Article Text

Statistics from Altmetric.com
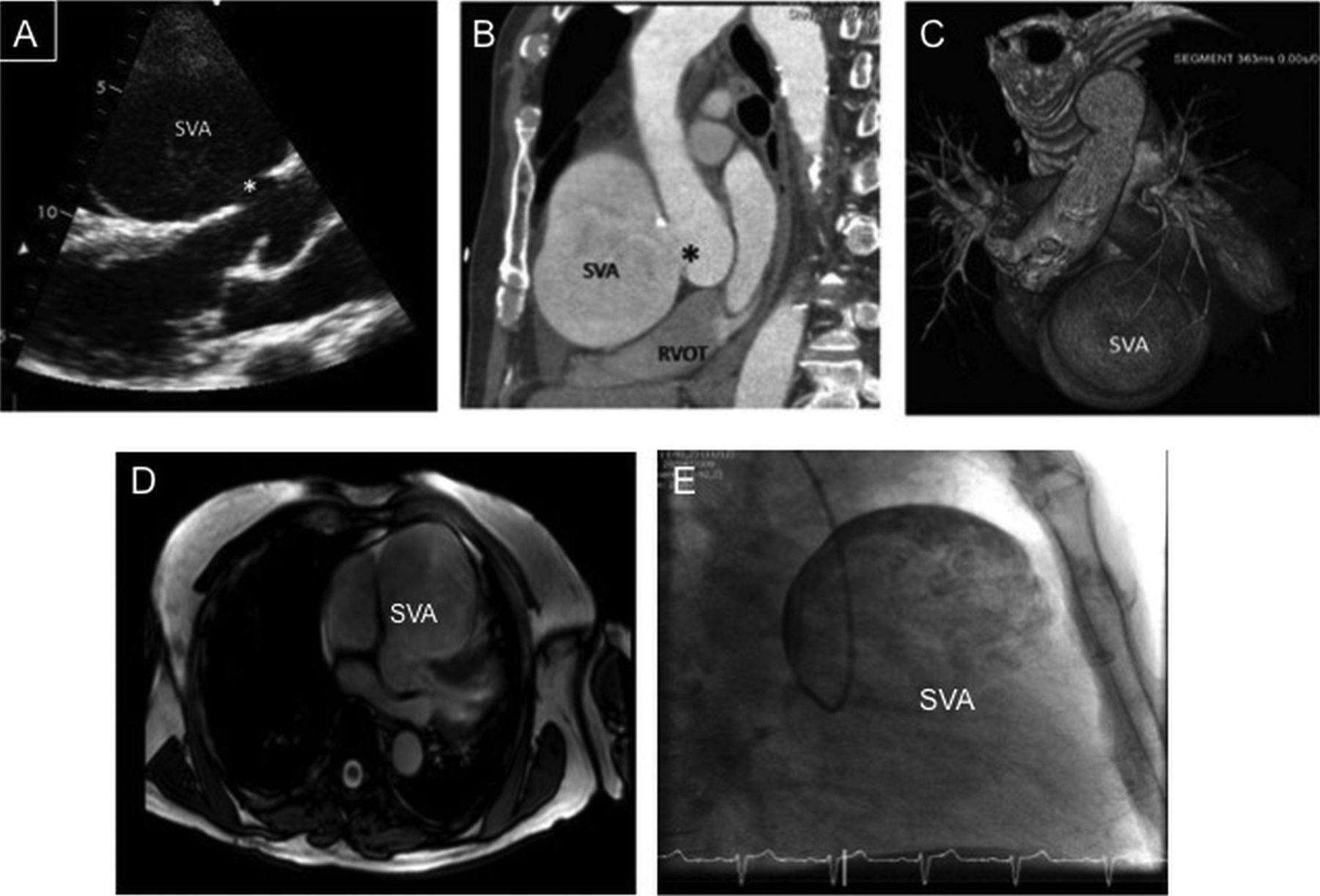
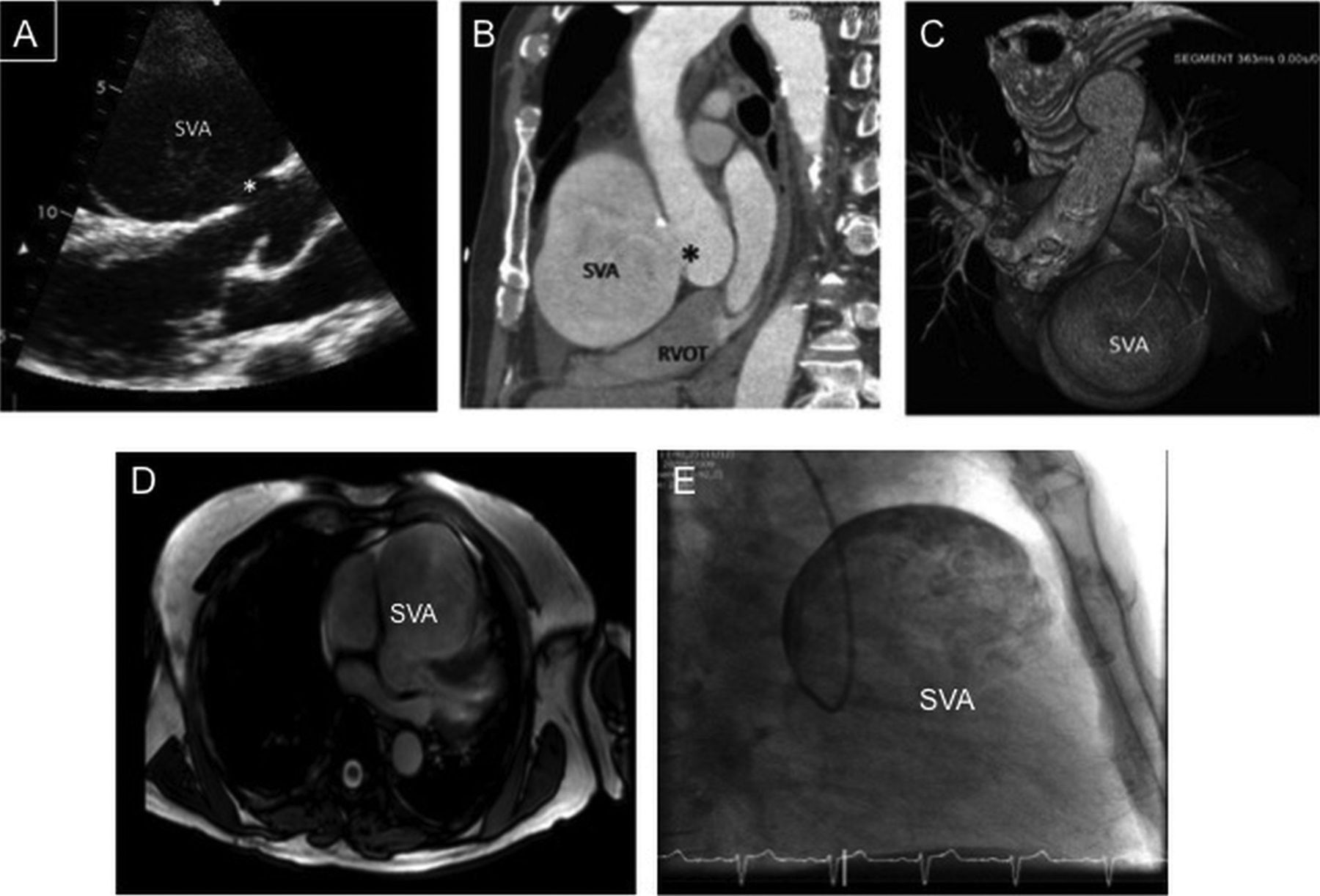
An 82-year-old man presented with severe exertional breathlessness to the outpatient clinic. Previous medical history included hypertension and transient ischaemic attack. During routine workup, transthoracic echocardiography was performed. A large defect (*) in the anterior wall of the aortic sinus of Valsalva was identified (figure 1A) which extended into a cavity containing spontaneous echo-contrast (see online supplementary data video S1). Further imaging by CT with three-dimensional reconstruction (figure 1B,C) and cardiac magnetic resonance (figure 1D) delineated the defect to extend into a giant sinus of Valsalva aneurysm (SVA) measuring (8.3×7.5×10 cm). The body of the aneurysm was causing extrinsic right ventricular outflow tract compression resulting in symptoms. Coronary angiography failed to identify the right coronary artery. The coronary catheter repeatedly entered the body of the aneurysm via a large defect in the right aortic sinus of Valsalva. Contrast injection demonstrated a smooth-walled aneurysmogram (figure 1E and see online supplementary data videos S2 and S3). Surgical reconstruction was performed by direct defect patch closure and bioprosthetic aortic valve replacement. The patient had an uncomplicated recovery from surgery and remains well at 2-year follow-up.
{kind=link}
(A) Parasternal long-axis echo view. A defect (*) can be identified in the aortic root extending into the sinus of Valsalva aneurysm (SVA). Right ventricular outflow tract (RVOT) compression by SVA detected by cardiac CT (B) with three-dimensional CT reconstruction (C). Cardiac MRI image of SVA (D). Left anterior oblique fluoroscopic view of SVA (E) outlined by contrast injection from coronary catheter within the SVA.
Giant SVAs are extremely rare. They usually have a congenital aetiology and are associated with Ehlers–Danlos syndrome. Aneurysms typically involve the right coronary sinus. Complications include: pericardial rupture, fistulation into the right atrium (Gerbode defect) or right ventricle and direct cardiac compression. Symptoms may be insidious in nature or present acutely. Multimodality imaging presented in this case provided extensive functional and anatomical data to plan successful surgical reconstruction of one of the largest SVAs ever reported.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
- Data supplement 2 - Online video
- Data supplement 3 - Online video
Footnotes
-
Contributors ZZ and SK wrote the article (design, planning and writing). ZZ is acting as overall guarantor. CL was involved in design, image acquisition and patient management.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.