Article Text

Abstract
Background Heart failure (HF) may influence the lungs and vice versa. However, this interaction and the influence on right ventricular function (RVF) are insufficiently described in patients with HF divided into the recent groups based on left ventricular ejection fraction (LVEF): HF with reduced, midrange and preserved ejection fraction (HFrEF, HFmrEF and HFpEF, respectively).
Methods Overall, 186 consecutive stable patients with HF seen in our outpatient clinic were retrospectively divided into HFrEF (n=70), HFmrEF (n=55) and HFpEF (n=61). Airflow limitation and gas exchange disturbance were measured by spirometry (forced expiratory volume in the first second/forced vital capacity (FEV1/FVC) (%)) and diffusion capacity of the lungs for carbon monoxide (DLCO). Standard echocardiography was performed to measure RV structure (RV diameter) and function (tricuspid annular plane systolic excursion/pulmonary artery systolic pressure (TAPSE/PASP)). Correlations were used to assess possible relations between pulmonary dysfunction and measurements of the RV.
Results None of the investigated parameters differed significantly between the three groups (all p>0.1); FEV1/FVC was 70%±12%, 70%±13% and 74%±10% in patients with HFrEF, HFmrEF and HFpEF (p=0.12) and DLCO was 5.7±1.6, 5.7±1.8 and 5.6±1.6 mmol/min/kPa, respectively (p=0.95). RV structure and function did not differ either (TAPSE/PASP 0.58, 0.60 and 0.57, respectively (p=0.84)). There was a correlation of DLCO with RV function (r=0.34, p<0.001).
Conclusion The investigated cardiopulmonary parameters were comparable in the three HF groups. Diffusion capacity was impaired in more than half of the stable HF population independently of the LVEF and showed a correlation with RV function.
- heart failure – spirometry – echocardiography
Statistics from Altmetric.com
Introduction
Heart Failure (HF) used to be subdivided into ‘HF with preserved Ejection Fraction’ (HFpEF) and ‘HF with reduced Ejection Fraction’ (HFrEF). This segmentation is based on the left ventricular ejection fraction (LVEF) being higher or lower than 40%–50%. Recently, HF with midrange EF (HFmrEF) was added as a new category representing a LVEF ranging from 40% to 49% to better explore this so far largely neglected subpopulation.1
In patients with HF, obstructive lung function abnormalities and disturbance in gas exchange are common.2 3 Both, chronic obstructive pulmonary disease (COPD) and low diffusion capacity, are associated with a worse prognosis.4 5 Nevertheless, the diagnosis of COPD and low diffusion capacity in patients with HF is challenging. Thus, measures of airflow limitation (AL) and diffusion capacity of the lungs for carbon monoxide (DLCO) are only reliable in a stable stage of HF.6 Still, research regarding the presence of lung function abnormalities has been done often in unstable HF patients.7
Precipitating factors contributing to HF hospitalisation in the three different HF groups were recently explored.8 Pneumonia was found to be an important factor in all groups, suggesting that the lungs play an important role in HF patients irrespectively of LVEF. However, information related to pulmonary function is lacking in the three HF groups. Thus, although routine testing of AL and DLCO may be relevant in all stable patients with HF, this has not yet been investigated in three different HF groups to explore if such abnormalities are particularly prevalent in one of these groups.
Vice versa, COPD may influence the heart as well, for example, by causing pulmonary hypertension.9 A study investigating patients with COPD did not show clear functional changes in the right heart.3 In this study, the right ventricular (RV) function was estimated through tricuspid annular plane systolic excursion (TAPSE), which was normal in this and another population.9 Nevertheless, the ratio TAPSE to pulmonary artery systolic pressure (PASP) may be better suited to assess RV function than each of the two variables alone.10 Moreover, TAPSE/PASP may be prognostically important in HF11 but has not yet been studied in a stable HF population subdivided into the three different HF groups.
Therefore, the primary aim of this study was to investigate pulmonary function (i.e., AL and disturbance in gas exchange) and RV function (i.e., TAPSE/PASP) in a stable HF population divided into the three recently defined groups based on LVEF (i.e., HFpEF, HFmrEF and HFrEF). In addition, we investigated the association between cardiopulmonary tests in all patients with HF to explore the potential interplay between pulmonary functional abnormalities and HF on both organs.
Methods
Study design and participants
Between October 2012 and November 2013, consecutive patients visiting the outpatient HF clinic at Maastricht University Medical Center (The Netherlands) were screened for inclusion in this prospective cross-sectional observational study. The purpose of this study was to perform a cohort study until a total of 200 patients were included. Patients were eligible for inclusion if they fulfilled the following criteria: a recent diagnosis of HF based on current guidelines,1 12 age above 50 years and clinically stable conditions for at least 1 month. The diagnosis for inclusion was based on criteria of the European Society of Cardiology (ESC) 2012.12 The separation into the three groups related to LVEF was based on the ESC guidelines 2016. All patients also fulfilled the criteria of HF based on the ESC guidelines 2016. Patients were selected irrespective of LVEF. Patients were excluded if: the measurement of LVEF was lacking, patients were not able to cooperate or when spirometry was clinically contraindicated (detached retina, active tuberculosis and resting pulse >120/ min). Other exclusion criteria included recent surgery, myocardial infarction (<1 month), uncorrected severe valvular disease, lower respiratory tract infection or pneumothorax within the last 2 months and a stroke within the last 12 months. Overall, 205 patients with HF volunteered to participate in this study. Nineteen patients were excluded from further analysis due to missing of recent echocardiography; thus, 186 patients with the diagnosis of HF were eligible for the present study. Patients not included did not differ significantly from those included regarding their baseline characteristics (data not shown). Written informed consent was provided by all patients. This study complies with the Declaration of Helsinki. The local medical ethics committee approved this study (METC 12-2-005 (NL39223.068.12)).
Measurements and data collection
Clinical characteristics
The following patients characteristics were recorded as clinically available: age, gender, HF aetiology, comorbidities, cardiovascular risk factors (diabetes, hypertension, hypercholesterolaemia and smoking), New York Heart Association Functional Classification (NYHA-class), blood pressure, heart rate, (non-invasive) O2-saturation at rest, N-terminal probrain natriuretic peptide (NT-proBNP), electrocardiography and current medication.
Pulmonary assessment
Lung function was measured before and after administration of 200 µg salbutamol. Spirometry (Masterscreen, Jaeger, Würzburg, Germany) was performed by trained respiratory technicians in accordance with the recommendations from the European Respiratory Society (ERS).13 The Global initiative for Obstructive Lung Disease (GOLD) criteria were used to define AL in COPD using the Tiffeneau Index (i.e., forced expiratory volume in the 1st second (FEV1)/forced vital capacity (FVC)%). Thus, patients were diagnosed with COPD if FEV1/FVC after bronchodilatation was lower than 70%. Furthermore, the severity of AL was staged according to the GOLD criteria. An AL was considered to be mild, moderate, severe and very severe if the predicted percentage of FEV1 was ≥80%, 50%–79%, 30%–49% or <30%, respectively.14 Patients fulfilling the diagnostic criteria for COPD were subsequently stratified according to symptoms and future risk.14 DLCO is an individual variable based on the patient’s length, age and gender and is measured according to ERS guidelines.13 15 Reliable FEV1 measurement was available in all but two patients. Twelve patients did not comply sufficiently to reliably assess of DLCO.
Echocardiography
A prerequisite for study inclusion was a comprehensive standard echocardiographic examination within a maximum of 6 months prior to enrolment in the study.16 If a recent cardiac echocardiography was not available, it was repeated for this study. However, in 19 cases, patients refrained from repeating it. These cases were excluded from the study. The following parameters were assessed: LVEF, RV diameter (RVD), RV function (TAPSE/PASP), E/e’ and left atrium volume index (LAVI). In case of absence of regional differences in contractility, M-mode (Teichholz) was used to determine LVEF. If contractility was not uniform for all segments of the LV, biplane Simpson method was used (apical 4-chamber and 2-chamber view). In order to determine LAVI, biplane method from 4-chamber and 2-chamber apical view was used prior to opening of mitral valve and volumes were divided by body surface area. HF was divided into three groups according to recent guidelines based on LVEF: HFrEF, HFmrEF and HFpEF.1
Statistical analysis
Statistical analysis was performed with the use of IBM SPSS Statistics software V.23. Descriptive data are presented as mean ±SD, frequencies (%) or median (IQR) as appropriate. Continuous variables with a normal distribution are compared with the use of analysis of variance test. Continuous variables with a non-normal distribution are compared using the Kruskal-Wallis test. Categorical variables are compared with the use of χ2 test or Fisher’s exact tests, as appropriate. p Values of less than 0.05 are considered to indicate statistical significance. Multiple comparisons are adjusted applying post hoc Bonferroni test. To determine the association between lung function abnormalities and cardiac function, Pearson or Spearman rank correlations are used, as appropriate. Based on the power of this relatively small study population, no multivariable regression analysis was performed on this study population to investigate potential predisposing factors for cardiopulmonary abnormalities (i.e., AL, DLCO and TAPSE/PASP).
Results
Patient characteristics
The baseline characteristics of the three groups based on LVEF are given in table 1. The mean age was 75±10 years, and the majority of the patients were male. The median LVEF was 44 [32–53]%.
Baseline characteristics in an HF population divided into three groups
The most common cause of HF was coronary artery disease in the HFrEF and HFmrEF groups and hypertensive heart disease in the HFpEF group. Cardiac risk factors were similar in all three HF groups. Approximately 80% of the patients had no or little symptoms during daily life activities (i.e., NYHA classes I and II). The NT-proBNP level in the HFpEF patient group was significant lower compared with HFrEF (p=0.01) (table 1).
Spirometry
No significant differences in AL or DLCO were observed between the three groups (table 2). On average, the mean Tiffeneau index was close to the cut-off of being abnormal and approximately half of all patients with HF had abnormal DLCO values. The percentage of predicted DLCO was overall slightly reduced with no significant differences between the three groups. Not unexpectedly, the percentage of predicted DLCO in HF patients with and without AL, respectively, differed significantly (p<0.001) but remained significantly reduced in both groups. There were no significant differences between the three groups based on LVEF in both, patients with and without AL (table 2).
Spirometry findings in an HF population divided into three groups
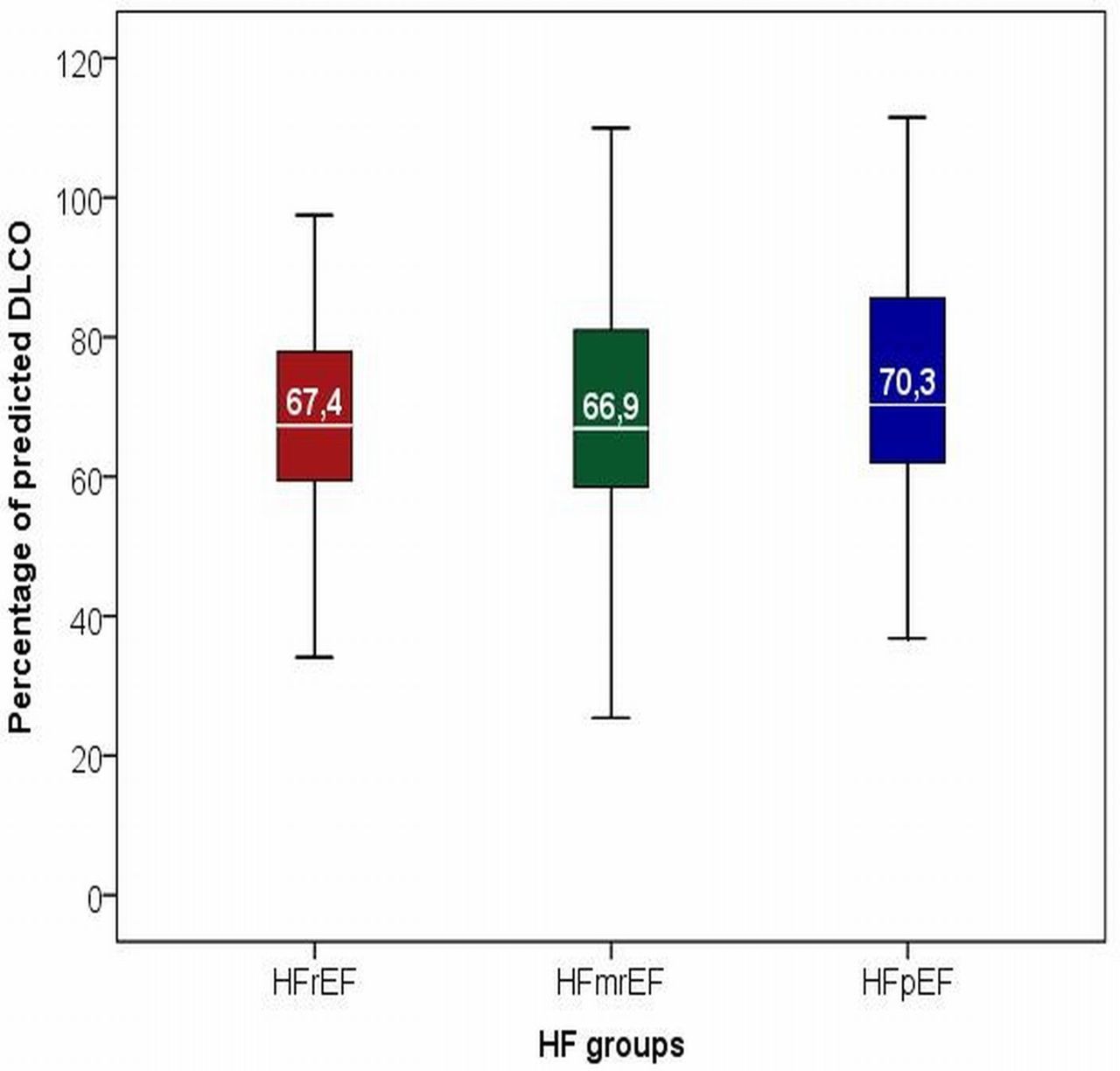
Percentage of predicted DLCO in three groups based on LVEF. DLCO, diffusion capacity of the lungs for carbon monoxide; HF, heart failure; HFmrEF, heart failure midrange ejection fraction; HFpEF, heart failure preserved ejection fraction; HFrEF, heart failure reduced ejection fraction; LVEF, left ventricular ejection fraction.
Echocardiography
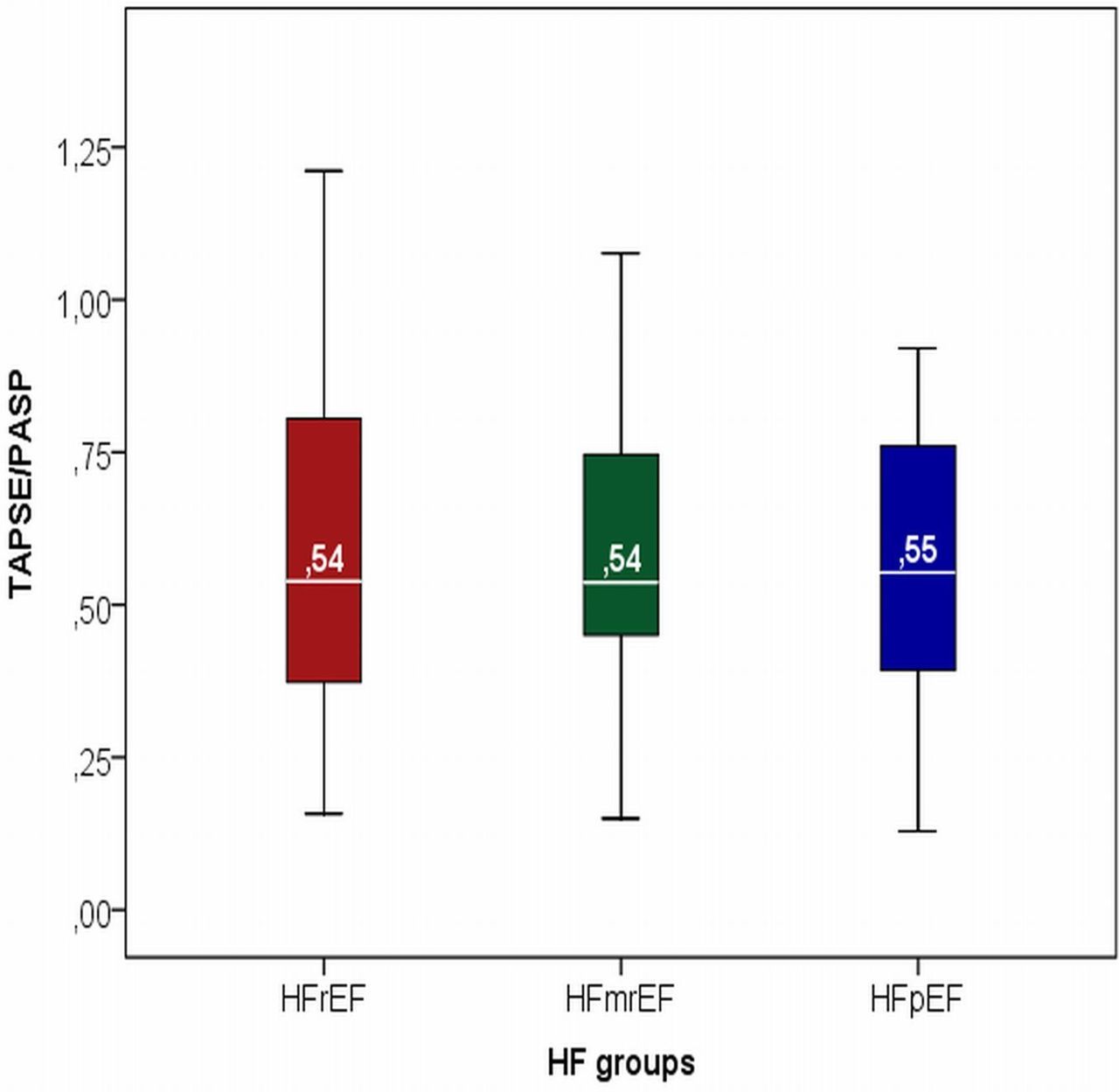
The echocardiographic findings are given in table 3. Measures of RVD and RV function (i.e., TAPSE/PASP) were similar in patients with HFrEF, HFmrEF and HFpEF. The diameter of the RV was enlarged in 30%, and the RV function was decreased in 27% of all patients with HF. Furthermore, parameters of diastolic function (i.e., LAVI, E/e′) were similar in the three groups based on LVEF (table 3).
{kind=link}
{kind=link}
TAPSE/PASP in three groups based on LVEF. HF, heart failure; HFmrEF, gheart failure midrange ejection fraction; HFpEF, heart failure preserved ejection fraction; HFrEF, heart failure reduced ejection fraction; LVEF, left ventricular ejection fraction; PASP, pulmonary artery systolic pressure; TASPE, tricuspid annular plane systolic excursion.
Echocardiography findings in an HF population divided into three groups
Correlations
The correlations between RV function and pulmonary dysfunctions are given in table 4. In general, the correlations were relatively weak.
Correlations (r) between cardiopulmonary tests
FEV1/FVC (%) showed a negative correlation with TAPSE/PASP. DLCO was positively correlated to the TAPSE/PASP and RV diameter and negatively correlated to PASP.
TAPSE/PASP showed negative correlations with RVD and NT-ProBNP. PASP was also positively correlated with RVD and NT-proBNP. (table 4). No correlations are found between TAPSE and DLCO, AL and PASP or between AL and PASP, NT-ProBNP.
Discussion
This study investigated to what extent lung function abnormalities and RV dysfunction might depend on LVEF. Lung function abnormalities and reduced RV function were common in this outpatient HF population without any differences between the three groups based on EF. Furthermore, a weak association between pulmonary and RV function was found across all HF groups, suggesting a limited influence of lung function abnormalities on the RV.
Equal AL in the HF groups
Interestingly, this study showed an equal AL across the whole spectrum of LVEF. Accordingly, patients with HFpEF were not diagnosed more frequently with COPD than the other two groups. This is in line with previous research,17 but not all.18 This variation in COPD prevalence in different HF groups may be influenced by different factors including patient selection but importantly also misdiagnosis of COPD.19 The diagnosis of COPD was often based solely on medical history without further testing and not systematically applying spirometry.7 Diagnosing COPD was also frequently done by performing spirometry in hospitalised patients, where fluid overload may have influenced results significantly.7 It is important to keep these limitations in mind when interpreting results regarding prevalence of COPD in the different groups of HF.7
Possible differences with other studies may also be related to presence of risk factors other than HF, for example, smoking is linked to AL and higher risk of COPD20 and it is obvious that extent of smoking may influence results. Interestingly, left ventricular hypertrophy (LVH) may be also related to FEV1.21 The authors posed the hypothesis that COPD may influence LV structure. Patients known with COPD experience hyperinflation, an increase of intrathoracic pressure and a decrease of intrathoracic volume. In this cascade of events, the pulmonary vascular pressure will increase. All this will decrease the left ventricular end diastolic diameter and a reduction in preload. In this process, patients might develop a ‘microcor’, possibly resulting in chronic inflammation and pronounced activation of the renin–angiotensin–aldosterone system,22 which may result in paradoxical LVH. This study confirms these results, yet the order of this cascade is not certain. After all, not all patients with COPD but only the patients with severe emphysema develop a microcor.23 In addition, decreased preload was found to reduce the chance to develop LVH.24 Given the fact that only very few patients of the HF population of this study had severe COPD, it is much more likely that changes of the heart and its function may have influenced lung function abnormalities.
Equal DLCO in all HF groups
The present study found similar limitation in DLCO in the three HF groups. Previous research noticed a lower DLCO in patients with HF compared with healthy subjects.25 Thus, HF may play an important role, among other factors, in the reduction of DLCO. In patients with HF performing exercise, pulmonary capillary hydrostatic pressure may increase, lymphatic fluid removal can decrease and a reduction of active transport through sodium channels might develop. In this manner, pulmonary fluid overload is produced and the conductance of the alveolar capillary membrane may decrease. If the decrease in alveolar membrane conductance is greater than the increase in pulmonary capillary blood volume, DLCO decreases.26 The latter occurs if the pulmonary capillary blood flow decreases, for example, during the pathogenesis of pulmonary hypertension.27 Thus, a consequence of HF can be a decreased gas exchange at rest and a lower increase during exercise as compared with healthy subjects.28 Interestingly, diffusion capacity was impaired in 55% of the patients independently of the LVEF and showed a correlation with RV function, suggesting that such alterations may be present even in stable HF patients without evidence of congestion. Importantly, AL influenced diffusion capacity as expected, but it was also significantly reduced in HF patients without AL, independently of the LVEF. The significant though relatively weak correlation of DLCO with NT-proBNP as a measure of severity of HF further supports a direct influence of HF on gas exchange. Although these findings require confirmation in a larger cohort, they may be clinically meaningful as they might explain some physical limitation in patients with HF and can be of prognostic significance.10 29 30 In addition, the influence of HF treatment should be investigated in this regard.
Obviously, HF is not the only factor influencing DLCO. Among the less well-known factors, male gender and increased BMI may influence DLCO.31–33 The influence of gender may be explained by the higher prevalence of smoking in men compared with women. The findings of the correlation higher BMI for a lower DLCO has been discussed in a previous study that found an alveolar enlargement and a decrease of ratio alveolar surface area-to-lung volume in obese rats.32
A comparable RV function in the three HF groups
A comparable RV function (i.e., TAPSE/PASP) was found in the three HF groups. The equal distribution of patients with COPD and pulmonary hypertension in all groups may have contributed to this, but this influence seems to be limited. This is in line with previous research that found similar RV function (i.e., TAPSE) in patients with non-severe COPD compared with healthy patients.3 Thus, LV failure in addition to the underlying cardiac pathology possibly affecting both ventricles is a much more important cause of RV failure due to first passive increase in pulmonary pressure, which may further result in an increase in pulmonary vascular resistance in some patients.34 The findings of the present study of correlations of TAPSE/PASP with NT-proBNP and pulmonary pressure supports this notion. The correlation between reduced systolic function of the LV and the RV may vary depending on the population included and needs to be better studied to determine the precise underlying cause of RV dysfunction in patients with HF. This may include invasive measurements to better define these different factors potentially influencing the RV. The well-known association between RV dysfunction and poor outcome supports this need.11 Our results suggest that this need is not dependent on LVEF.
Study strength and limitations
The strengths of this study are the comprehensive patient characterisation regarding comorbidities, cause of HF, symptoms, lung function abnormalities and echocardiography. It is based on a representative group of stable, chronic HF patients subdivided according to the most recent ESC guidelines using a uniformed cut-off regarding LVEF. The measurements of pulmonary function and echocardiography occurred systematically according to state-of-the-art practice. Accordingly, the determination of HF and functional limitations of the lungs are accurate.
The main limitations are the relatively limited sample size, the single-centre setting, missing items for some of the variables and lack of invasive measurements and histological data. Therefore, it is possible that some differences between the three groups based on LVEF may become significant in a larger population. Still, the clinical consequences that lung function testing should be considered in all patients irrespectively of LVEF would not change. NT-proBNP values were measured in only 123 patients because this was not compulsory per protocol, and only values from study visits were used. Similarly, E/e′ was not obtained in all patients as we used clinically indicated echocardiograms if done within 6 months, and these values were available in all. Systolic pulmonary pressure was only obtained if clear signal of tricuspid regurgitation was available, which was not the case in all patients. Still, patients without these measurements did not differ from the others (data not shown), which makes it rather unlikely that these missing data influenced the outcome of our study significantly. Given the stable situation and the fact that patients were well compensated, NT-proBNP and E/e′ levels were on average relatively low and results might differ in patients with more advanced HF. Because of the lack of invasive measurements, it is impossible to precisely explore the pathophysiology of lung function abnormalities, pulmonary vascular disease, pulmonary hypertension and diagnosis of RV dysfunction.
Based on the power of this small study population and the amount of missing variables, no multivariable regression analysis was performed on this study population to investigate other predisposing factors for cardiopulmonary abnormalities. Future research on a large scale can be interesting to investigate these factors and potential causal links between them. Finally, we did not investigate any influence of treatment of HF on pulmonary abnormalities and vice versa. Such intervention studies may help to improve treatment of such patients and may improve understanding of pathophysiological interaction between heart and lungs.
Conclusions
Pulmonary function in terms of both diffusion capacity and airway limitation was reduced in a significant proportion of patients in this stable outpatient HF population, with no differences between HFpEF, HFmrEF and HFrEF. The reduction of diffusion capacity was even seen in a substantial proportion of patients who did not have airway limitations. Also, RV function was similarly affected in all three groups. The findings of this study underline the importance of identifying lung function abnormalities in stable patients with HF independently of the type of HF.
Key messages
What is already known about this subject?
The link between heart failure (HF) and pulmonary abnormalities is already known. The relationship between the right ventricular function and pulmonary abnormalities is less clear. This relationship is not yet investigated in the three recent defined groups of HF (HF with reduced ejection fraction, HF with midrange ejection fraction (HFmrEF) and HF with preserved ejection fraction).
What does this study add?
Using a stable group of patients with HF, a measurement of gas exchange in the lungs and the most accurate echocardiographic technique to estimate right ventricular function (eg, tricuspid annular plane systolic excursion/pulmonary artery systolic pressure), this study demonstrates accurate and state-of-the-art information concerning the lungs and heart of the involved patients.
Another new element in this study is that lung abnormalities and right ventricular function are not influenced by left ventricular ejection fraction (LVEF). Thus, the pulmonary abnormalities and their frequencies are equal in the three groups.
How might this impact on clinical practice?
This study emphasises the importance to perform extra investigation of the lungs in stable patients with HF independently of the LVEF. This is also applicable in the newly proposed and less investigated group of HFmrEF.
References
Footnotes
Contributors H-PB-LR, CK, VvE, SB and WR planned this research by inventing the research question. H-PB-LR and SB planned this research by making the set-up of this study. H-PB-LR, CK, VvE, JB, NU-L conducted this research by giving critical revisions. H-PB-LR, SB and WR reported the research by writing the manuscript. H-PB-LR and WR made the figures. WR submitted the research. H-PB-LR is the guarantor.
Funding This study was funded by GlaxoSmithKline Pharma.
Competing interests We report grants from GSK-Pharma during the conduct of this study.
Patient consent Obtained.
Ethics approval The local medical ethics committee approved this study (METC 12-2-005 (NL39223.068.12)).
Provenance and peer review Not commissioned; externally peer reviewed.