Article Text

Abstract
Background The numerical values and ranges of the ECG are used as criteria for classifying types of arrhythmia. However, one criterion cannot be generically applied for all patient groups. Several studies have shown that age, gender, and race are the major key factors which produce variations in ECG values.
Methods From May 2013 to February 2014, we collected 12 993 normal ECG data from 9853 Northern Thai patients at Maharaj Nakorn Chiang Mai Hospital, Chiang Mai, Thailand, to analyse their ECG reference ranges.
Results The results showed that the average heart rate decreased, while the PR interval and QTcB increased with increasing age in both genders. The normal range of heart rate was lower than the standard interval. QRS duration was stable in all age groups but longer in males than females. QRS axis deviated to the left with increasing age. SV1+RV5 amplitude slightly changed in both genders, but the upper limit crossed over the criteria of ventricular hypertrophy.
Conclusions We observed that the general trend of data was mainly similar to that found in other studies in Chinese, American, and African populations. However, some minor differences should be considered specifically for the Northern Thai population. Flexible criteria on conditions depending on age and gender should be adjusted for Northern Thai patients according to the results of this research.
Statistics from Altmetric.com
Introduction
For many decades the ECG has been well established as a useful tool for diagnosing cardiac diseases. Cardiologists use ranges of ECG numerical values as criteria to classify the different types of arrhythmias. For example, heart rates which are lower than 50 beats/min (bpm) or higher than 100 bpm are classified as bradycardia and tachycardia, respectively (normal range 60–100 bpm).1 PR interval exceeding 200 ms indicates first degree atrioventricular (AV) block (normal range 120–200 ms).1 QRS duration which is wider than the traditional upper limit of 120 ms is considered to be a bundle branch block. The normal range of heart rate-corrected QT interval, obtained by using Bazett's formula (QTcB), recommends that QTcB is generally accepted to be ≤440 ms and the upper limit should be set at 450 or 460 ms.1 Hypokalaemia results in a prolonged QT which may indicate an increased risk for developing ventricular fibrillation. Left or right QRS axis deviation (normal value −30° to +90°1) and high SV1+RV5 amplitude (Sokolow Lyon index (SL index), normal value <3.5 mV1) help clinicians to detect ventricular hypertrophy.
However, global diagnostic criteria cannot be applied generically for all patients. Several studies have reported that race, gender, and age are major factors affecting normal limits of ECG references.2–10 The study of normal limits derived from 5360 Chinese people by Wu et al2 proposed that the normal range of heart rate should be adjusted from 60–100 bpm to 50–95 bpm for ethnic Chinese. The Chinese study showed that the average heart rate in women was higher than in men, but heart rate decreased with increasing age only for women. The PR interval gradually increased with age but the upper limit was still under 200 ms in all age groups. QRS duration was quite constant in both genders but the upper limit for women should be lowered to 109 ms. The upper limit of QTcB tended to increase with age and it was always above the standard cut point. The QRS axis shifted to the left with increasing age. The SL index in men was higher than for women in all age groups and the threshold in men should be renewed to 4.2 mV.
Mason et al4 also proposed that ECG reference ranges should be modernised in regard to the large influence of age and gender factors. They suggested the new recommended normal range of heart rate was between 48–98 bpm, PR interval was between 113–212 ms, QRS duration was between 69–109 ms, QRS axis was between −40° to 91°, and QTcB was between 361–457 ms. Similar to the Wu report, the range of heart rate was 48–98 bpm and it decreased with increasing age in both men and women. The PR interval increased with age whereas QRS duration was stable in all age groups. QTcB interval increased with age only in women and QRS axes shifted to the left with increasing age.
As mentioned above, several studies have already documented the effect of gender, age, and race on the ECG values in different groups of the population. However, a study of Thai subjects (South East Asia inhabitants) has never been reported.
This research aims to present the ECG references of Northern Thai people, derived from ambulatory patients at Maharaj Nakorn Chiang Mai Hospital, the largest hospital in northern Thailand, and compare the ethnic differences of ECG intervals and axes with Chinese, Nigerian, American, and Thai subjects. This information can also provide more accurate reference ranges for Northern Thai patients, thus leading to better diagnosis and treatment.
Subjects and methods
Selection of subjects
The ECGs were recorded in a supine position with ambulatory patients by three well-trained nurses at the Outpatient Department (OPD) ECG room, Maharaj Nakorn Chiang Mai Hospital. From May 2013 to February 2014, 12 993 standard 12-lead ECGs from 9853 patients were included in the study. All ECG data were blindly retrieved by system software and made anonymous by using numeric identification. Only 11 091 ECGs with interpretations of ‘sinus rhythm’ and ‘normal sinus rhythm’ were included in the analysis. The study population was divided into gender and age groups. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee.
The ECG records from the OPD ECG room included a wide range of patient characteristics. Most patients in this room were ambulatory. Unstable patients had their ECGs recorded at an emergency room or internal wards for reasons of patient safety. ECGs for specific diagnoses were recorded at the Cardiology Center. The medical records showed that the majority of ECGs were used for general assessment such as assessing target organ damage in chronic diseases, follow-up examination after treatment, and general medical check-up. Among the total population, 17% were patients with cardiovascular diseases. Within this cardiovascular group, patients with primary hypertension and heart diseases were the most common diseases (44.08% and 19.16% of the cardiovascular group or 7.52% and 3.72% of the total sample, respectively). Screening tests such as follow-up examination after surgery and general medical screening were the second largest group (11.46%).
ECG and data management system
The signal was processed using three different types of ECG; CardiofaxM, Philips PageWriter, and GE MAC 800. There was no report that showed statistically or clinically significant differences in ECG parameters between these three cardiographs. Each cardiograph contains individual software to convert electrical raw signals to binary data. The data were analysed by applying a mathematic algorithm to measure ECG wave amplitudes and intervals. All digital parameters and ECG signal values were transmitted via a local area network (LAN) cable from the cardiograph to a personal computer (PC) within the transmission control protocol/internet protocol (TCP/IP). The data were stored as an extensible markup language (XML) file in a local directory in a PC. The ECG was displayed on a screen using a local ECG management system11 and the quality of the signal was verified by the nurse before data were submitted into the hospital database.
ECG parameters
Measurements of amplitudes and durations were computed by software in the cardiograph in accordance with standard recommendations. Six parameters—heart rate, PR interval, QRS duration, QTcB, QRS axis, and SV1+RV5 amplitudes—were included for observation in this study.
Statistical analysis
The 2nd and 98th centiles of the distributions on each parameter were taken to represent the lower and upper normal limits, respectively. Mean was calculated as an arithmetic average of a set of values and median was calculated as the middle number of the data.
Results
Characteristics of the study population
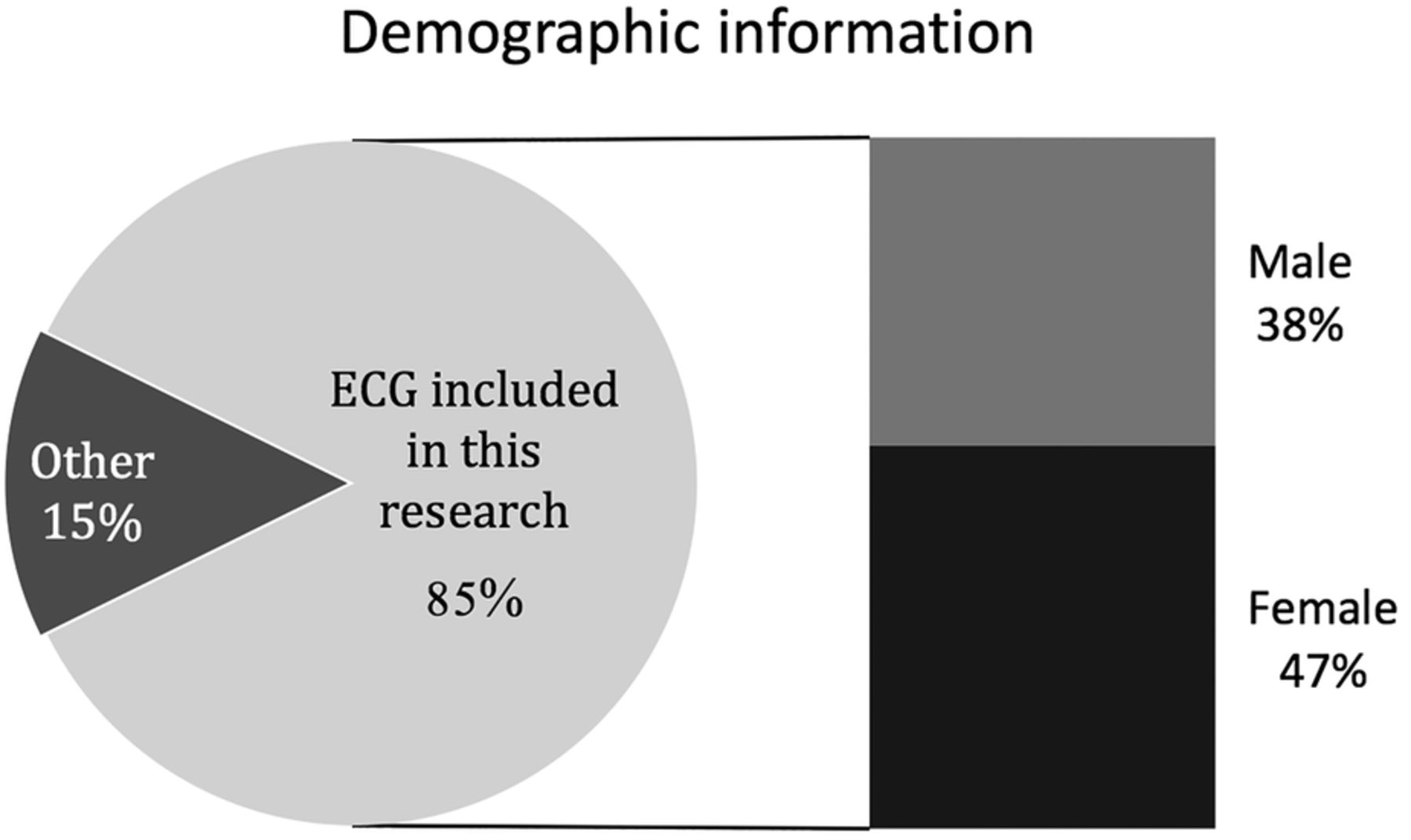
Table 1 and figure 1 show the demographic information for the study population. Eighty-five per cent of total ECGs were included in the analysis. Fifteen per cent were excluded from this study because of abnormal ECG findings. Around 45% of selected subjects were men. The average age in the selected group was 55.62 years and the lowest and highest ages were 4 and 98 years, respectively.
Demographic information
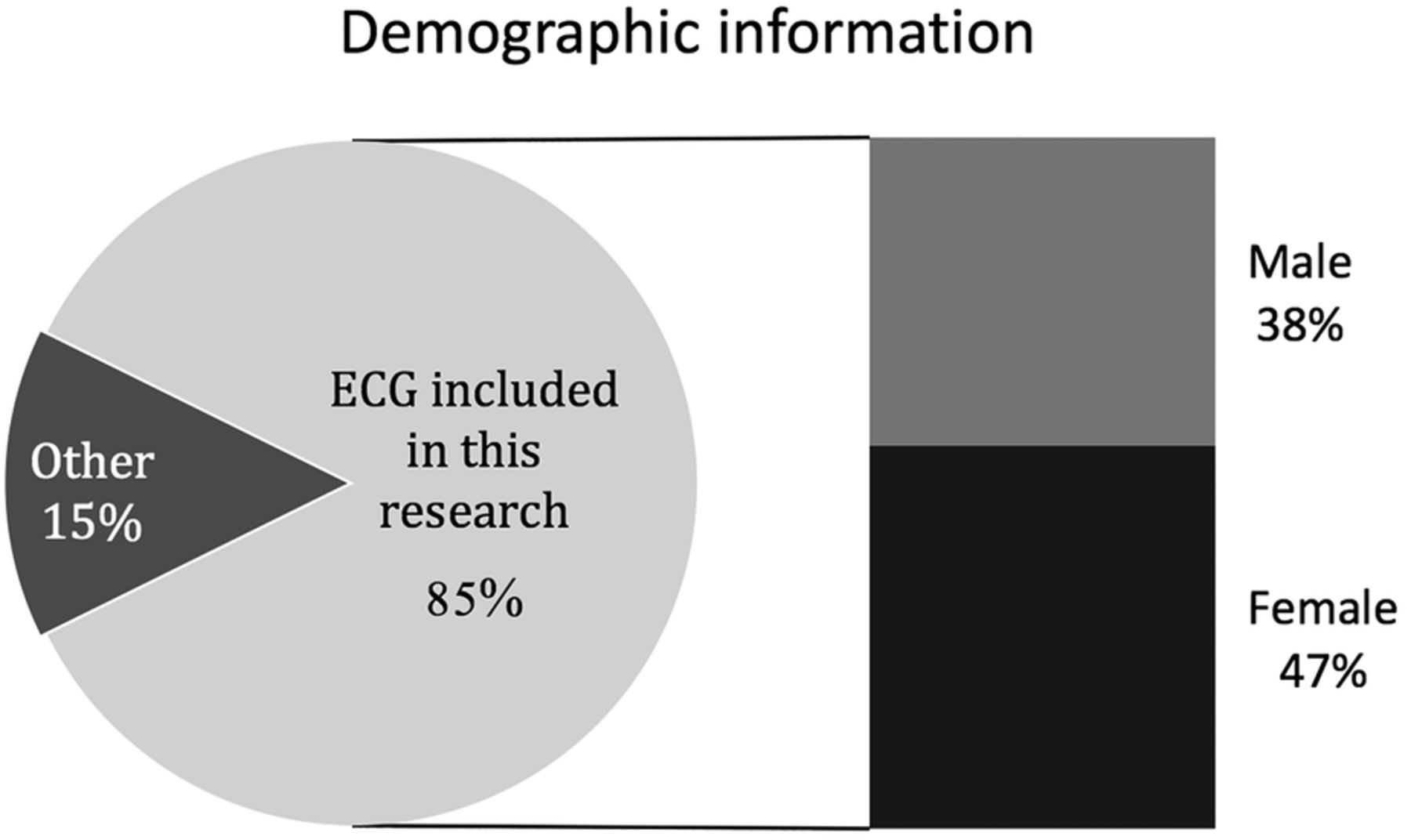
Demographic information of the study population.
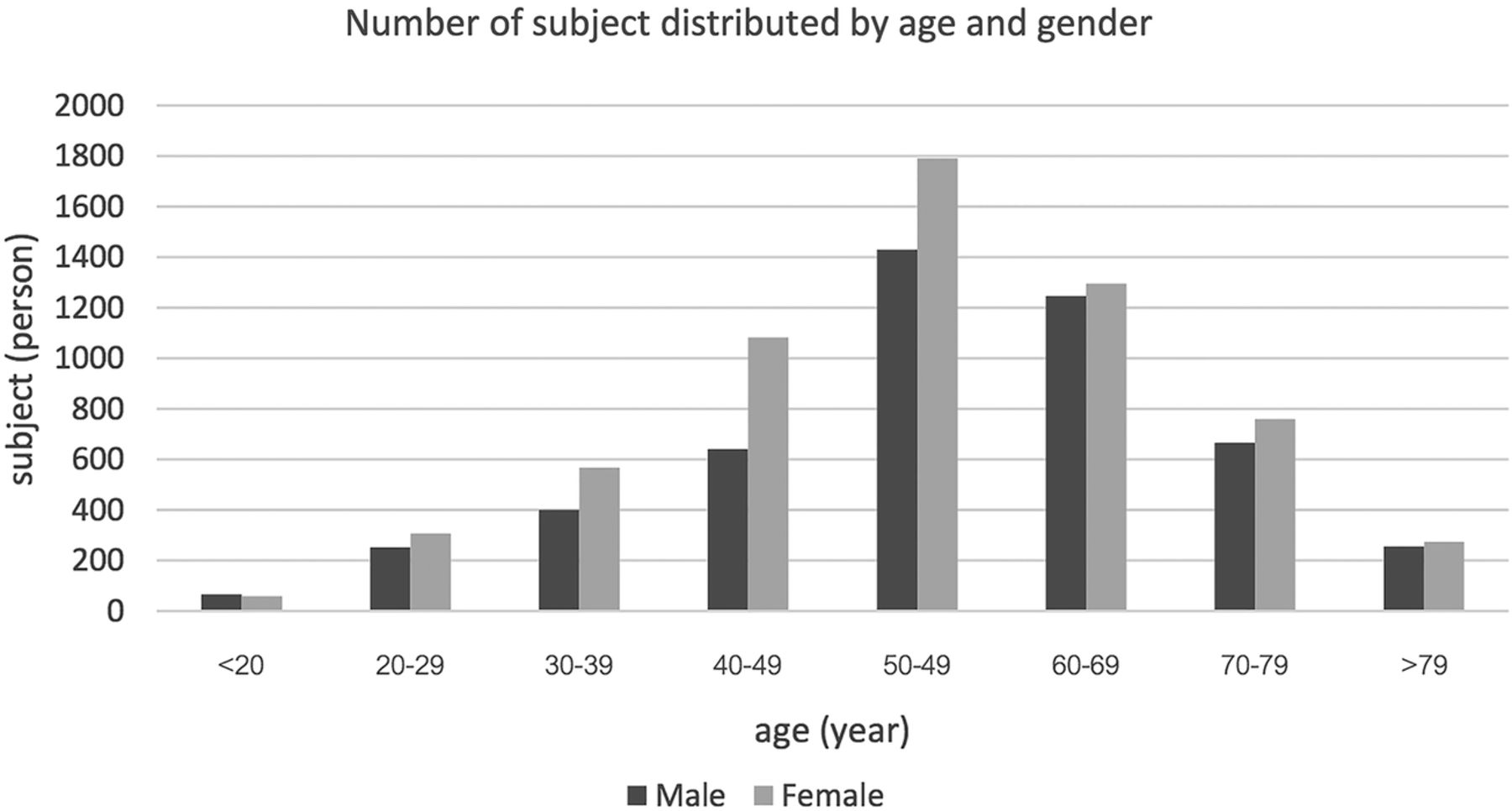
In table 2, the data show the distribution of subjects by age and gender. Subjects were divided into eight age groups: <20 years, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, and >79 years. The majority of our population was middle-aged (between 40–69 years). The age group 50–59 years had the highest percentage of subjects (29.04%). The smallest group was the <20 years range which contained only 1% of all subjects. Figure 2 illustrates a normal distribution pattern of population by age.
Number of subject distributed by age and gender
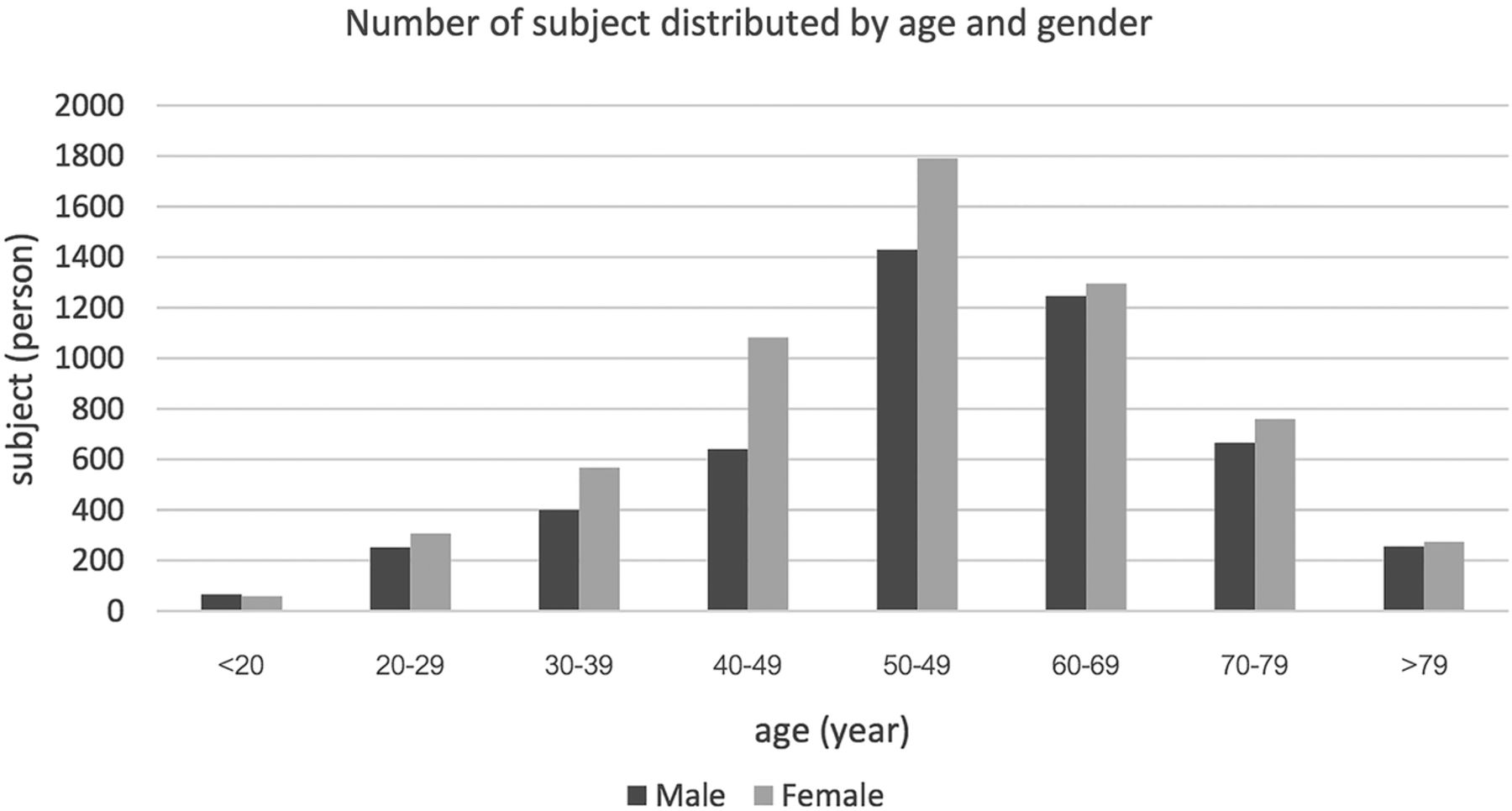
Number of subjects distributed by age and gender.
ECG findings
Tables 3⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–14 show the median, mean, SD, upper limit, and lower limit of the six key ECG parameters distributed by age groups and gender.
Heart rate
Heart rate distributed by age and gender
PR intervals
PR intervals distributed by age and gender
QRS duration
QRS duration distributed by age and gender
QTcB interval
QTcB interval distributed by age and gender
QRS axis
QRS axis distributed by age and gender
Sokolow-Lyon (SL) index (SV1+SV5)
Sokolow-Lyon (SL) index (SV1+SV5) distributed by age and gender
Age factor in ECG
All parameters showed significant age trends except QRS duration and SL index. Heart rate and QRS axis gradually decreased with increasing age whereas PR interval and QTcB interval increased.
Gender factor in ECG
Sex differences were noticeable in all six parameters: median heart rate was 3 bpm higher in females; PR interval and QRS duration were 8 ms longer in males; QTcB was 5 ms longer in females; QRS axis was 4° higher in females; and SL index was 0.36 mV higher in males.
Heart rate
The average heart rate gradually decreased with increasing age in both genders. The average heart rate in all age groups was slightly higher for females than males. The upper limit of heart rate was approximately 97 bpm in both genders. The lower limits were 53 bpm in males in all age groups whereas the lower limit decreased from 59 to 52 bpm with increasing age in females.
PR interval
The median PR interval was 164 ms in males and 156 ms in females. In both genders, PR interval increased with increasing age from 148 to 185 ms in males and from 154 to 164 ms in females. The upper limits of PR interval were 238 ms in males and 216 ms in females.
QRS duration
The median QRS duration was 94 ms in males with a range of 76–142 ms and 86 ms in females with a range of 70–132 ms, with no age trend.
QTcB interval
The median QTcB increased with increasing age, from 432 to 443 ms in females and from 427 to 439 ms in males. The upper limit of QTcB in both genders was close to 500 ms.
QRS axis
The median QRS axis was 45° in females and 41° in males. The data showed a progressive deviation to the left in both genders. The QRS axis deviated from 78° to 31° in males and from 75° to 29° in females with increasing age.
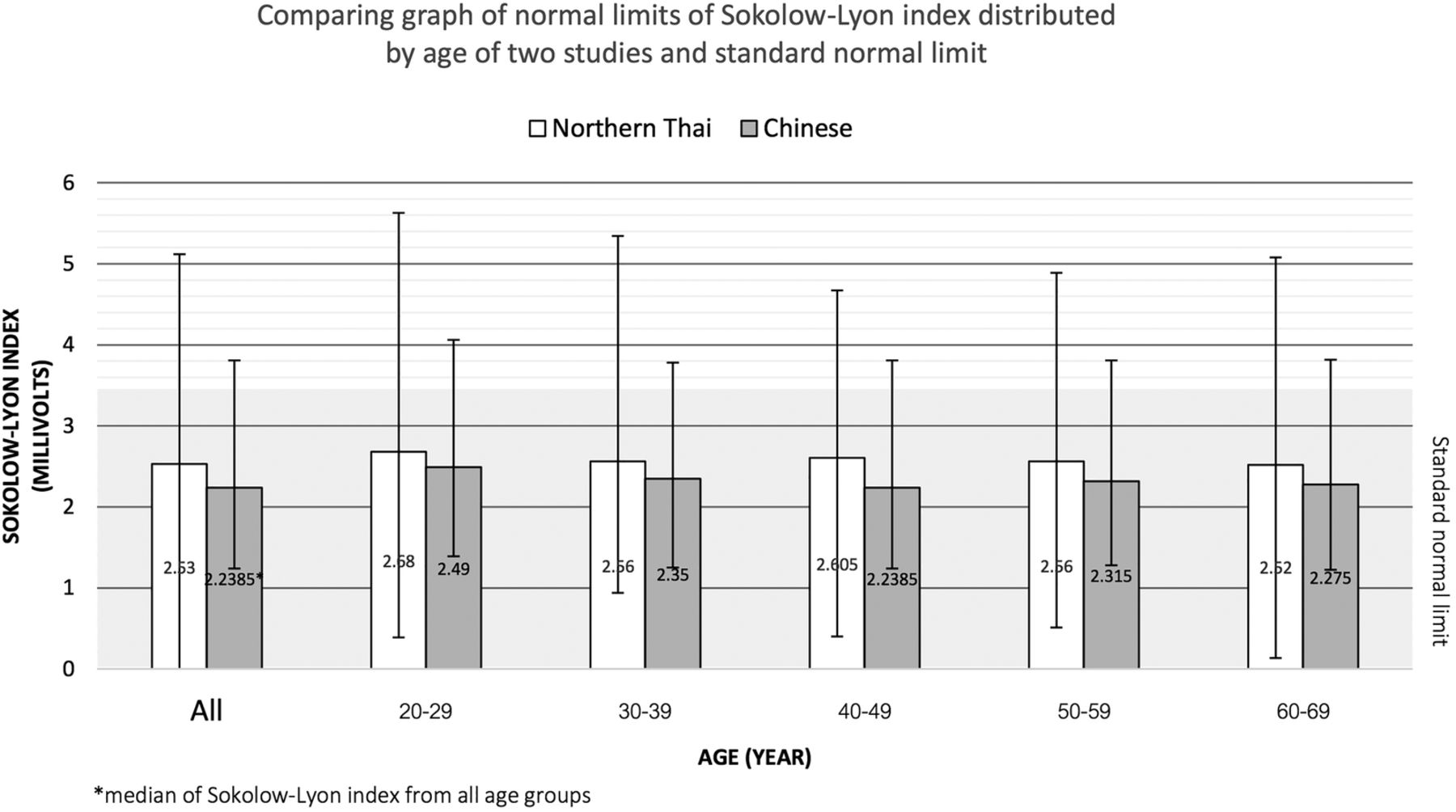
SL index
The median SV1+RV5 amplitude was 2.73 mV in males and 2.37 mV in females. SV1+RV5 amplitude did not show a significant trend with increasing age in both genders. However, the general trend in males gradually decreased over time whereas it increased in females. The upper limit of SL index was between 4.97–6.19 mV in males and between 4.29–5.45 mV in females.
Discussion
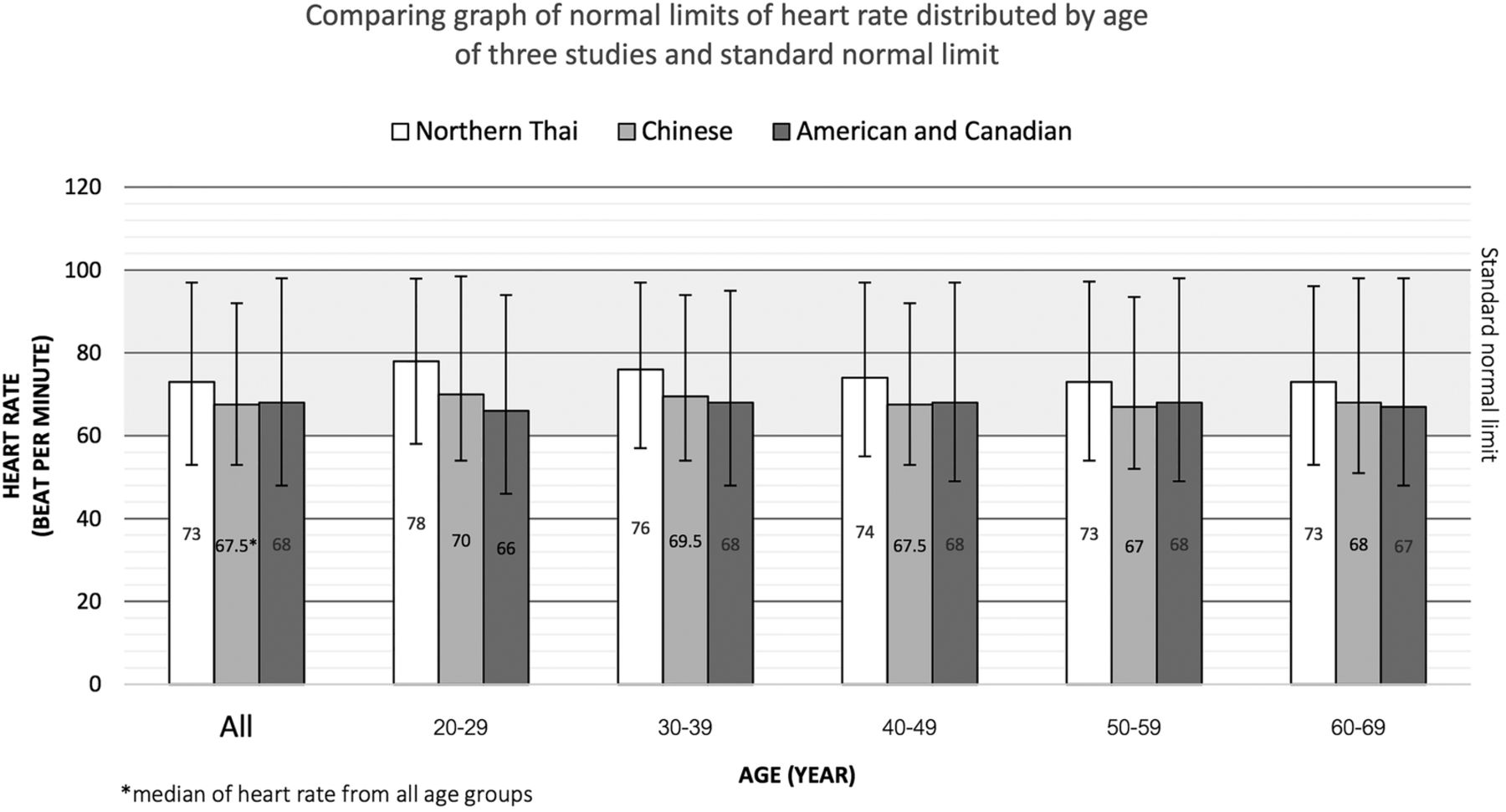
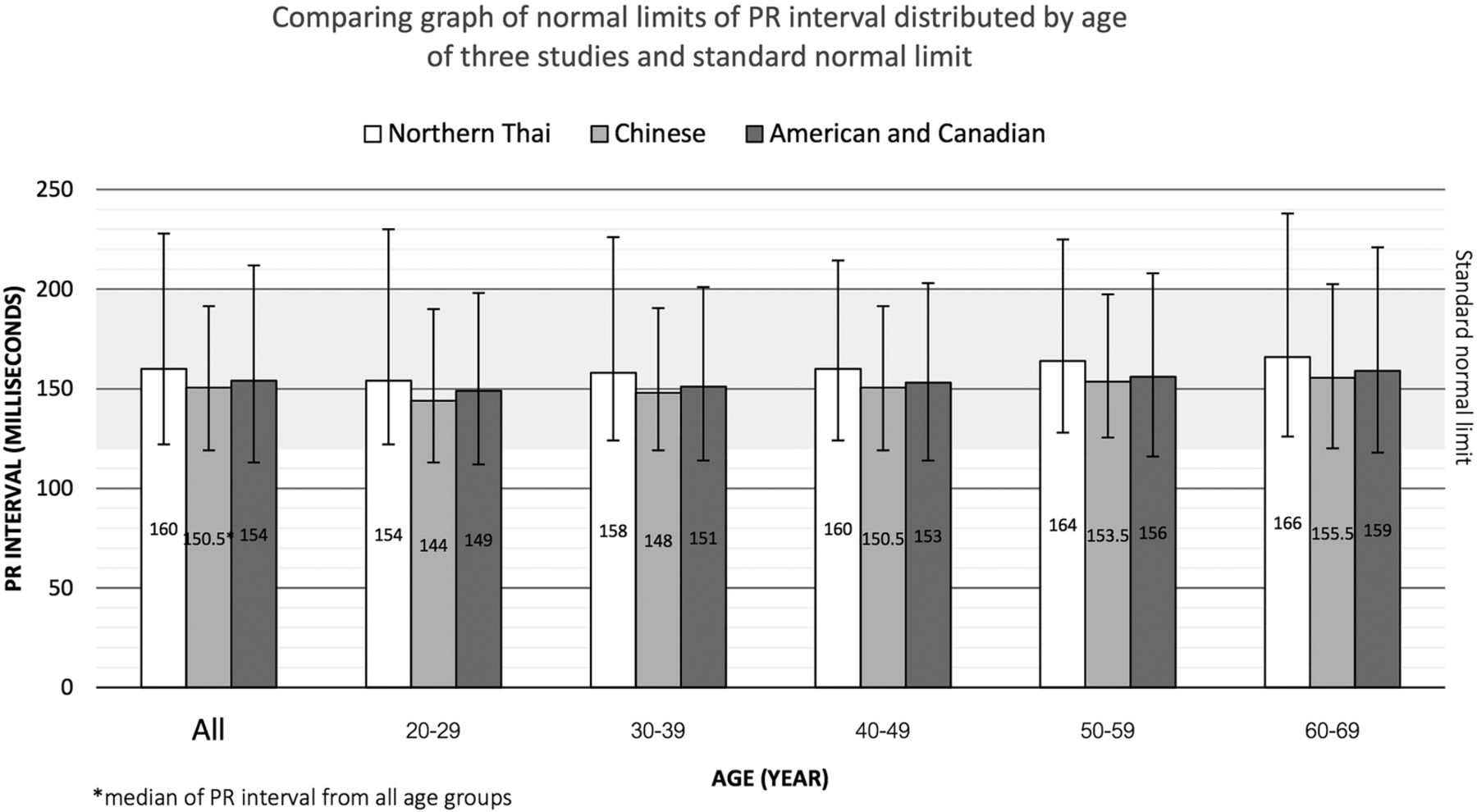
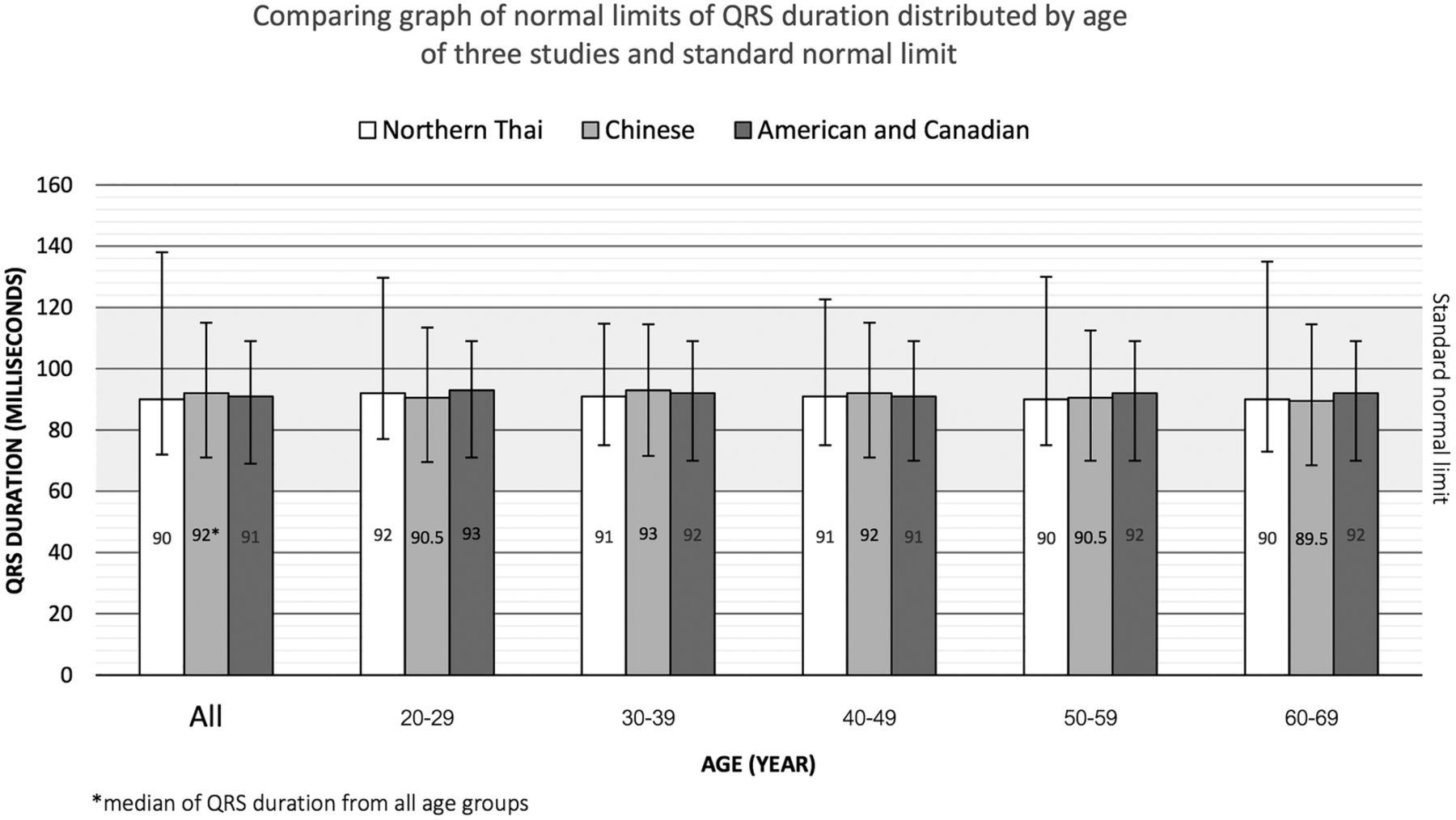
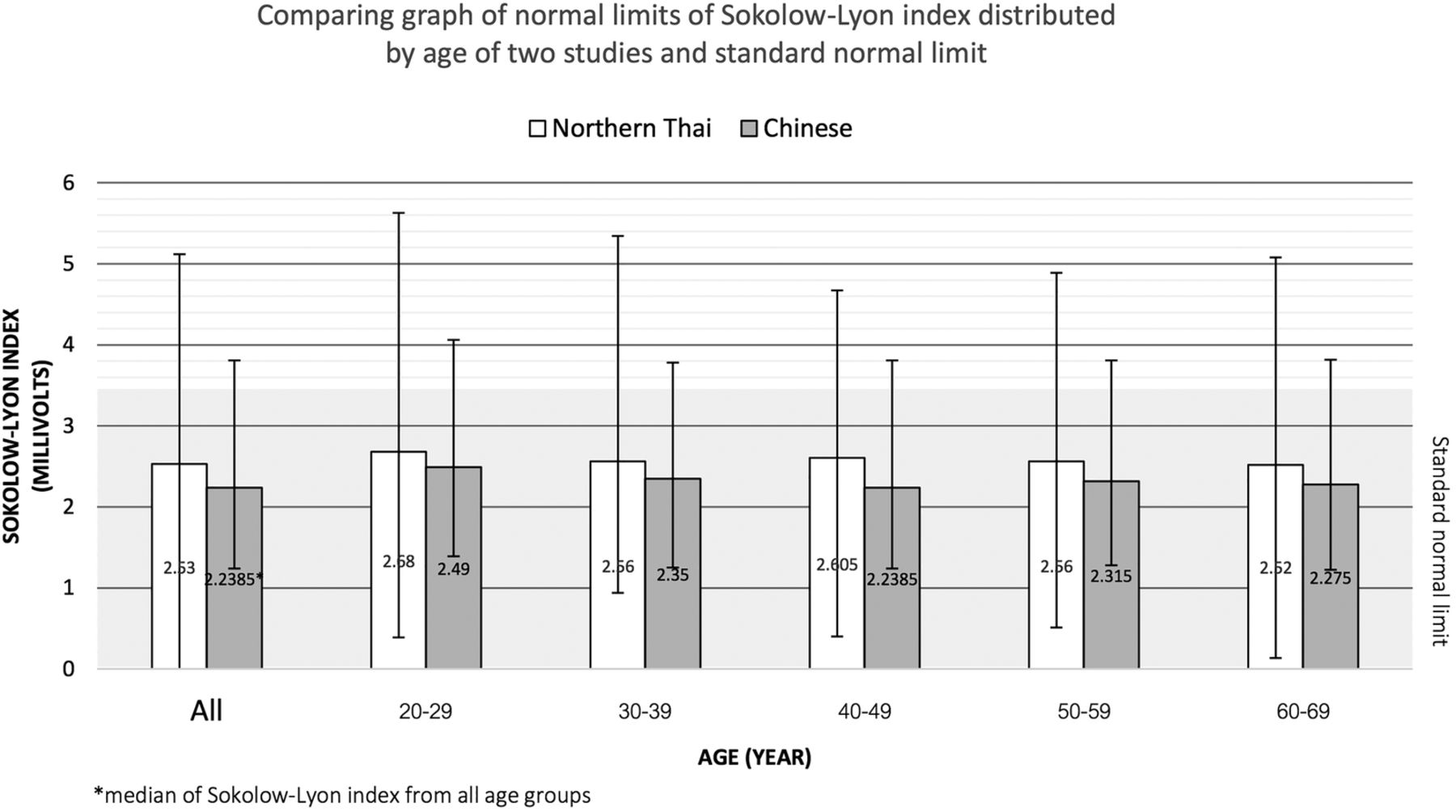
We discuss the results of this study by considering the three factors of age, gender, and race. We selected three studies to compare their findings with our data. Each study represents a population from a different continent: the study reported by Wu et al2 represents the ECG values for a Chinese population; the study reported by Mason et al4 represents the ECG values for a Western (Northern American—US and Canadian) population; while the study reported by Katibi et al3 represents the ECG values for a Nigerian population. This study provides the comparative ECG values for the Northern Thai population. Figures 3⇓⇓⇓–7 illustrate the comparison of heart rate, PR interval, QRS axis, QRS duration, and SL index, respectively, by median with 98% upper and 2% lower limit in Northern Thai, Chinese, and American populations.
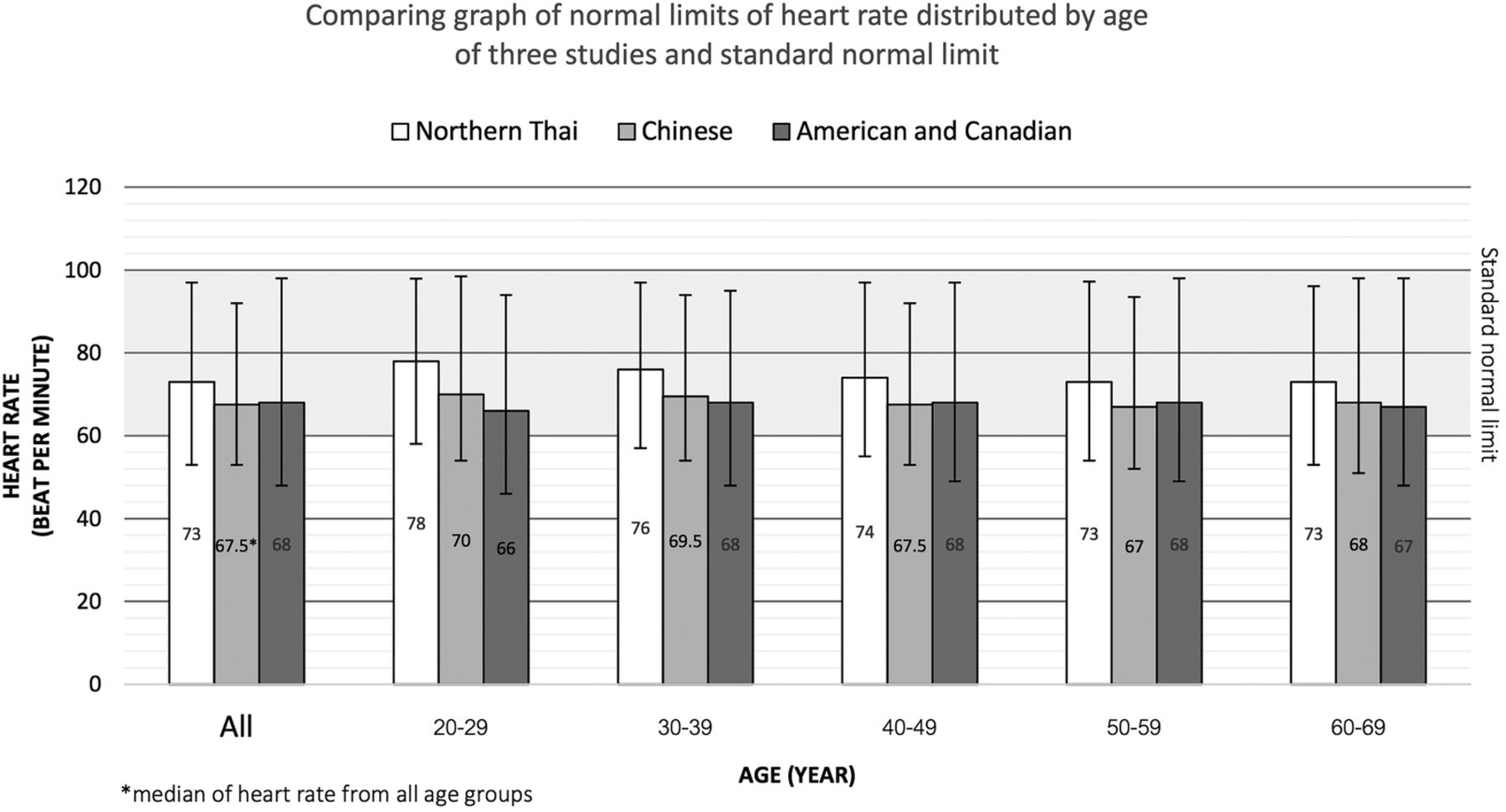
Normal limits of heart rate distributed by age.
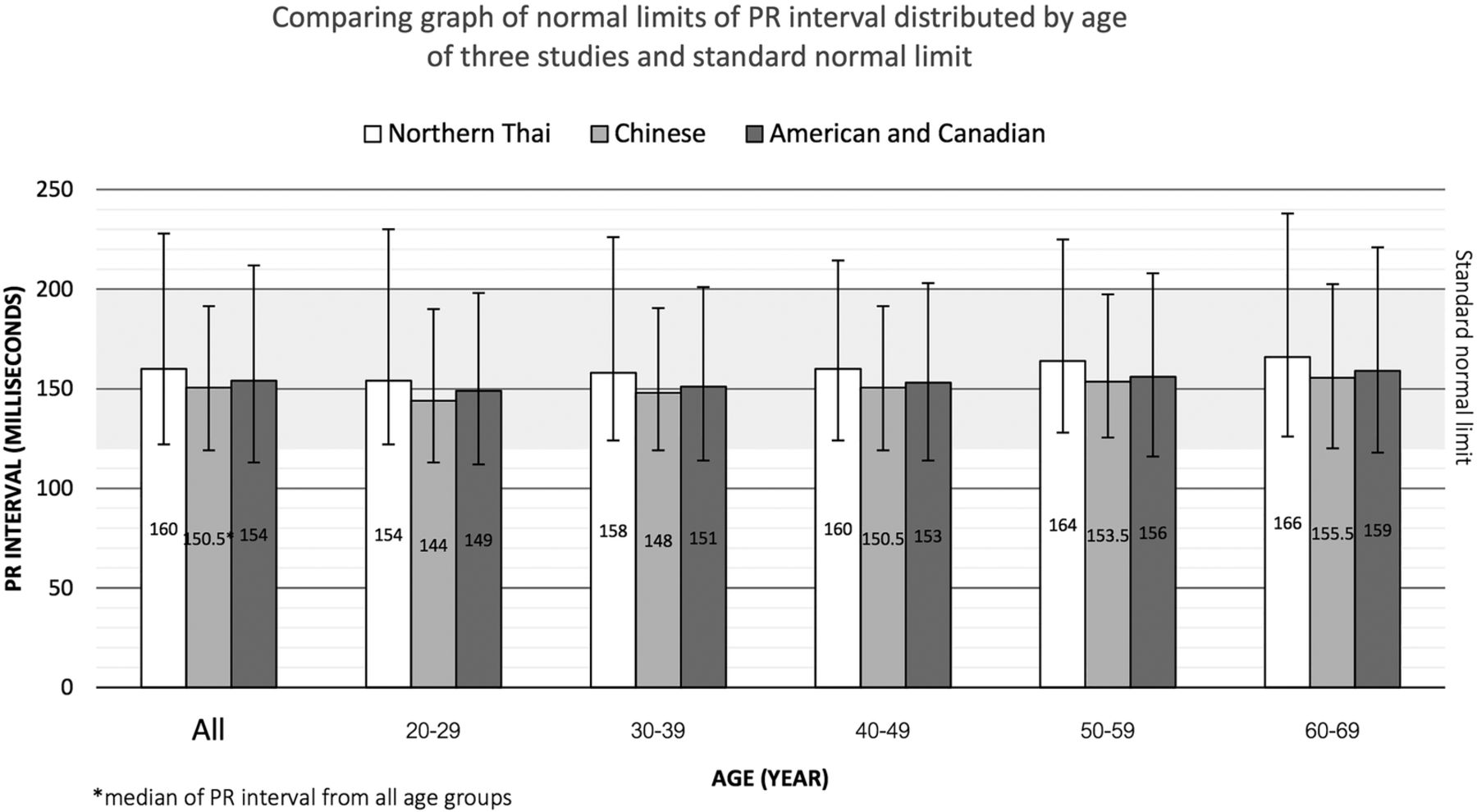
Normal limits of PR interval distributed by age.
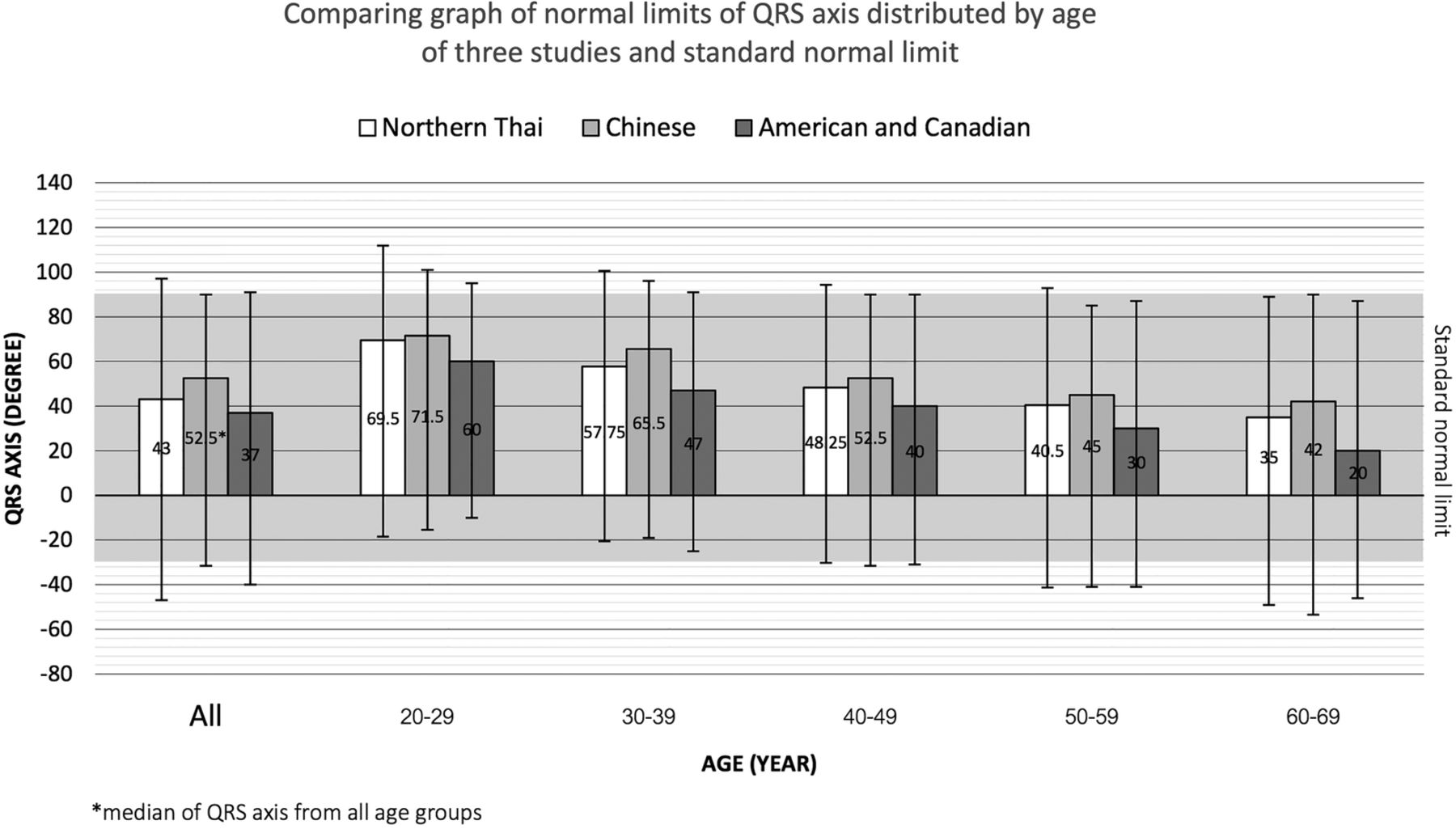
Normal limits of QRS axis distributed by age.
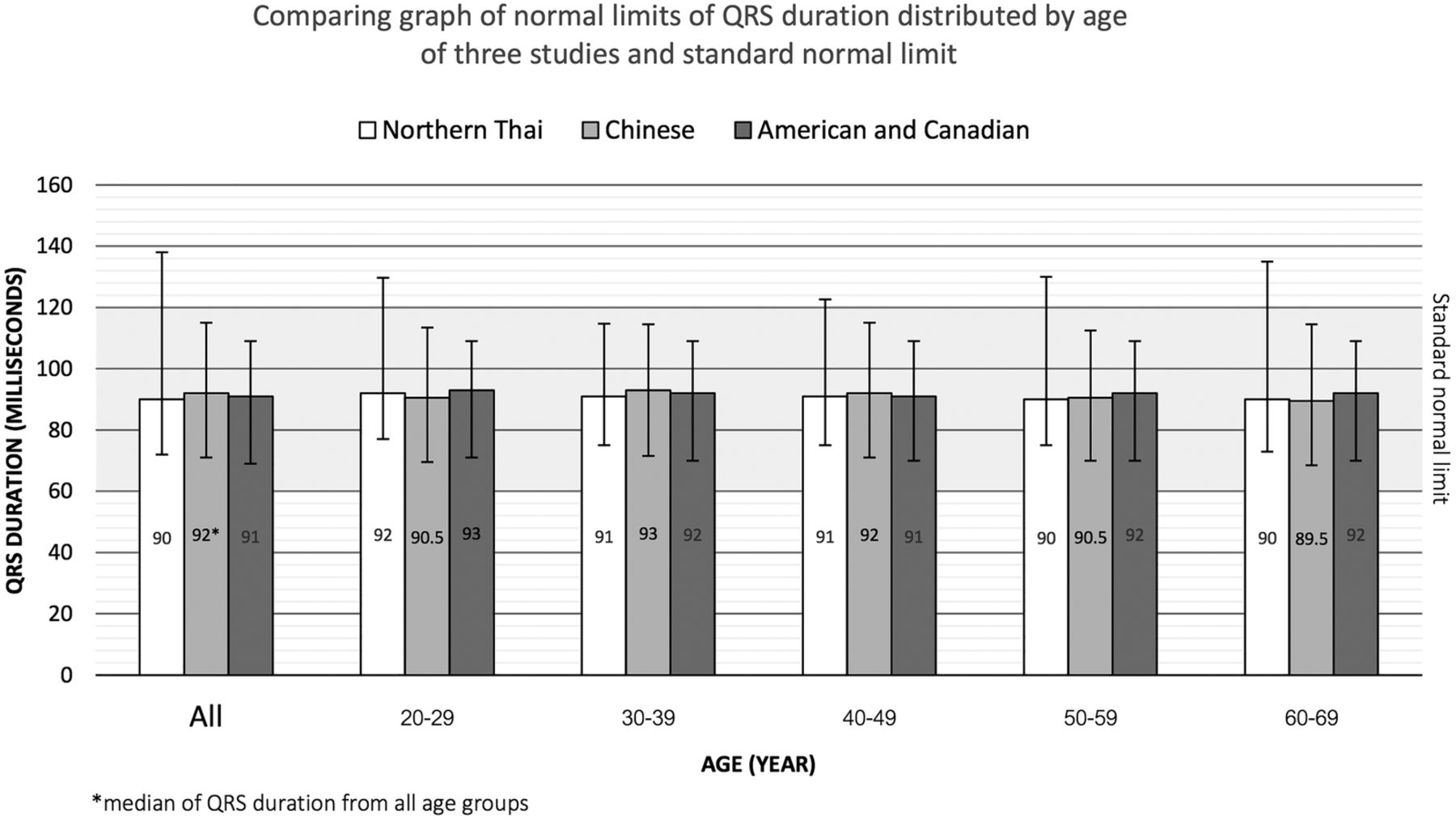
Normal limits of QRS duration distributed by age.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Normal limits of Sokolow-Lyon (SL) index distributed by age.
Factors affecting ECG parameters
Age factor
Heart rate
In this study, heart rate tends to decrease with increasing age in accordance with the report from Chinese and Western subjects. However, our result is in contrast with the study of Nigerian subjects. The authors of that study suggested that the higher heart rate might be influenced by patients’ nervousness. Nevertheless, the decreasing trend of heart rate shows that we should be concerned about the possible need to adjust the criteria for bradycardia and tachycardia, especially in elderly people. This suggestion of lowering the criteria was also proposed by Wu et al for the Chinese population. From our observations, there is no indication that it is necessary to change the diagnostic criteria for all age groups. For example, bradycardia and tachycardia should only be considered for adjustment for some age groups. In this study, the traditional criteria can still be applied to young and middle-aged groups, but we propose that the upper and lower limits of heart rate should be decreased by 5 bpm in people aged >50 years.
PR interval
The average PR interval in this study increases with age as in Chinese and Western subjects, but the PR interval in Nigerian subjects did not change with increasing age. Most of the upper limits of our PR intervals from patients aged >20 years are longer than 200 ms in men and women. The age related criteria of the PR interval should be reconsidered in those groups for Northern Thai people.
QRS duration
All studies in Chinese, Western, and Nigerian subjects showed similar results—namely, that QRS duration was quite stable in all age groups. However, the upper limit of QRS duration in most age groups is >120 ms. Therefore, we suggest that the criterion for prolonged QRS duration should be extended to 160 ms in males older than 40 years and in females older than 50 years.
QTcB
In this study, the average QTcB interval increases with age, the same finding as in the report on Chinese subjects. The study of Western subjects reported that QTcB interval increased in females aged 30–99 years old. Interestingly, the average QTcB interval in this study was much longer than in Chinese, Western, and Nigerian subjects and much longer than the general upper and lower limits. For further study, we have to confirm this finding with clinicians that QTcB is really longer in Northern Thai people. Following this confirmation, it will be necessary to derive a new general criterion of QTcB interval for Northern Thai people. The appropriate lower and upper limits of QTcB interval for Northern Thai people should be about 380 ms and 495 ms, respectively.
QRS axis
We found the average QRS axis progressively deviated to the left with increasing age. The studies of Chinese and Western subjects also reported the same trend. QRS axis criteria should be adjusted by age groups. Normal QRS axis in patients aged <30 years should be set to 60–100°; in patients aged between 30–50 years it should be set to 40–60°; and in patients aged >50 years it should be set to 30–40°.
SL index
In this study, SL index does not show an age trend in both genders although there was a small increased value with increasing age in females. In Chinese subjects, RV5+SV1 amplitude decreased with increasing age in males, but it did not significantly change in females. In Nigerians, RV5+SV1 amplitude also did not depend on age. The upper limit of SV1+RV5 amplitude in all age groups in this study is much higher than 3.5 mV, in accordance with other studies. In Nigerians, the upper limit of SL index in the oldest age group had 4.77 mV in males and 5.71 mV in females. In addition, the Chinese study suggested that their threshold in men should be set at 4.2 mV. Accordingly, we suggest that the normal upper limit of SL index should increase to 5.12 mV for Northern Thai people.
Gender factor
Heart rate
The average heart rate in females is slightly higher than in males, similar to the data from Chinese, Western, and Nigerian subjects. With the combination of age and gender factors, heart rate in elderly men is lowest.
PR interval
PR interval for females is shorter than males, corresponding to the relatively higher heart rate. This result is also similar to Chinese and Western subjects. Prolonged PR interval in elderly men should be carefully diagnosed because of the age and gender factors.
QRS duration
QRS duration in males is longer than in females, similar to the data from Chinese, Western, and Nigerian subjects. Gender has more of an effect on QRS duration than age. A possible key reason could be ventricular mass. QRS duration represents ventricular depolarisation and the period of time depends on ventricular mass (if the electrical signal is conducted in a normal conducting pathway). Therefore, a higher volume of ventricular mass in males creates a longer QRS duration. The study in Chinese subjects proposed that a normal limit of QRS duration should be 120 ms for males and 109 ms for females. Another recommendation proposed that ventricular late potentials should be diagnosed when the duration is more than 114 ms in males and 104 ms in females.8 For the Thai population, we might not be able to apply these recommendations because the upper limits of QRS duration in this study were much longer than that. We recommend the upper limits should be 142 ms in males and 132 ms in females.
QTcB
QTcB duration in females is slightly higher than in males, similar to the data from Chinese, Western, and Nigerian subjects. In both genders, the upper limit of QTcB exceeds 440 ms. The study of Chinese subjects recommended a new upper limit regardless of gender and age for the Chinese population. In this study, we also agree with their recommendation to adjust the recommended value to 490 ms.
QRS axis
The QRS axis shifts to the left with increasing age in both genders, similar to Chinese and Western subjects, but the shift is less affected by gender. Several factors were proposed as the causes of the shifting. Wu et al explained that obesity resulted in an upward shift of the diaphragm and a more horizontal position of the heart. Rautaharju et al proposed that QRS amplitude changed due to diseases associated with the cardiovascular system, bodyweight, chest width and depth, and sum of skin fold.
SL index
The averages of SL index in both genders are quite stable with some effect on aging and gender. Two research groups have suggested a new criterion for SL index. For male Chinese, a new criterion should be set at 4.2 mV. For Nigerians, the data showed that upper limits of SL index were 4.77 mV for males and 5.71 mV for females. The research group proposed that a new criterion should be set higher in both genders for Nigerians. The upper limits of SL index in this study were 5.52 mV in males and 4.77 mV in females. Therefore, the upper limit for SL index should be extended to cover these upper ranges.
Race factor
Heart rate
The average heart rate in this study was similar to Chinese subjects but lower than Nigerians and higher than Western subjects. Another study from a large ethnically diverse population of women also reported that heart rate in Asian women was higher than in Caucasian women.5 Another study on ethnic differences showed that heart rates of Saudi Arabians and Indians were higher than for other groups. The heart rate of Jordanian, Filipino, and Sri Lankan subjects were higher than Caucasians.6 We could group the population according to these multiple studies as evidence that heart rate in Caucasians was lowest, Asian was in the middle, and Nigerian and Middle East were highest. Therefore, race is one of the major factors producing the variation of heart rate.
PR interval
The study in Chinese subjects showed that PR interval was equal to Caucasians but shorter than Nigerians. However, the PR interval in this study was longer than in the Chinese and Western groups. Two previous studies have observed PR interval in different populations.5 ,6 These reports showed that PR interval was in the range 150–165 ms but the values did not show a significant difference between races. The difference in PR interval might be influenced by other factors such as heart rate and age. One study has filtered the heart rate factor by applying a specific formula. The result revealed that PR interval and heart rate have a linear relationship—PR interval decreasing with increasing heart rate. Their observation showed that PR interval in adults aged 40 years and older is significantly dependent on heart rate and age. In order to have more appropriate consideration for PR interval, age-specific PR adjustments should be applied to eliminate the heart rate dependence of PR.
QRS duration
The average QRS duration in this study was similar to that found in Chinese and Western subjects but higher than in Nigerians. The study of QT interval in a diverse population of women showed a similar QRS duration in Caucasian, Asian, and American Indian subjects.5 In addition, another study6 of a diverse population showed that the average QRS duration in Caucasian, Saudi, Indian, Jordanian, Filipino, and Sri Lankan subjects was between 80–90 ms, which was similar to this study. A study published in 1954 showed that there was no change over a 10-year period in mean QRS duration in any given heart.7 Therefore, QRS duration is not a time dependent value, and is little effected by age and race factors, but is effected more by gender.
QTcB
The average QTcB in this study was higher than in Chinese, Nigerian and Western subjects. Our results showed the average QTcB was between 430–440 ms whereas in the other subjects it was between 400–420 ms. One prior study in QT derived from a large ethnically diverse population of women showed that the average QTcB was 400 ms. That study concluded that racial differences can be ignored, except that the mean adjusted QT values were 10 ms greater in Asian women than in the other racial groups. This result supports our finding that QTcB in females was higher than other averages. Another study in a diverse population showed that the average QTcB in Caucasian, Saudi, Indian, Jordanian, Filipino, and Sri Lankan subjects was lower than the results from this study. Their study showed that QTcB was around 380 ms in males and 410 ms in females, but our finding showed that QTcB was 435 ms in males and 438 ms in females. Overall, QTcB in this study has a higher value than in other studies. A further more detailed study is needed to find the causes of this difference.
QRS axis
The QRS axis in this study shifted to the left with increasing age, consistent with similar results found in Chinese, Nigerian and Western subjects. We could not find a significant difference between races for QRS axis.
SL index
This study did not show a significant trend for SL index in either age or gender factors. The average SL index in this study was similar to the result in Chinese subjects. One pattern that was recognised in the study in Chinese subjects was that the upper normal limit of SL index decreased with increasing age in males. However, other studies in Western and Nigerian subjects did not find a significant difference.
Conclusion
For the Northern Thai population, consideration should be given to decreasing the upper and lower limits of heart rate by 5 bpm for patients aged >50 years. First degree AV block should be more carefully considered as a possible diagnosis in patients aged >60 years. One criterion for prolonged QRS duration can be applied for all age groups in light of the awareness that the average QRS duration in males is longer than females. The awareness of prolonged QT syndrome detection is emphasised in older age groups because of the slight progression of QTcB with increasing age. QRS axis tends to deviate to the left because of the aging process and its effect on the chest, bodyweight, and diseases associated with the cardiovascular system. Consideration should be given to extending the upper limit of SV1+RV5 in young and old age groups from the current standard criterion.
Acknowledgments
I would like to thank the Tilley family who always gave me advice, our team from the IT department who are working very hard to help me implement the system, the nurses from the ECG room who learnt and provided a new electronic ECG service, and companies which provided us with a trial cardiograph. Most importantly, thanks to the Maharaj Nakorn Chiang Mai Hospital, Department of Physiology, Faculty of Medicine, Chiang Mai University for facilitating this project.
References
Footnotes
Contributors PK, a full time lecturer, is the main investigator of this research. He supervised PS, a second year medical student, WL a third year medical student, LL, a third year medical student, and CP a third year medical student. Those students assisted PK to conduct the research. PK established the research project, conceived of the study, submitted an ethical approval, critically reviewed the study proposal, initiated the study design, collected the data, approved the final manuscript, and submitted the paper. PS comprehensively wrote the introduction and added relevant findings from other research, and illustrated the tables and figures. WL, LL, and CP cleaned the raw data, included and excluded subjects, conducted the statistical analysis, processed the analysis, and noted the interpretations. WL helped PK to write the discussion. All authors reviewed research articles, refined the study protocol, and read and revised the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.