Article Text

Statistics from Altmetric.com
A 48-year-old man was referred to our institution for acute limb ischaemia. He had been diagnosed with cutaneous T-cell lymphoma, so-called mycosis fungoides by gene rearrangement analysis of skin biopsy samples 9 years ago. He had received prednisolone 5 mg daily and phototherapy for mycosis fungoides. Although allergy symptoms and signs including asthma, peripheral neuropathy and glomerulonephritis had not been evident, his rashes had been worsening in his face and abdomen for a few months.
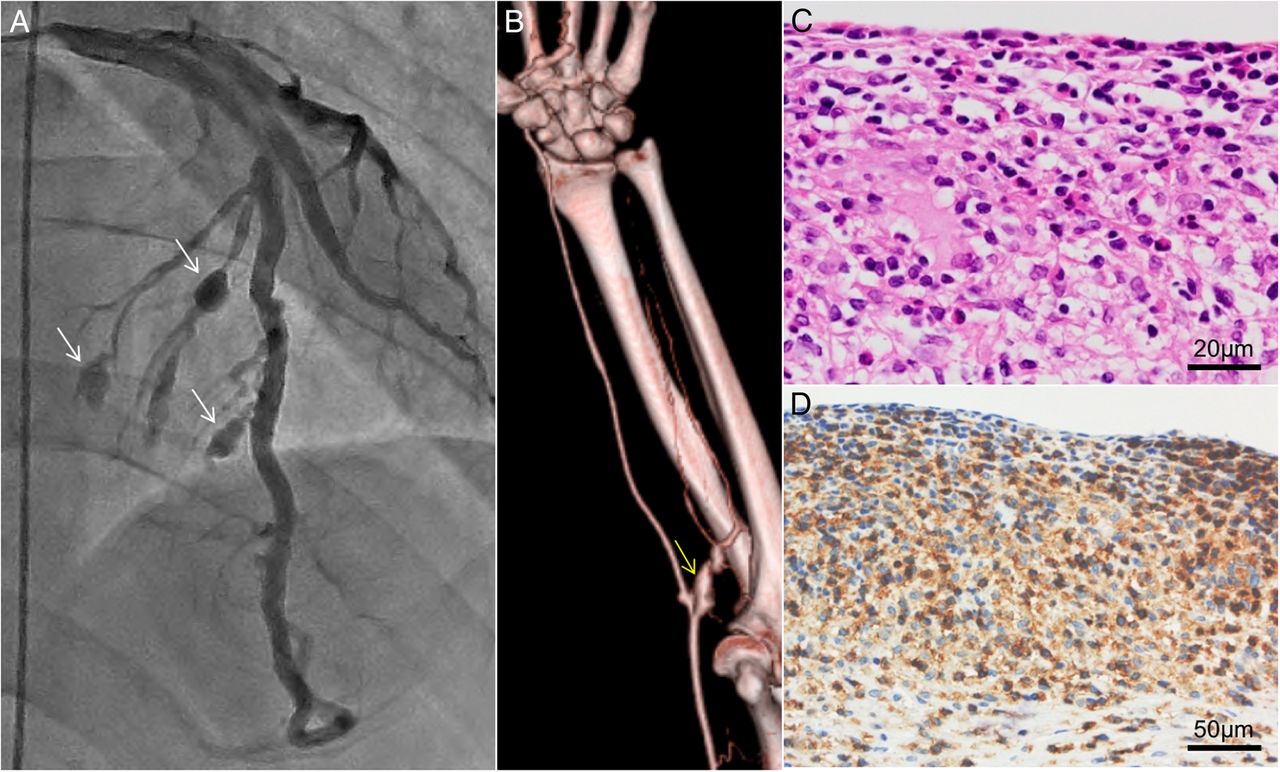
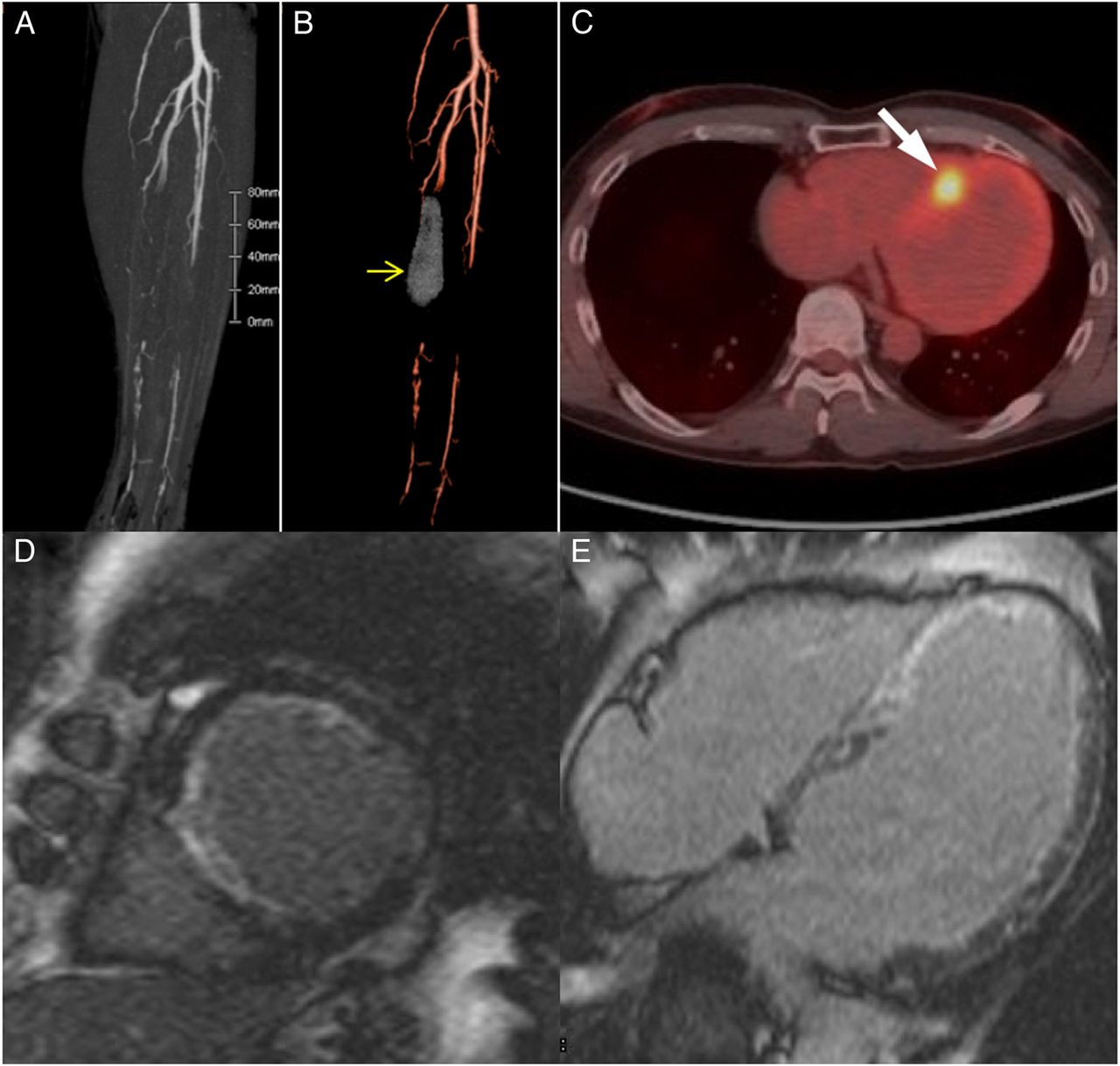
On examination, enhanced CT revealed thrombotic occlusion in the left posterior tibial artery (figure 1A, B) and multiple aneurysms of various systemic peripheral vascular beds, including those of posterior tibial artery, ulnar artery and so on. Laboratory test showed slight elevation of C reactive protein (0.40 mg/dL) and hypereosinophilia (leucocyte count 5.5×109/L, eosinophil 19.4%), whereas antineutrophil cytoplasmic antibody (ANCA) was negative. Cardiac MRI showed late gadolinium enhancement in endocardium side and 18F-fluorodeoxyglucose positron emission tomography demonstrated abnormal uptake in interventricular septum (figure 1C–E). Coronary angiography revealed the asymptomatic development of multiple septal branch aneurysms (figure 2A). End-myocardial biopsy showed severe fibrosis without infiltration of inflammatory cell nor granulomas. Biopsy of the affected ulnar artery demonstrated abundant infiltration of eosinophils and CD4-positive T cells and no evidence of necrotising vasculitis (figure 2B–D).
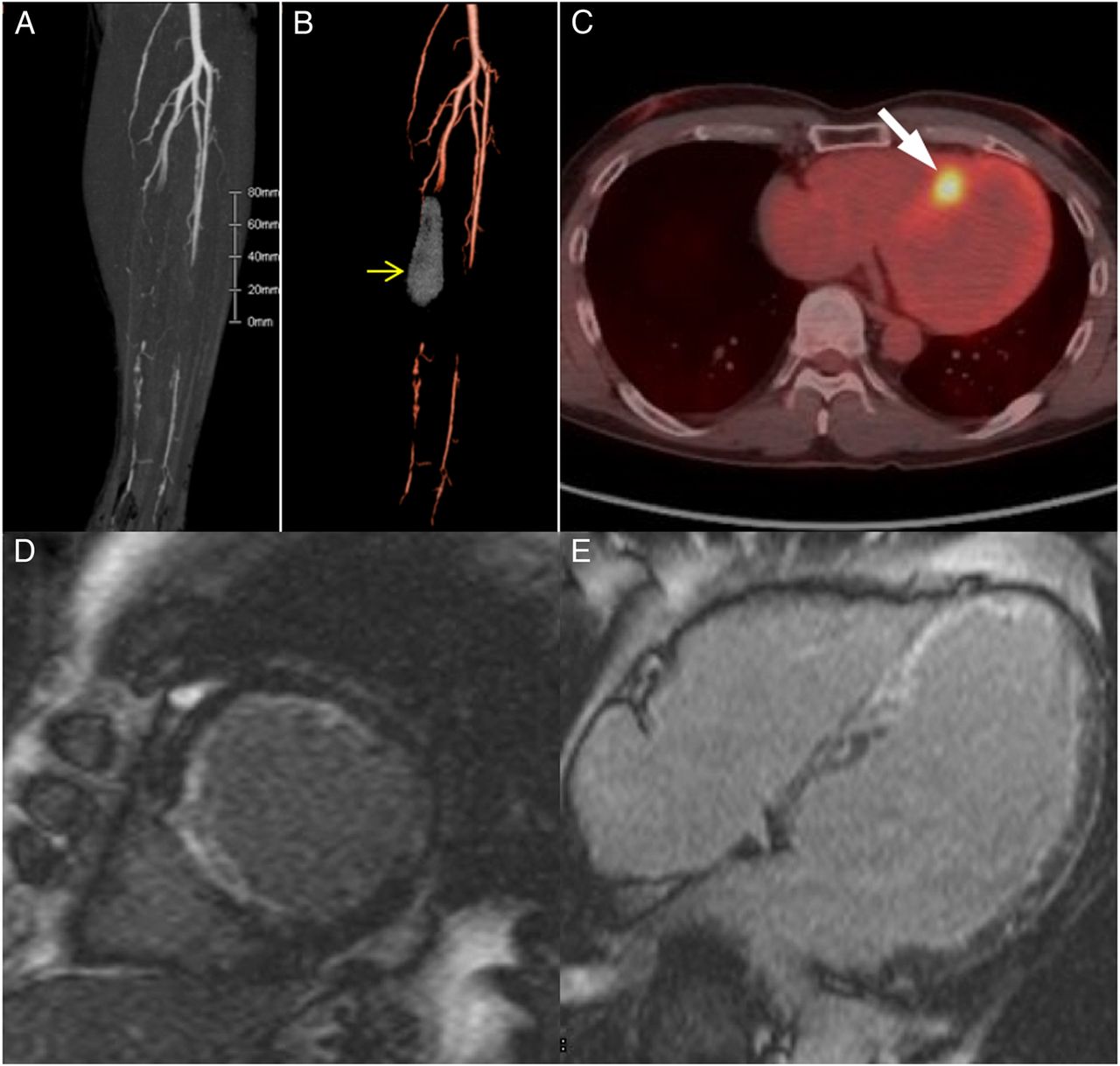
Enhanced CT of the left infrapopliteal artery (A). Yellow arrow showing left posterior tibial aneurysm with thrombotic occlusion (B). Abnormal uptake in interventricular septum (arrow) shown using 18F-fluorodeoxyglucose positron emission tomography (C). Late gadolinium enhancement cardiac MRI in short-axis (D) and long-axis images (E).
{kind=link}
{kind=link}
Multiple septal branch aneurysms (arrow) identified by coronary angiography (A). Left ulnar aneurysm (yellow arrow) in enhanced CT (B). Histopathological findings of an ulnar artery aneurysm showing infiltration of eosinophils and lymphocytes (H&E stain) (C) and CD-4 positive T cells (immunostaining) (D).
Vasculitis with hypereosinophilia is primarily recognised in eosinophilic granulomastosis with polyangiitis (EGPA) that preferentially affects certain organ systems including the airways, peripheral nerves, heart, kidney and gastrointestinal tract. Given that cardiac involvement is reported to be more frequent in patients with EGPA who are ANCA-negative, EGPA is one of differential diagnosis in this case.1 However, lack of typical clinical manifestations of the affected organs, no evidence of a histological necrotising vasculitis and an abundance of eosinophils in this case could advocate other kinds of vasculitis. According to previous reports, angiolymphoid hyperplasia with eosinophilia (ALHE) associated with mycosis fungoides is characterised by the proliferation of blood vessel with infiltration of lymphocyte and eosinophils.2 ,3 This case corresponding to these previous reports suggests cardiac involvement in ALHE with mycosis fungoides. We emphasise the need for an increasing awareness of systemic cardiovascular disorder in patients with mycosis fungoides.
Footnotes
Contributors All the authors were involved in the clinical management of the patients. HY drafted, and OK revised the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.