Cardiology. Paired t test was used to evaluate the significance of the angle of the aberrant artery with the aorta. Complications encountered during the procedure were noted and their relative percentage was calculated.
Results
Baseline data
The baseline data revealing the details of the patients undergoing coronary angiography via the radial route despite the presence of AL are detailed in table 1. The group mainly consists of men in the age group between 56.6 and 66.4 years undergoing routine coronary angiography after acute coronary syndrome. The OR for the contribution of the various associated comorbidities to the detection of AL was not significant. Ulnar pulsations and adequate palmar arch flow were seen in all the patients.
Baseline clinical characteristics of patients undergoing coronary angiography in patients with arteria lusoria via the radial route
Procedural and postprocedural data
The details of the procedural and postprocedural data are summarised in table 2.
Intraprocedural and postprocedural data in patients undergoing radial access for coronary angiography in patients with arteria lusoria
The total time taken for the procedure was 18.1±6.9 min with 7±2.7 min taken as for fluoroscopic manipulation. When stratified on basis of the experience of the operator in performing coronary angiography by the radial route of access, there is the expected trend of decreasing times needed, both for the total procedure and for the fluoroscopy time. There is significant difference in the times taken (p<0.001) for the performance of the procedure, when compared with intrastudy controls, represented by the times needed by the operator when in the last quintile of procedures. Initially the number of catheters needed to be changed over the wire for the completion of the procedure is high which with better experience and high index of suspicion is reduced to using the same catheter for the entire procedure. The mean angle with the horizontal plane of the aortic arch, made by the aberrant Subclavian artery is 45°. No significant association with the associated sites of tortuosity is present in these patients.
These patients have a higher incidence of complications as compared to routine patients undergoing radial access for coronary angiography and significance to the intraprocedural vasospasm and postprocedural minor bleeds is attained. No significant changes in the other postprocedural events are noted.
Discussion
Radial artery access is a very convenient and patient friendly route for performance of coronary artery interventions.2 ,3 Performing the intervention in cases of AL is also not a big scare or issue in case of an experienced operator and does not need access site changeover. The superficial location of the vessel at the wrist allows for easy haemostasis thereby virtually eliminating access site complications. Overall, 0.7% of all coronary angiographies and 1.1% of all coronary interventions fail owing to severe tortuosity of subclavian artery. No study has focused on the incidence of AL in this group.
Comparisons of the total procedural and fluoroscopy times taken for the completion of the procedure via the radial access site in the study by Looi et al did not show any significant difference in the performance of the procedure or in the total fluoroscopy time. Intrastudy stratification of the times taken for the performance of the procedure depict a decrease in the total procedure time and fluoroscopy time consistent with better experience of the performing operator.
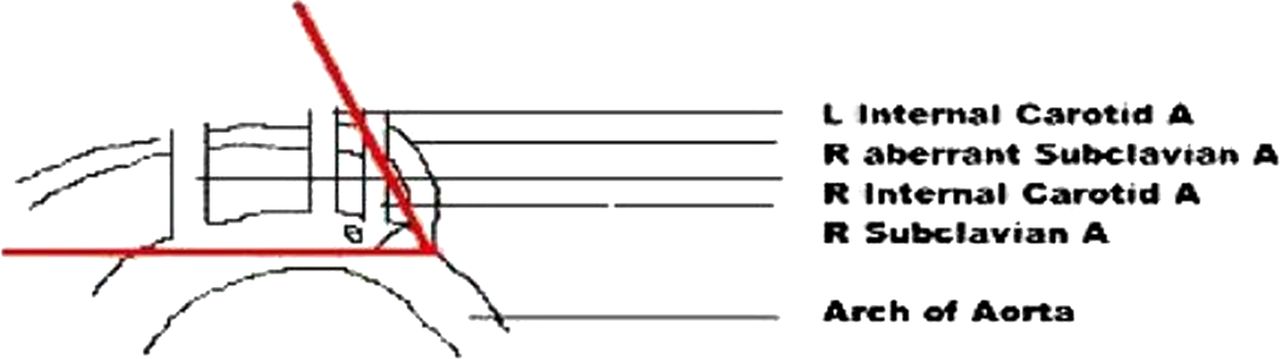
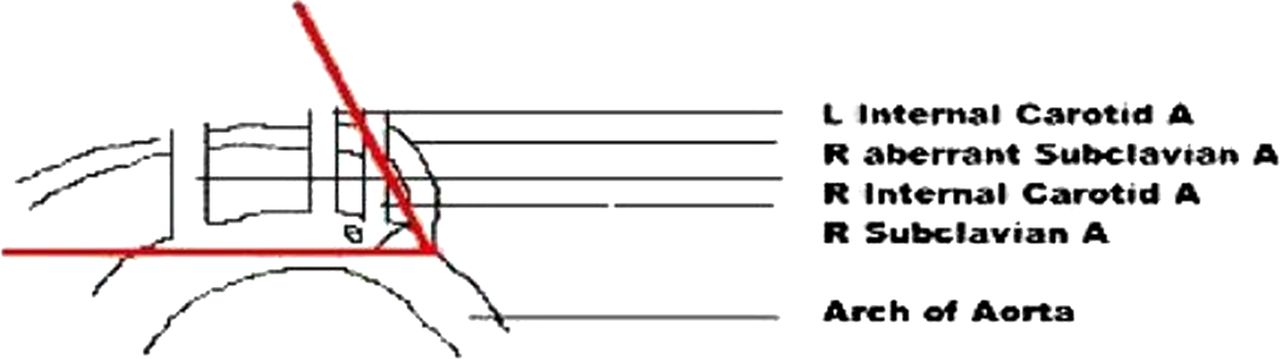
Requirement of change in catheters during the performance of procedure is also minimised with increasing experience as there is an improvement in the manoeuvring of the catheter by the operator. The angle Θ made by the aberrant vessel with the arch of aorta is approximately 45±5° (figure 1). This angle usually directs entry of the catheter into the descending aorta. The technique used at our centre is to withdraw the guidewire into the guiding catheter and allow the natural curve of the Tiger catheter to direct the guidewire into the arch of aorta and further into the ascending aorta. Additional techniques are to take deep breaths, hold the breath in inspiration and road-mapping of the origin of the aberrant subclavian vessel to help in the completion of the procedure.
{kind=link}
Diagram of the angle Θ made by the aberrant subclavian A with the arch of aorta.
Limitations of the study
-
Our study is a review of the transradial procedures conducted in patients of AL at our centre. This being a primary radial access centre, intrahospital comparisons between transfemoral angiography (TFA) and transradial angiography were not possible owing to the relative paucity of TFA coronary procedures. We have had to rely upon results of other studies whose protocols and procedure profile may not have an accurate match with that at our centre.
-
There has been an absence of regular follow-up of these patients at 30 days for detection of the radial artery patency, owing to the predominantly rural and uneducated profile of the population under study, and so the rates of delayed closure of the radial artery cannot be estimated in that subset of patients.
-
In these patients, we do not have data on coronary interventions, which may be the step ahead for evaluating the radial access route in these patients.
Conclusions
AL is an entity encountered rarely on clinical grounds. However, with the growing use of the radial artery for interventions, it has assumed significance owing to switch over of access sites. Our observational study shows that there is no need to change over at the stage of performing a routine angiogram and, as with all radial interventions, shows a learning curve with the improvement in the performance of the procedure with increasing experience. The time taken for the procedure is comparable with routine procedures albeit with an increase in minor complications all of which can be safely managed. Thus, this route may be safely used as an access site for the performance of coronary angiographies even in the presence of this most severe arterial tortuosity of the subclavian artery including AL.
Footnotes
-
Contributors RKG performed the procedures and gave the concept of the paper as well as proofread the paper. DP performed the review, wrote the paper and analysed the findings. DB and SG were responsible for the ethics committee approval, the data collection and statistical analysis.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics committee, J.L.N. Medical College, Ajmer.
-
Provenance and peer review Not commissioned; externally peer reviewed.