Article Text

Statistics from Altmetric.com
A 51-year-old gentleman with tetralogy of Fallot underwent pulmonary valve replacement and tricuspid valve annuloplasty necessitating endocardial pacing system extraction so that the annuloplasty ring could be sited. During the same operation, an epicardial pacing system was implanted with the generator positioned subcutaneously in an epigastric position.
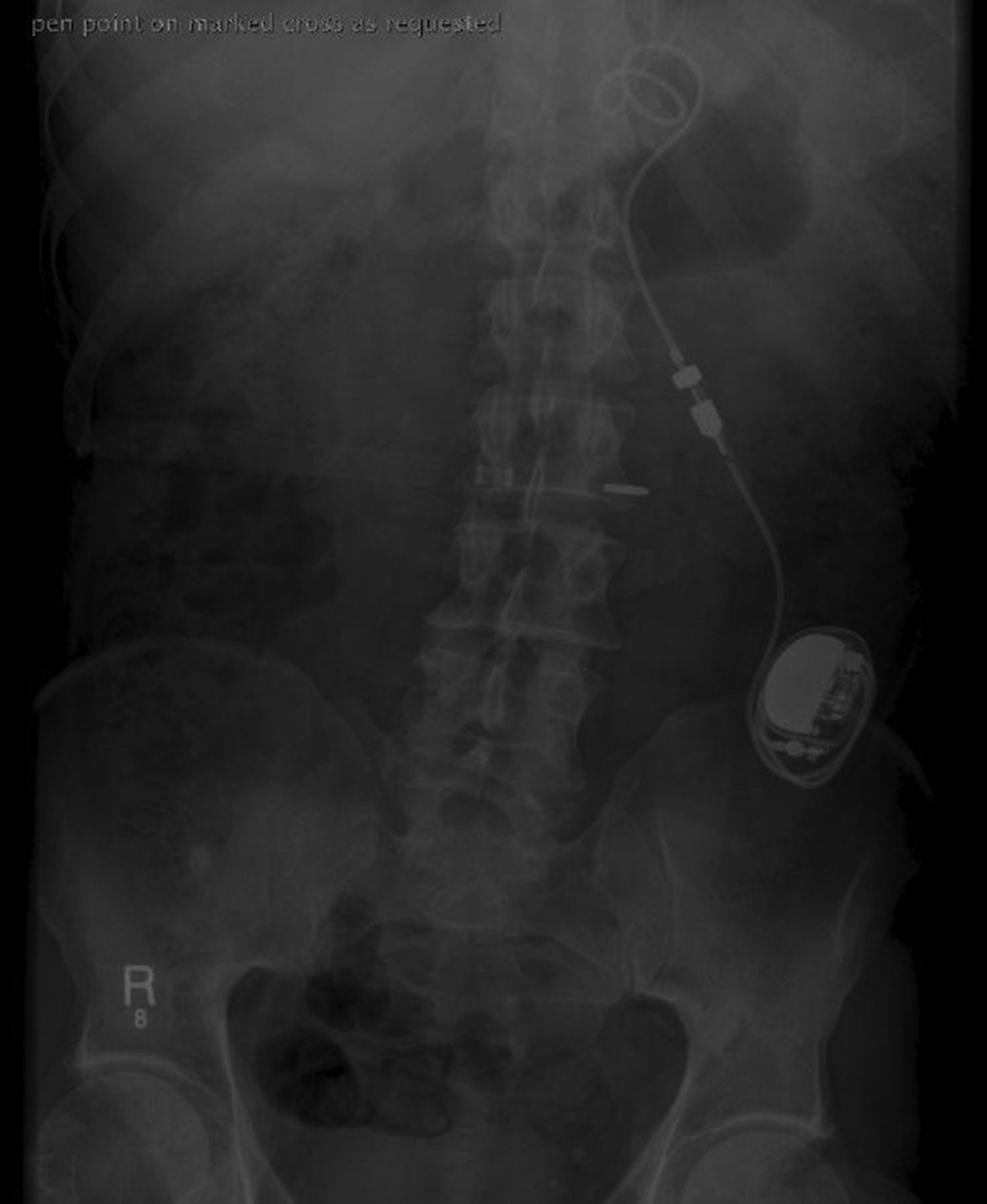
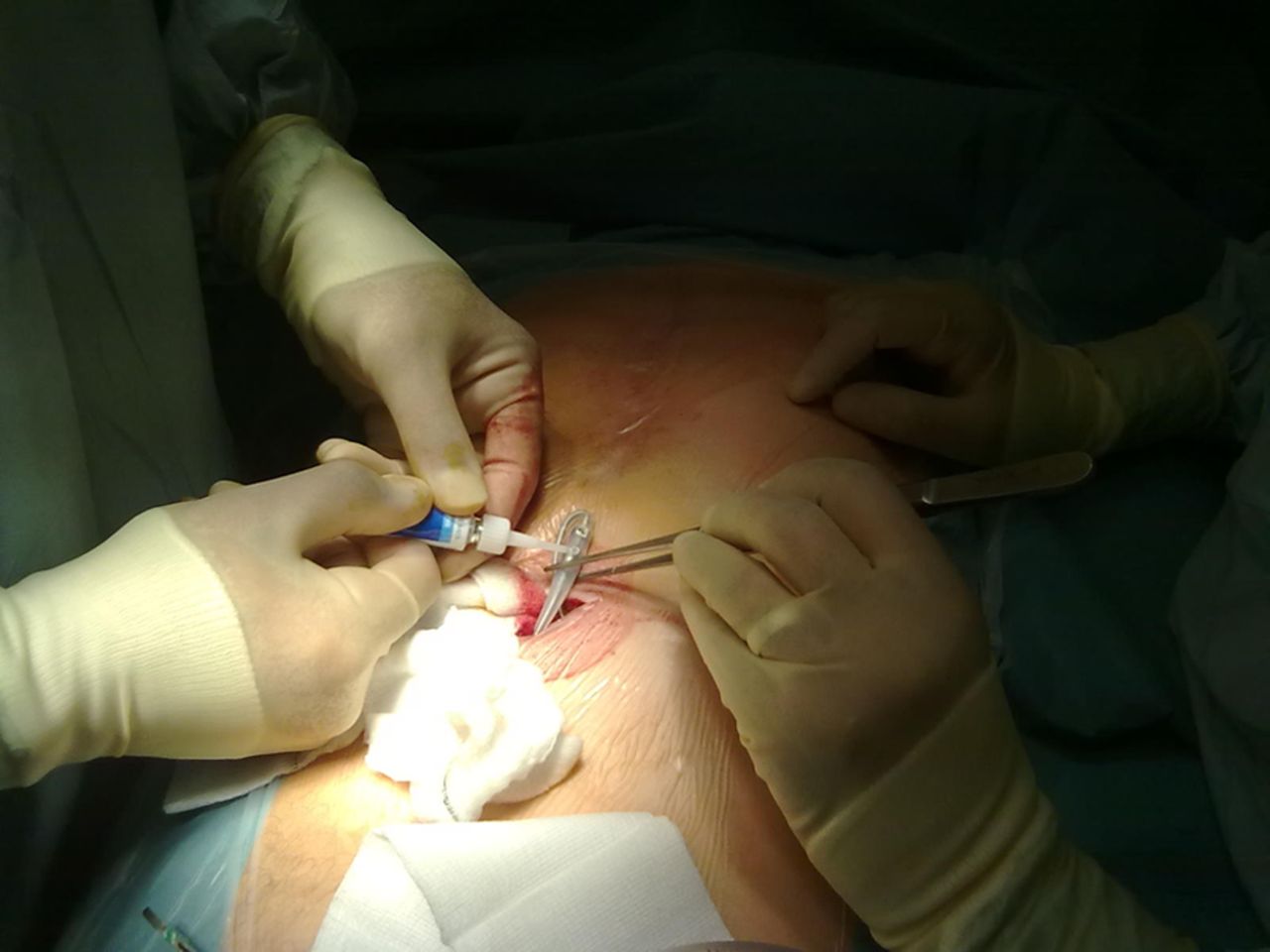
Six months later, the box was moved to the left iliac fossa because of pocket pain and a Medtronic extension connector box was used to extend the lead so that it could be implanted in a subrectus position. Several months later, the patient presented with intermittent skeletal muscle twitching in the abdomen. Lead impedance had fallen from 746 to 562 Ohms suggestive of a current leak. A radio-opaque marker was placed over the site of maximal twitching on abdominal x-ray (figure 1) which appeared to overly a lead fracture and so the patient was admitted electively for surgical exploration. During the operation, no fracture could be identified but rather the large screws used to secure the existing lead to the connector box were exposed resulting in a current leak. Figure 2 shows the surgeon placing medical adhesive over one of the screws. Due to the infrequent use of this equipment, the insulating glue was overlooked at the time of initial implantation. This case illustrates the need for a full understanding of all pacing hardware not in routine use prior to the start of a case and the importance of close collaboration between surgeons and pacing specialists when the need arises.

A radio-opaque marker was placed over the site of maximal abdominal twitching and appeared to overly a lead fracture.

{kind=link}
{kind=link}
Surgeons place medical insulating glue over the bare screws which caused the current leak.
Footnotes
-
Contributors All authors contributed to the writing up of the case and management of this patient.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.