Article Text

Statistics from Altmetric.com
Introduction
Diabetics are at an increased risk of cardiovascular morbidity and mortality as a consequence of inherent metabolic abnormalities and comorbidities. Furthermore, these patients derive less benefit from the standard therapies of coronary artery disease (CAD); the unique pathophysiological response to arterial injury has a profound effect on outcomes of percutaneous coronary interventions (PCIs). However, as the technology, techniques and experience of operators in PCI are evolving, the understanding of revascularisation strategies and patterns of clinical practice are changing. In this review, we discuss specific issues related to cardiac intervention in diabetics.
Magnitude of the problem, pathophysiology and mechanistic insights into adverse outcomes after revascularisation
Currently, diabetes affects >180 million people worldwide. In the current era of advanced medical therapy, improved medical facilities and medical infrastructure, the term myocardial infarction (MI) equivalent might not hold true.1 However, despite improved outcomes, the gradient of increased risk of mortality and morbidity as compared with non-diabetics persists throughout the spectrum of CAD. Diabetics constitutes around one quarter of patients undergoing revascularisation. Both types of revascularisation strategies have been evaluated extensively. Preoperative mortality, repeat revascularisation and long-term mortality are the issues of concern.
Diabetes is a metabolic disorder characterised by chronic hyperglycaemia and insulin resistance. Disturbed delicate balance of fibrinolytic system as well as abnormalities of platelet structure and function results (box 1) in a persistent prothrombotic milieu.2 (A) Metabolic factors: Hyperglycaemia include endothelial dysfunction, vascular effects of advanced glycation end products, adverse effects of circulating free fatty acids and increased systemic inflammation. (B) Vascular anatomic characters: Diabetics have more frequent diffuse disease, higher prevalence of extensive CAD, left main disease, multivessel disease and occlusions. The narrow calibred vessels are associated with impaired collateral development. (C) Adverse prothrombotic milieu and high atherosclerotic burden: Proteofibrinolytic system and platelet biology are unfavourably altered in diabetes and a state of platelet activation exists. Glycoprotein IIb/IIIa (GP IIb/IIIa) receptor density is high and increased thrombosis is an independent marker of adverse outcomes following PCI. Diabetics have a higher atherosclerotic burden and plaques, which are high risk and vulnerable to rupture.
Abnormalities of platelet function
▸ Increased thromboxane A2 synthesis/arachidonic acid metabolism
▸ Decreased nitric oxide and prostacyclin production
▸ Decreased antioxidant levels
▸ Increased expression of activation-dependent adhesion molecules (eg, glycoprotein IIb/IIIa, P-selectin)
▸ Increased platelet microparticle formation
▸ Increased platelet turnover
Adverse outcomes after coronary intervention in diabetics
Balloon angioplasty and bare metal stent implantation
Procedure-related and in-hospital mortality
Early studies had shown more procedural complications and in-hospital complications twofold higher in diabetics. However, the rate of angiographic success was same as non-diabetics.3 The complication rates fell in later studies, in-hospital mortality (1.9% vs 4.3%), MI (1.0% vs 7.4%), an in-hospital coronary artery bypass grafting (CABG) surgery (0.8% vs 6.2%).4 Patients with diabetes poorly tolerate the ischemic complications of PCI.5 Renal dysfunction after PCI occurs more frequently in diabetics.6
Repeat revascularisation and long-term outcomes
Initial data from the National Heart, Lung and Blood Institute reported restenosis rates exceeding 47% as compared with non-diabetics.7 An absolute 10% difference exists between patients with and without diabetes regarding repeat revascularisation. The restenotic process more often results in total occlusions, MI and ventricular dysfunction in diabetics than in non-diabetics.8
Drug-eluting stents (DES)
Angiographic and clinical outcomes
DESs altered both rate and type of restenosis compared with bare metal stents (BMSs) in diabetic population. However, the result was still inferior to that of non-diabetics. The TAXUS IV and SIRIUS trials provided enough evidence favouring DESs and showed reduction of target lesion revascularisation and restenosis rates to the tune of 65%.9 ,10 Prevention of REStenosis with Tranilast and its Outcomes, the largest contemporary restenosis trial till date, showed that compared with non-diabetic patients, patients with diabetes were older, more often had comorbid health problems and had more complex culprit stenoses. But even after adjustment for these differences in baseline characteristics, diabetics still had higher 9-month rate of death (relative risk (RR) 1.87, 95% CI 1.31 to 2.68), target vessel revascularisation (TVR; RR 1.27, 95% CI 1.14 to 1.42), and the composite of death/MI and TVR (RR 1.26, 95% CI 1.13 to 1.40).11 Diabetic status was also predictive of major adverse cardiac and cerebrovascular events (MACCE) and mortality in long term.12 ,13 While DESs, compared to BMS are effective in reducing the need for repeat revascularisation but whether this translates into reduction in MI and lesser deaths is not clear.14
DES compared with BMS in diabetes
DESs reduce the rate of angiographic restenosis and need of repeat revascularisation in all patients and diabetics too seem to derive benefit from DES as compared with BMS. Results of SIRIUS and TAXUS IV trials in the diabetic subgroup were encouraging. In DIABETES Trial15 target-lesion revascularisation at 9 months was significantly lower in the sirolimus-eluting stent (SES) group as compared with that in the BMS group (6.3% vs 31.3%). However, in all these trial, diabetes was a significant predictor of target lesion revascularisation. Furthermore, whether reduced rates of restenosis translate into mortality benefit in the complex multivessel PCI in diabetics is unknown.
SESs compared with paclitaxel-eluting stents (PESs)
Three major trials were compared head to head, the SESs and PESs. ISAR-DIABETIS trial16 included patients with angina or a positive stress test and a native vessel culprit lesion (exclusion: ST-segment elevation MI, LMS disease and restenosis). Median angiographic follow-up was 196 days. The extent of in-segment late luminal loss was 0.24 mm greater in the paclitaxel-stent group than in the sirolimus-stent group (p=0.002). In the SIRTAX trial,17 the HR for MACCE was less in SES when compared with that in PES patients and this difference was more pronounced in diabetics. The REALITY trial was a prospective, randomised clinical study, designed to compare the safety and efficacy of the Cypher (SES) and the Taxus (PES). The primary endpoint was in-lesion binary restenosis rate by quantitative coronary angiography at 8 months post procedure. There was no difference between the groups with regard to the rate of binary angiographic in-lesion restenosis at 8 months. Angiographic parameters favoured a more robust inhibition of neointimal hyperplasia by the sirolimus-eluting Cypher stent. There were no differences between the groups with regard to in-lesion restenosis rates. There was a higher incidence of in-stent thrombosis (<30 days) in Taxus-treated patients.
The resolute zotarolimus-eluting stent (ZES) and diabetes mellitus
The resolute ZES is a new-generation DES consisting of a thin-strut cobalt alloy bare metal stent coated with a durable biostable polymer and the cell-cycle inhibitor zotarolimus. While DESs have been recommended for PCI in patients with diabetes, no DES prior to the resolute has been specifically indicated by the US Food and Drug Administration for use in this high-risk population based on 1-year target vessel failure (TVF) outcomes for on-label non-complex resolute DM patients against a performance goal derived from a meta-analysis of published literature (which included six trials with Cypher SES and Taxus PES) and pooled data for the endeavour ZES. The composite TVF endpoint included cardiac death, MI and TVR. At 1 year, the rate of TVF for the 878 non-complex diabetic resolute patients was 7.8%, significantly lower than the performance goal of 14.5% (p=0.001). The recent data presented at the American College of Cardiology18 also report similar results.
Stent thrombosis after DES and disease progression
Insulin requiring diabetes is a strong and independent risk factor for probable and definite stent thrombosis with a risk twofold more than non-diabetics.19 ,20 As discussed above, diabetics have a faster progression of native disease and appearance of new lesions is approximately 30% and attributed primarily to new lesions in the treated vessels.21
Percutaneous revascularisation compared with surgical revascularisation (multivessel PCI vs CABG)
Surgical revascularisation is the recommended strategy in diabetics with multivessel disease, but recent trials have resulted in a changing paradigm for revascularisation strategies. Still, most randomised controlled trials have shown higher rates of repeat revascularisation procedures after PCI and survival advantage for CABG over PCI in patients with diabetes.
Trials with long-term results
The Emory Angioplasty versus Surgery Trial (EAST) compared a strategy of initial percutaneous transluminal coronary angioplasty (PTCA) versus CABG in patients with multivessel coronary heart disease. The 8-year survival was greater in patients with diabetes who underwent CABG (75.5%) compared with those who underwent PTCA (60.1%; p=0.23). Diabetic subjects who underwent PCI had a reduced survival rate (60.1% vs 82.6%; p=0.02). Repeat revascularisation occurred in 26.5% of the CABG-treated patients and in 65.3% of the PTCA-treated patients (p=0.001) over a period of 8 years.22 Bypass Angioplasty Revascularization Investigation (BARI) investigators recently reported sustained survival benefit of CABG at 10 years, 71.0% for PTCA and 73.5% for CABG. However, treated DM patients randomised to CABG had higher survival than those randomised to PCI (PCI 45.5% vs CABG 57.8%, p=0.025).23
Registries with long-term result
In contrast to results of EAST, BARI and CABRI24 which favoured CABG, the 20-year results of a European registry showed reduced survival rates in surgically treated patients.25
CABG versus PCI with BMS
Table 1 summarises major randomised trials of multivessel PCI using stents versus CABG, which included patients with diabetes. A recent meta-analysis26 included 10 major studies of revascularisation reported that in patients with diabetes (CABG, n=615; PCI, n=618), mortality was substantially lower in the CABG group than in the PCI group (HR 0.70, 0.56–0.87 95% CI); unlike non-diabetics where it was similar (HR 0.98, 0.86–1.12; p=0.014).
Trials comparing bare metal stents with CABG (results for diabetic subgroup)
CABG versus PCI with DES
The SYNTAX trial was a landmark contemporary trial. In diabetics the 1-year composite MACCE rate was significantly higher after PES treatment compared with CABG treatment (RR 1.83). The RR of repeat revascularisation of PES over CABG was 3.18 in diabetics as compared with 1.94 in non-diabetics. Compared with CABG, diabetics had higher mortality after PES use in highly complex lesions, that is, SYNTAX score >33, (4.1% vs 13.5%). Revascularisation with PES resulted in higher repeat revascularisation for both patients without diabetes (5.7% vs 11.1%) and patients with diabetes (6.4% vs 20.3%). The authors concluded that CABG remained the standard of care in patients of diabetes with left main or triple vessel disease. Table 2 summarises other contemporary trials. Arterial Revascularization Therapies Study–Part II27 was a major trial which concluded that PCI using SES was safer and more efficacious than using BMS in both diabetic and non-diabetics and was a valuable alternative to CABG in patients with diabetes as well. FREEDOM was a landmark trial asserted that CABG scores over PCI with DESs in patients with diabetes (all-cause mortality and MI). CABG was better, regardless of SYNTAX score, number of diseased vessels, ejection fraction, race or sex of the patient.
Trials comparing drug-eluting stent (DES) with CABG in diabetic subjects
Revascularisation versus medical therapy
In the BARI 2D trial, the rates of death from any cause did not differ significantly between the revascularisation group and the medical therapy group. Prompt revascularisation significantly reduced major cardiovascular events, as compared with intensive medical therapy, among patients who were selected to undergo CABG largely because of a reduction in MI events. The COURAGE Trial also showed that PCI with optimal medical therapy was no better than optimal medical therapy alone for patients with stable CAD in diabetics and non-diabetics.
Improving outcomes of PCI in diabetics
Management of hyperglycaemia after CABG or PCI in patients with diabetes
It is proposed that the strict control of hyperglycaemia immediate postoperative period may have beneficial effect on myocardial energetic. Indirect support for this concept came from studies in critically ill patients with diabetes. No specific studies are available to address this issue and no trial has shown improved PCI outcome after ST-segment-elevation myocardial infarction with the administration of insulin or glucose insulin potassium.
Antiplatelet agents
GP IIb/IIIa receptor antagonists have assumed an important place and provided improved outcomes after PCI in diabetics. A pooled analysis from three trials (n=1462) investigating the use of the GP IIb/IIIa inhibitor, abciximab with PCI in patients with diabetes showed a 2% absolute mortality reduction (4.5% vs 2.5%, p=0.03) at 1 year.28 In recent meta-analysis of six trials of various GP IIb/IIIa inhibitors in acute coronary syndromes, mortality benefit was greater in patients with diabetes (n=1279) who underwent PCI during the index hospitalisation (4.0% vs 1.2%, p=0.002). Contemporary PCI guidelines recommend GP IIb/IIIa inhibitors in patients with unstable CAD and in elective PCI patients with risk factors, such as diabetes. However, ISAR-SWEET trial did not report significant impact of abciximab on the risk of death and MI in patients with diabetes undergoing PCI, but abciximab reduced the risk of restenosis in patients with diabetes receiving BMS.
Bioabsorbable stents
After intense preclinical research, there has been a revolutionary advance that of bioresorbable vascular scaffolds (BVSs), which are designed to provide temporary radial support to the vessel, to facilitate administration of antiproliferative drugs and to promote recovery of the artery’s normal structure and physiological function by gradual removal of the scaffolding through a process of biodegradation. BVSs have several advantages, including physiological recovery of the vessel, reduced stent thrombosis and need for antiplatelet therapy, fewer constraints on future interventions in the vessel and its collaterals and the possibility of using non-invasive diagnostic exams, particularly CT angiography. One-year clinical outcomes of patients with diabetes treated with everolimus-eluting BVS, a pooled analysis of the ABSORB and the SPIRIT trial, patients with diabetes treated with the BVS showed similar rates of device-oriented composite endpoint compared with non-diabetic patients treated with the BVS and patients with diabetes treated with everolimus-eluting metal stents (EESs). There were no differences in the incidence of definite or probable scaffold/stent thrombosis (0.7% for both diabetic and non-diabetic patients with the BVS; 1.0% for patients with diabetes with the BVS vs 1.7% for patients with diabetes with EES in the matched study group).
Primary PCI in diabetics
Patients with diabetes more often present with late and with congestive heart failure, after a ST elevation MI. CABG is usually done in cases with mechanical complications or failed PCI. PCI is more effective than fibrinolytic therapy. Studies comparing fibrinolytic therapy with primary angioplasty with or without use of GP IIb/IIIa report better short- and long-term outcomes with primary PCI in diabetics. In a recent study of 6315 patients (14% diabetics), 30-day mortality (9.4% vs 5.9%, p=0.001) was higher in patients with diabetes.29 Mortality was lower after primary PCI compared with fibrinolysis in both patients with diabetes (unadjusted OR, 0.49, 95% CI 0.31 to 0.79, p=0.004) and without diabetes (unadjusted OR 0.69, 95% CI 0.54 to 0.86, p=0.001). Recurrent infarction and stroke were also reduced after primary PCI in both patient groups. After multivariable analysis, primary PCI was associated with decreased 30-day mortality in patients with and without diabetes, with a point estimate of greater benefit in patients with diabetes. In non-ST MI, patients with acute coronary syndrome, there is no interaction between the effect of myocardial revascularisation and diabetic status.30 However, an early invasive strategy was associated with improved outcomes; in TACTICS-TIMI 18, the benefit in patients with diabetes was greater than in non-diabetics.
Outcomes in insulin requiring versus non-insulin requiring diabetes
The issue of adverse outcomes in patients with insulin requiring diabetes (IRDM) versus those who are non-insulin requiring diabetes is far less than resolved. However, the published data indicate that short-term and mid-term outcomes may be worse in IRDM population. In a large, real-world multicenter registry of diabetic population from Italy, the use of DES was associated with a moderate reduction in the 2-year risk of TVR, a benefit that was limited to non-insulin-dependent diabetic patients.
In the TRUE Study which evaluated clinical impact of the Taxus stent in non-insulin-requiring vs insulin-requiring diabetics, the 1-month MACE rate was similar (p=0.4) between the two groups, 3% vs 5%. At 7 months, the MACE rate was significantly (p=0.001) lower in the group of diabetics on oral agents (8.5%) than in insulin-requiring diabetics (25.3%). This difference was constant (p<0.01 for all) across deaths (0% vs 8%), TVR (8.4% vs 20.7%) and TLR (3.1% vs 14.6%), while the rate of MI was similar (5.3% vs 4.8%, p=0.7). Further studies are required to evaluate the long-term effects.
Contemporary guidelines and approach to revascularisation in diabetics
Contemporary PCI guidelines31 emphasise the long-term survival benefit of CABG over PCI in diabetics with multivessel disease. However, individual clinician judgment on the revascularisation strategy remains an important decisive factor. Although PCIs with DES have narrowed the gap with surgery, the effectiveness of PCI in CABG-eligible diabetic patients with stable multivessel disease is still not clear. Primary PCI is preferred over fibrinolysis if it can be performed within recommended time frame (class I, level of evidence-a). The use of DES is recommended to reduce restenosis and repeat TVR (class I, level of evidence-a). CABG should be considered when the extent of the CAD justifies a surgical approach (especially MVD), and the patient's risk profile is acceptable (class II, level of evidence-a). Figure 1 outlines an approach to choice of revascularisation in diabetics with multivessel CAD.
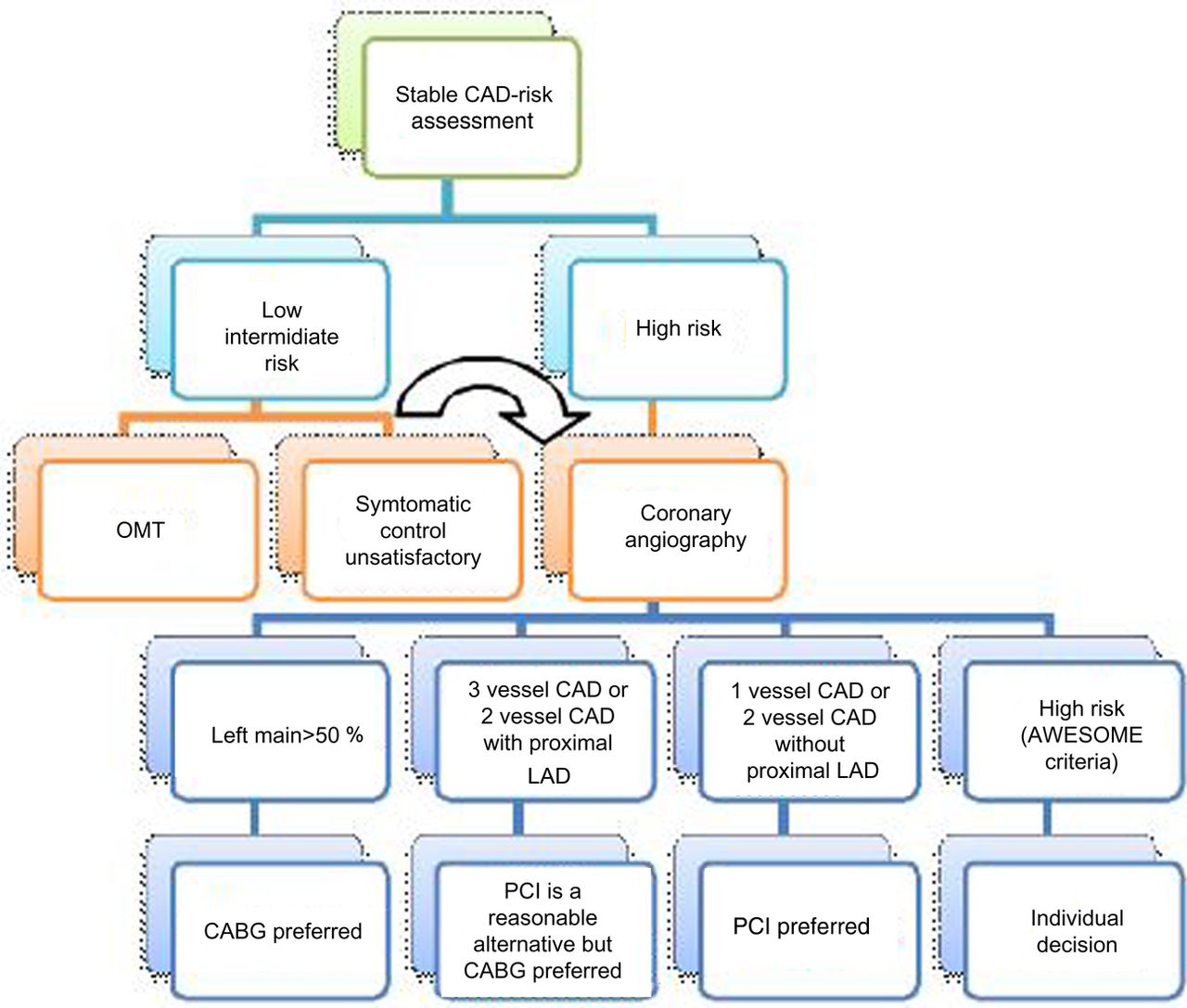
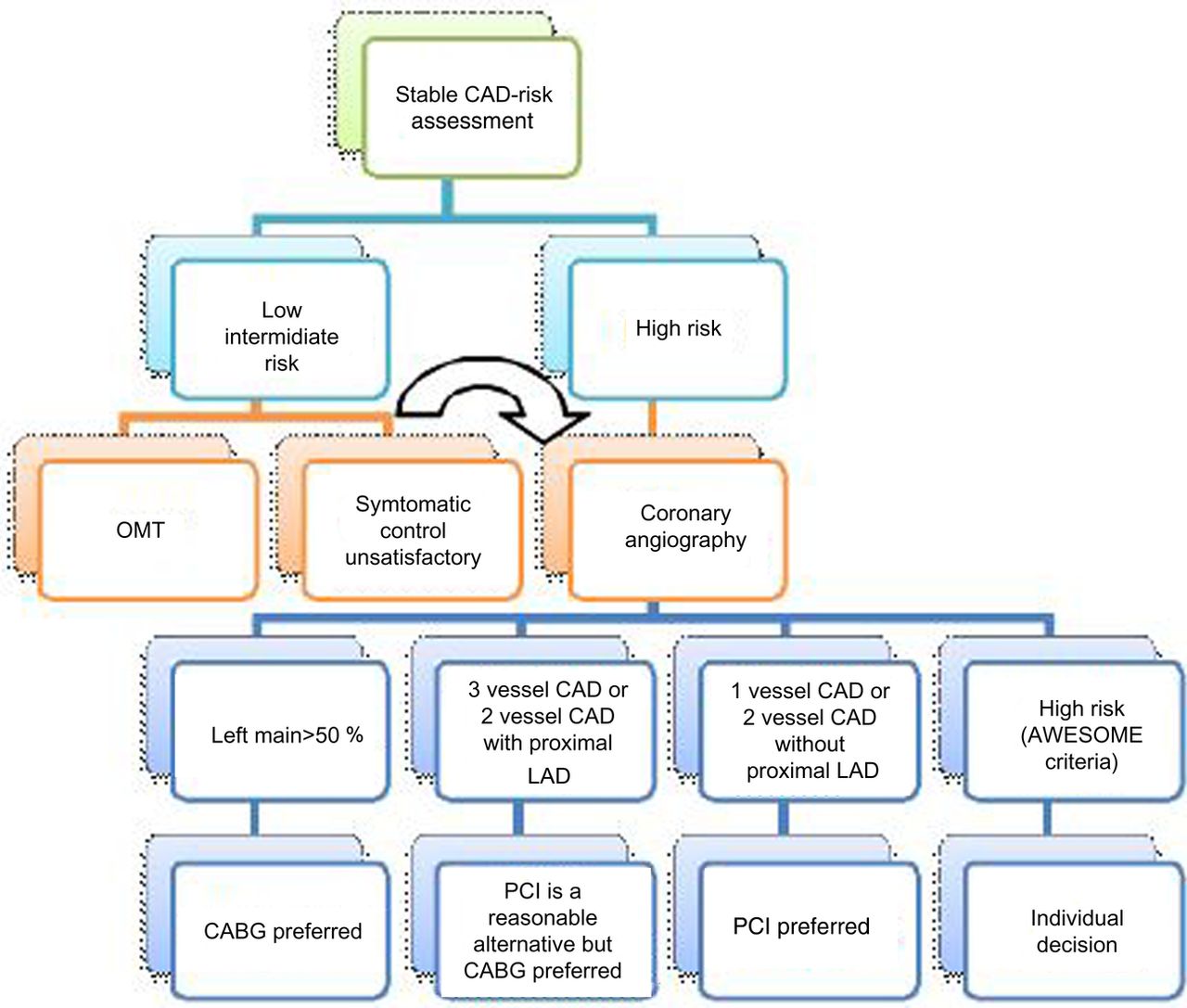{kind=link}
Revascularisation algorithm in diabetics. CABG, coronary artery bypass grafting; CAD, coronary artery disease; LAD, left anterior descending artery; OMT, optimal medical therapy; PCI, percutaneous coronary intervention.
Conclusion
The expanding diabetic population and burden of CAD-related mortality and morbidity mandates a clear perspective in optimising the management of such patients, especially mode of myocardial revascularisation. This becomes even more important in view of the multiple adverse pathophysiological and anatomic characteristics and unique response to arterial injury which confer a relatively poor prognosis and worse outcome after revascularisation procedures. Several early studies comparing CABG surgery versus balloon-only PCI or BMS in subgroups of patients with diabetes with multivessel CAD demonstrated a survival advantage and less repeat revascularisation procedures with an initial surgical strategy. Recent advances in technique use of DES and progress in medical therapy appears to bridge the gap and have made PCI a viable alternative to CABG. Currently, mortality after PCI is comparable with that after CABG, but the need for subsequent revascularisation is greater after PCI. Thus the revascularisation strategy should be individualised based on patient profile, anatomic characteristics of lesions. In general, it is a good idea to have a Heart Team Approach which involves combined assessments by primary physician, interventional cardiologists and cardiac surgeons, also taking into account the patient preference.
References
Footnotes
Contributors In relation to our manuscript, we declare that the authors were actively involved in the drafting, revision and final approval of the manuscript, hence we are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.