Article Text

Statistics from Altmetric.com
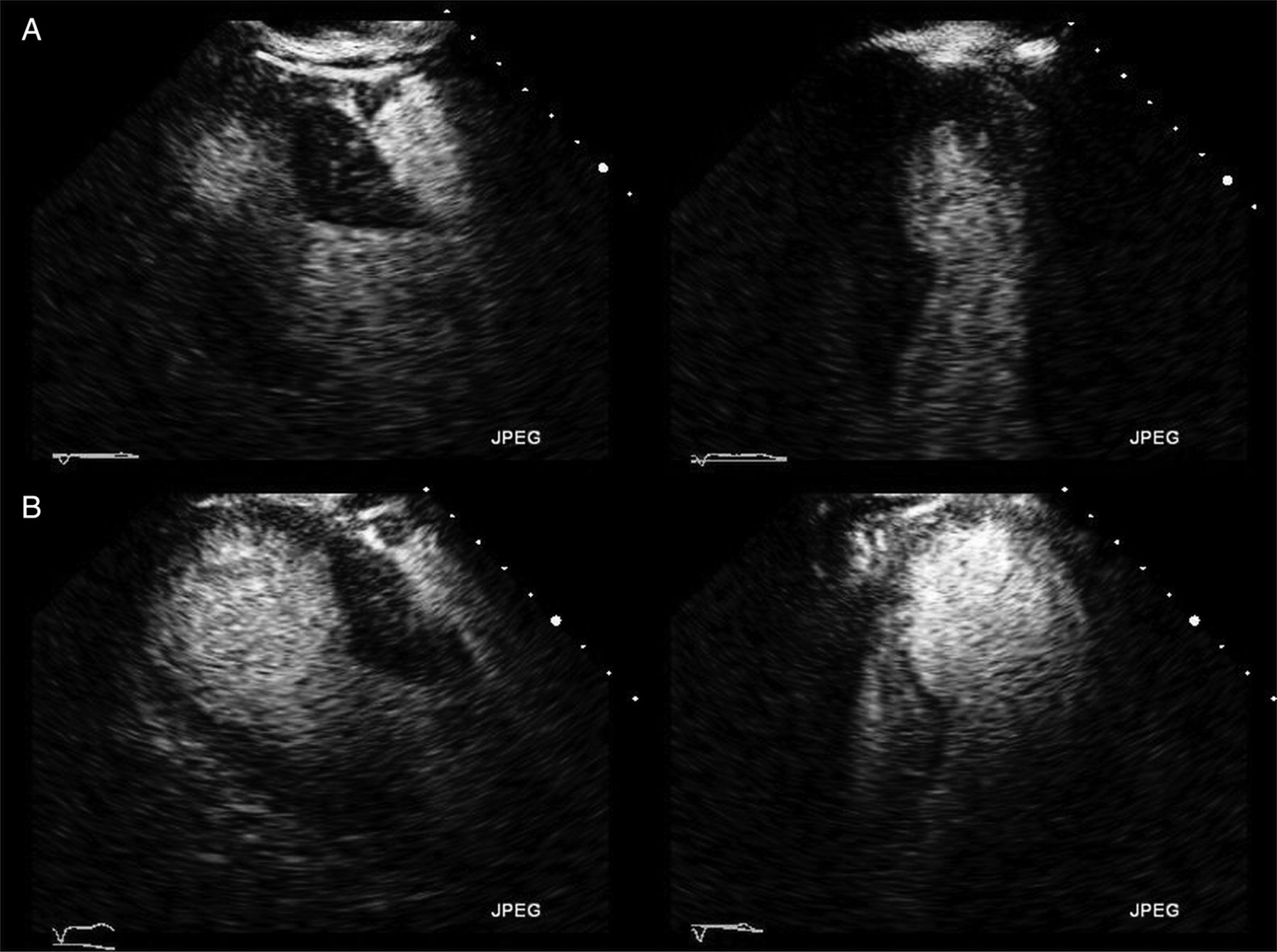
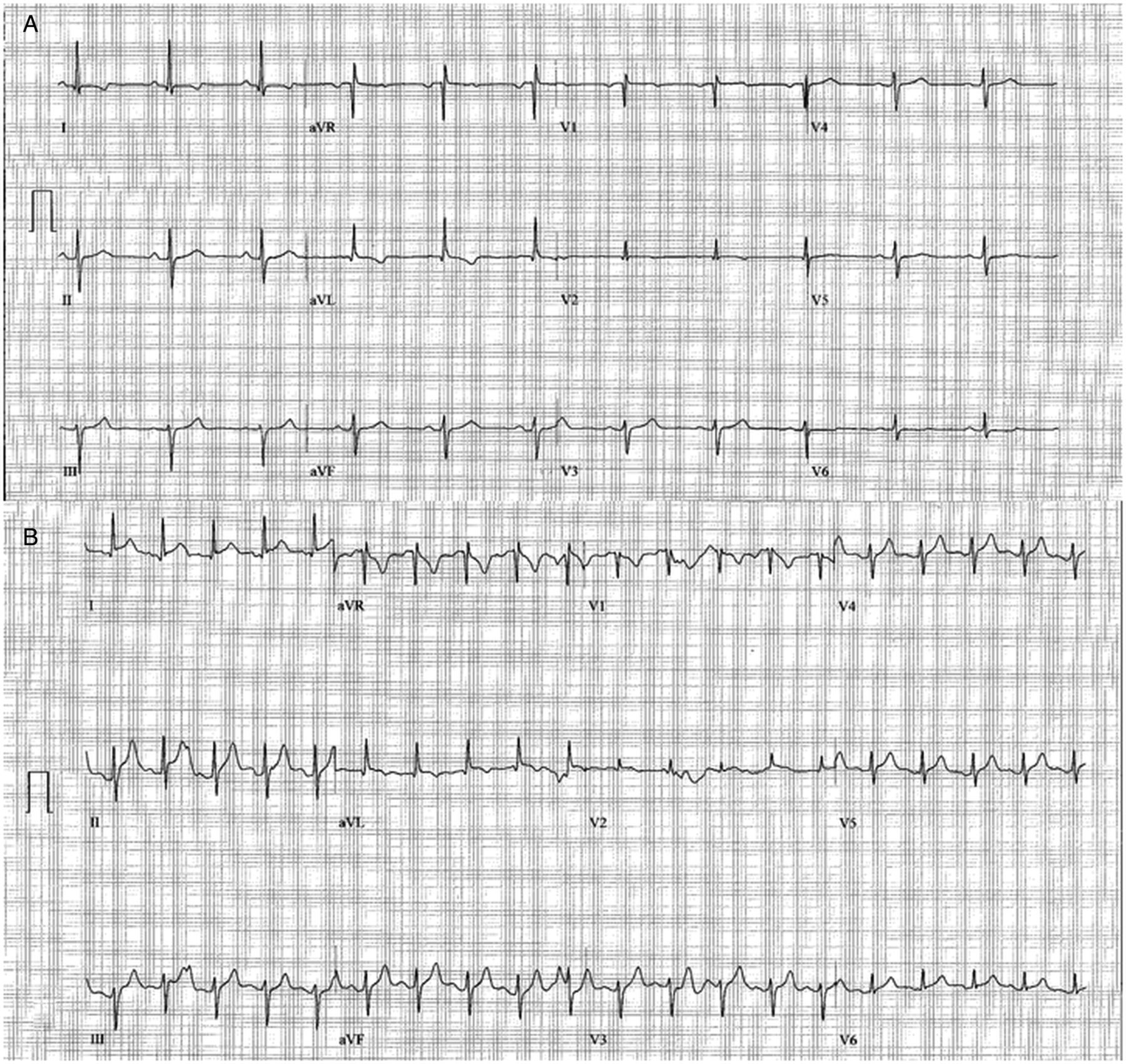
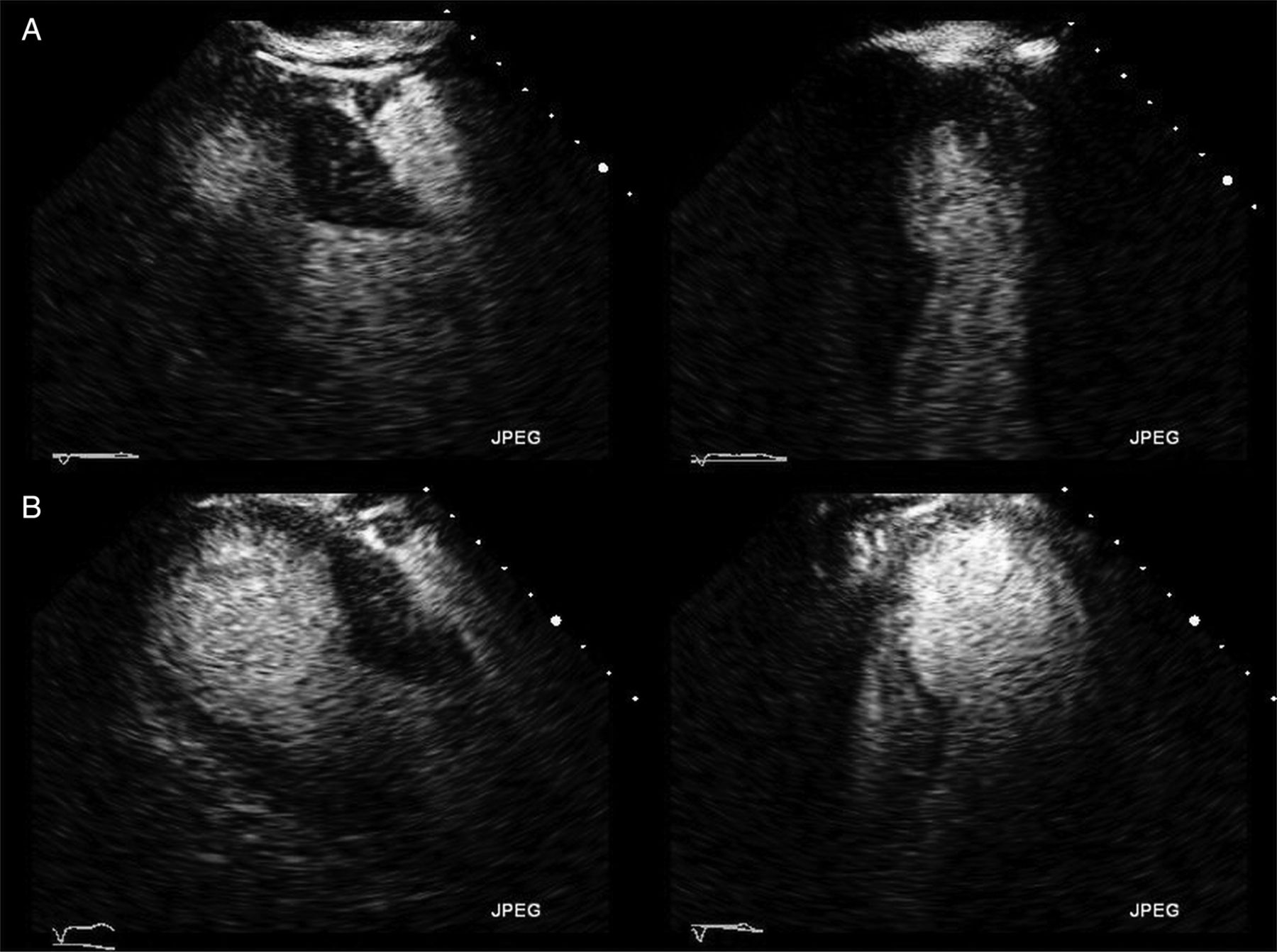
A 52-year-old man with a history of hypertension, insulin-dependent diabetes mellitus and hyperlipidaemia was referred for a dobutamine stress echocardiogram as part of a pre-renal transplant evaluation. The baseline echocardiogram showed normal systolic function with no wall-motion abnormalities (see videos 1 and 2). At peak dobutamine infusion, he developed severe abdominal pain associated with deep T-wave inversions in leads aVR and V1 and 0.5 mm ST-segment elevations in leads I and aVL (figure 1). The echocardiogram revealed akinesis of the left ventricular apex with apical ballooning (figure 2; videos 3 and 4).
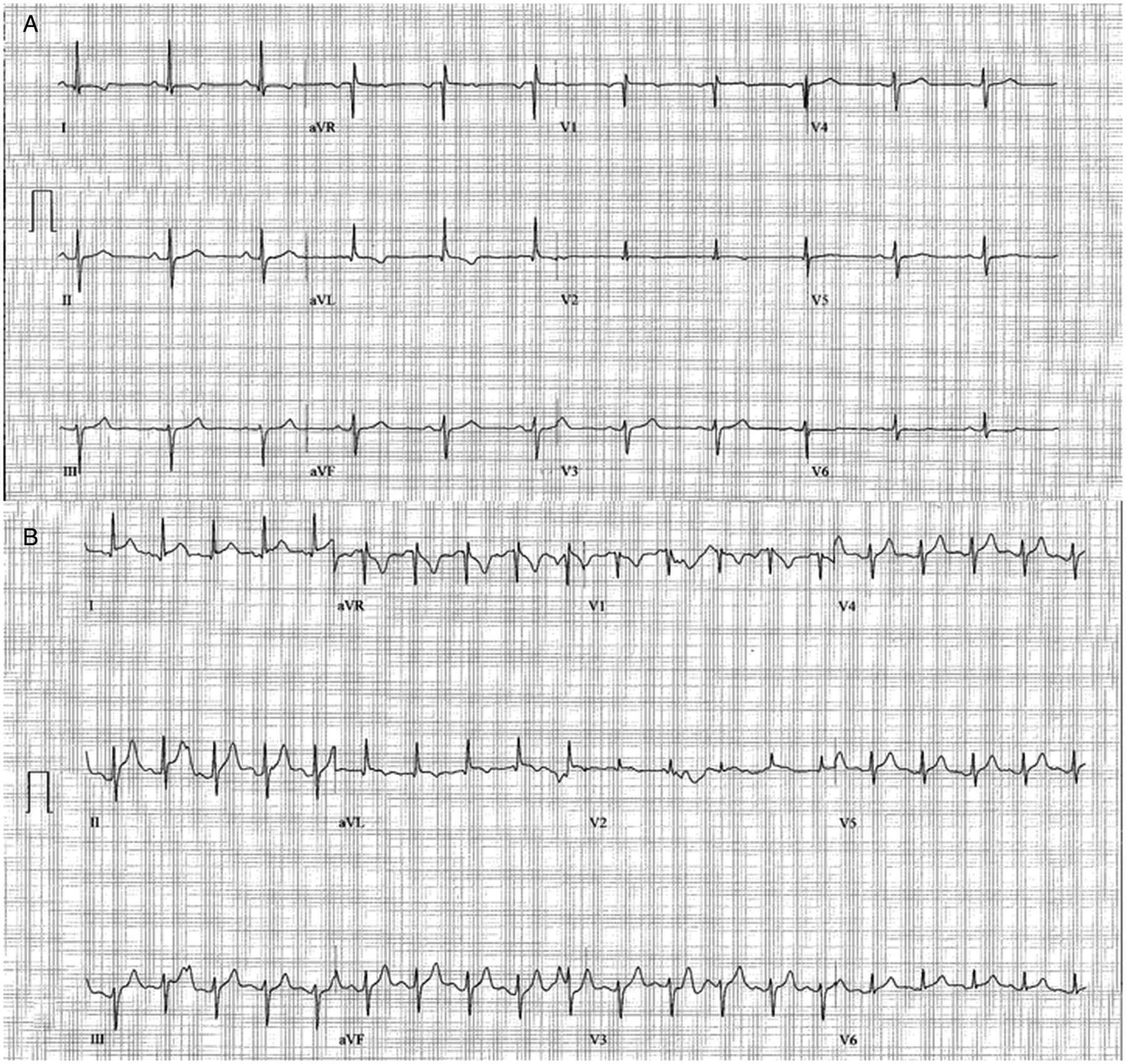
Baseline EKG (A). Immediate post-infusion EKG (B) showing 0.5–1 mm ST-segment elevations in leads I and aVL.
{kind=link}
{kind=link}
Standard parasternal long axis and apical four chamber views obtained during a dobutamine stress echocardiogram. Baseline images (A) show normal left ventricular systolic function. At peak dobutamine infusion (B), there is mid and apical wall akinesis with sparing of the basal segments.
An emergent cardiac catheterisation showed single-vessel coronary artery disease in a small first diagonal branch of the left anterior descending, but there was no evidence of thrombosis or plaque rupture in a coronary distribution to explain the severe apical wall-motion abnormalities. Two weeks later, a repeat echocardiogram showed return of normal left ventricular systolic function.
Takotsubo cardiomyopathy was first described by Sato et al1 in 1990 as a condition of reversible left ventricular dysfunction and apical ballooning that mimics an acute myocardial infarction but it occurs in the absence of obstructive coronary artery disease. Several mechanisms have been proposed, including coronary vasospasm, microvascular dysfunction and catecholamine toxicity; however, the exact aetiology is not fully understood.2 This report of dobutamine-induced transient apical ballooning supports the hypothesis of catecholamine-induced cardiotoxicity as a significant contributor to the pathophysiology of Takotsubo cardiomyopathy. All clinicians should be aware of the potential of dobutamine stress testing to induce transient apical ballooning.
References
Footnotes
-
Contributors All authors contributed to the preparation and submission of this manuscript and approved the final draft of this manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.