
Abstract
Rheumatic heart disease, a neglected disease, continues to be a burden in India and other developing countries. It is a result of an autoimmune sequalae in response to group A beta hemolytic streptococcus (GAS) infection of the pharynx. Acute rheumatic fever (RF), a multisystem inflammatory disease, is followed by rheumatic heart disease (RHD) and has manifestations of joints, skin and central nervous system involvement. A review of epidemiological studies indicates unchanged GAS pharyngitis and carrier rates in India. The apparent decline in RHD rates in India as indicated by the epidemiological studies has to be taken with caution as methodological differences exist among studies. Use of echocardiography increases case detection rates of RHD in population surveys. However, the significance of echo based diagnosis of carditis needs further evaluation to establish the significance. Research in this area through prospective follow up studies will have to be undertaken by the developing countries as the interest of developed countries in the disease has waned due the declined burden in their populations. Prevention of RHD is possible through treatment of GAS pharyngitis (primary prophylaxis) and continued antibiotic treatment for number of years in patients with history of RF to prevent recurrences (secondary prophylaxis). The cost effectiveness and practicality of secondary prophylaxis is well documented. The challenge to any secondary prophylaxis program for prevention of RF in India will be the availability of benzathine penicillin G and dissipation of fears of allergic reactions to penicillin among practitioners, general public and policy makers. The authors review here the progress and challenges in epidemiology, diagnosis and primary and secondary prevention of RF and RHD.
Similar content being viewed by others


Introduction
Acute rheumatic fever (RF), rheumatic heart disease (RHD) and post-streptococcal glomerulonephritis (PSGN) are nonsuppurative sequelae of Streptococcus pyogenes or group A beta hemolytic streptococcus (GAS) infections. The bacterial pathogen is responsible for a wide variety of diseases ranging from noninvasive mild infections like pharyngitis, and impetigo to invasive, life threatening conditions like bacteremia, pneumonia, necrotizing fasciitis and streptococcal toxic shock syndrome (STSS). The organism spreads rapidly through droplets and contact from one person to another. The predominant M type strain of GAS changes continuously.
The GAS serotyping scheme developed by Lancefield in 1928 is based on antiphagocytic M protein encoded by emm gene [1]. There are 83 GAS M serotypes and many of the GAS isolates are non-M serotypable [2]. Currently, emm typing is done to identify the GAS serotype by a PCR based sequencing method which identifies the N terminal variable region of the M protein. The CDC website currently lists more than 200 GAS emm types. Studies from India have also reported a high degree of heterogeneity in the emm types of GAS strains [3–9].
GAS Pharyngitis and Impetigo: Relationship with RF and RHD
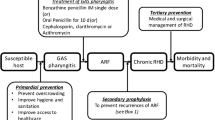
Though majority of the pharyngitis are viral infections, around 26% of pharyngitis is estimated to be due to infection with GAS [10]. It occurs predominantly in the winter season [6, 11]. Incidence of GAS pharyngitis ranges from 2.8 to 13.7 per cent in India as compared to 9 to 34.1 per cent in other parts of the world [6, 11]. The primary concern for GAS pharyngitis in the pediatric population is due to RF in 3% of cases during epidemics and 0.3% in endemic situations [12, 13]. RF is a multisystem autoimmune inflammatory disorder and primarily involves heart, joints, skin and central nervous system. However, heart is the only organ which suffers permanent damage. The clinical manifestations of RF include polyarthritis, carditis, chorea, erythema marginatum and subcutaneous nodules. The occurrence of carditis in first or recurrent episodes of RF can lead to RHD in 50% of RF patients. The risk of RF is negatively correlated with age and number of years since the last attack [14]. It increases with the number of previous attacks and the presence of pre-existing RHD [14]. Though appropriate antibiotic treatment can prevent RF, a clinician’s dilemma is that one third of GAS infection is not evident [15]. GAS carriage rates have been shown to range from 1.3 to 20% in school-age children in India [5, 6, 16, 17].
GAS impetigo is known to be prevalent at much higher rates in developing countries than in developed countries [10, 18]. It is uncommon in North India [6] but is more common (6.9 per 100 children) in the tropical climate of South India and in the aboriginal communities of northern territories of Australia [19]. As the aboriginal communities of Australia have one of the highest prevalence rates of RHD with low incidence rates of GAS pharyngitis, a role of GAS impetigo in the pathogenesis of RHD has been hypothesized [20, 21]. However, well structured research is required to confirm this hypothesis.
RF and RHD Epidemiology
Epidemiology of RF and RHD is radically different between developed and developing countries. The socioeconomic and environmental factors are known to play an important part in contributing to the magnitude and severity of RF and RHD. In developed countries, the peak incidence of RF is in the 5 to 15 y age group, being rare below the age of 5 [22]. On the other hand, in developing countries the age at presentation for rheumatic mitral stenosis has been reported to be below 12 and in 20% below 20 y [23]. Though, clinical features of RF are similar in different parts of the world, presentation of RHD in developed and developing countries was reported to be different initially by two studies published in 1960s from India [24, 25] and then by a study comparing the characteristics of patients with mitral stenosis from five non-Western and two Western countries [26]. Onset of symptomatic RHD with mitral stenosis occurred within a short interval of symptom following RF in individuals younger than 20 y. Mitral valve calcification, atrial fibrillation and thromboembolic complications were infrequent among patients below 20 y. Further, an early development (under 5 y) of established RHD and its rapid progression to disabling cardiac involvement, termed as “Juvenile Mitral Stenosis”, poses a major problem in India. Similarly, a study from Saudi Arabia reported 43% mitral stenosis in patients aged 20 y or less in 1981 [27], but the rates declined with improved socio-economic status and healthcare by 2001[28]. To update the findings of 1960s study, systematic studies in RF are required in India.
The incidence of RF has declined in the high-income countries since 1950s, which now have an annual incidence of around 0.5 cases per 100,000 children of school age compared to 100 to 200 cases per 100,000 in low income countries [29]. Reduction in the incidence of RF is mainly attributable to improvements in living conditions leading to less crowding resulting in lower rates of transmission of GAS. Carapetis et al [11] in 2005 suggested that the prevalence of severe GAS disease (acute RF, RHD, post-streptococcal glomerulonephritis, and invasive infections) was present in at least 18·1 million cases with 1·78 million new cases added each year. The severe GAS disease results in at least 517, 000 deaths each year. Major burden of the GAS diseases was due to RHD which accounted for about 15.6 million people worldwide with 282, 000 new cases annually and 233,000 deaths each year. The highest rates of RF and RHD in the world are among Australia’s Aboriginal and Torres Strait Islander peoples living in remote areas [11]. However, the absolute numbers of people afflicted with RHD in this review were derived from very few studies from Asia. Subsequently studies conducted between 2003 to 2007 in Asian countries were included [30]. It was estimated that about 1.96 to 2.21 million cases of RHD are prevalent in the age group of 5 to 14 y and 10.8 to 15.9 million cases exist in all ages in Asia.
Studies from India from 1988 to 2005 observed marked heterogeneity in prevalence of RHD ranging from 0.67 to 6.4 per 1000 [31–41]. Most of these epidemiological studies were school based cross sectional surveys carried out in different geographical locations of the country with varying methodologies making it difficult to understand the changes in trends of disease burden. Since 1970, ICMR has conducted three large multi centric studies (Year 1972–1975; 1982–1990 and; 2000–2010) among school children in the age group of 5 to 14 y using common methodologies across centres. The first two studies used auscultatory clinical findings of murmurs for the diagnosis of RHD [42]. The study between 1972 to 1975 included schools at Agra, Allepy, Bombay, Delhi and Hyderabad (n = 1,33,000), whereas that between 1984 to 1987 included population at Delhi, Varanasi and Vellore (total population covered = 2,17,000 with 53,986 children in age group of 5 to 14 y studied). The prevalence rate of RHD observed in these studies at different places in India is shown in Fig 1 and range from 0.8/1000 to 11/1000 in 1970s to 1.0/1000 to 5.6/1000 in 1980s [42]. A steep decline was observed in RHD prevalence in Delhi within a decade by these two studies [42]. In other study centres, the average reported prevalence of RHD based on these two surveys was 3.4/1000 (1972–1975) and 4.2/1000 (1984–1987), indicating insignificant change in epidemiology of RHD from 1970’s to 80’s.

Prevalence /1000 of RHD in school children in age group of 5 to 14 y in ICMR studies conducted in 1970s and 1980s
In 1991, India embarked on economic reform process and by 2000, the country witnessed higher economic growth rates and increase in life expectancy and urbanization. The increase in life expectancy along with changes in the lifestyles has led to an increase in non communicable diseases in the country along with yet unfinished agenda of communicable diseases. In such a changed scenario, it was considered important from policy point of view to revisit RHD in different states of India so as to access whether public health system needs to be toned up to reduce the burden of one of the preventable cardiac disease of the pediatric population. ICMR’s multicentric ‘Jai Vigyan Mission Mode Project on RF/RHD’ was undertaken from 2000 to 2010 to estimate the prevalence of RF/RHD in 176904 school children in the age group of 5 to 14 y at Roopnagar (Punjab), Shimla (Himachal Pradesh), Jammu (Jammu and Kashmir), Jodhpur (Rajasthan), Mumbai (Maharashtra), Indore (Madhya Pradesh), Vellore (Tamil Nadu), Kochi (Kerala), Wayanad (Kerala) and Dibrugarh (Assam) [43]. It is the largest study on RF/RHD from India. Primary screening to identify abnormal heart sounds and murmurs was performed by auscultation by a trained medical officer in the school children in the age group of 5–14 y. Children with abnormal heart sounds or murmurs during the primary screening were referred to a tertiary care hospital for confirmation of the diagnosis using echocardiography. The prevalence of RHD in this multicentric school study ranged from 0.13 to 1.5 per 1000 in school children in the age group 5 to 9 y and 0.13 to 1.1 per 1000 in the age group of 10 to 14 y. The extrapolation of incidence of RF and prevalence of RHD observed in this multicentric ICMR study to the entire country has to be undertaken with utmost caution, as it might not have been possible to register all cases from the defined population through active surveillance using clinical examination of school children for initial screening followed by echocardiography in suspected cases and passive surveillance (RHD population registry data). Moreover this study does not have data from some underdeveloped areas of India. There is a likelihood of a higher burden of RF/RHD than estimated, as pockets with lower development of healthcare infrastructure exist in many states. Further, the apparent decline in RHD prevalence in this study (2000–2010) from the earlier ICMR studies conducted in 1970s and 80s may be an artefact arising from methodological differences used for diagnosis of RHD. Preliminary comparison of prevalence rates of RHD based on auscultatory clinical findings of murmurs in the two surveys conducted between 1984–87 and 2000–2010 did not indicate decline of RHD in Vellore, a centre which participated in both the surveys. The study concluded that RF/RHD still appears to be a problem of public health significance.
Use of Echocardiography for Detection of RHD Cases in Population Surveys
The estimation of true burden of RHD in the community is challenging because RHD can be asymptomatic [44], which is only detected either incidentally during a medical examination or when the person becomes symptomatic. There is absence of periodic medical checkups as well as life insurance for a very large population in India. Therefore, development of an affordable, highly sensitive and specific screening technique, capable of detecting asymptomatic cases is required for the estimation of true disease burden [45]. Though auscultatory screening by specially trained community health workers followed by echocardiography of suspected cases is cost effective, the clinical evaluation to diagnose heart valve lesions even by an experienced cardiologist has been documented to be inaccurate [46].
Onsite portable echocardiography is considered to be highly sensitive for detection of heart valve lesions [44, 46]. However, specialized skills required and the high cost of the equipment hampers its use for multicentric population based surveillance [47]. Using echocardiographic diagnostic criteria, prevalence rates of 62/1000 in Kenya, 21.5 per 1,000 in Cambodia, 30.4 per 1,000 in Mozambique, 48/1000 in Nicaragua, 51 per 1000 in Bikaner (India) and 20.4 per 1000 in Ballabgarh(India) have been reported in school going children [47–51]. The variation in case detection rates (10 to 55 times) by echocardiograhic vs. clinical criterion alone in different studies may be due to non-availability of standardized echocardiographic criteria. The WHO criteria [52] for echocardiography Doppler detection of subclinical RHD demonstrated the importance of criteria consideration on the number of detected cases. Minor changes in echo criteria may have a great impact on the number of detected RHD cases. Nature Review Cardiology has recently published World Heart Federation’s (WHF) echocardiographic criteria for RHD aimed to permit rapid detection of patients with subclinical RHD and placing them on secondary penicillin prophylaxis [53]. Table 1 compares the WHO and WHF’s criteria for echocardiography for RHD. Though WHF criteria provide a uniform methodology for rapid identification of individuals with RHD in the absence of a clear-cut history of acute RF, implementation of these guidelines in clinical practise requires skilled practitioners [54]. The paucity of skilled practitioners within the existing healthcare set up in a developing country may limit the implementation of these guidelines, especially in population surveys. This highlights the urgent need for development and evaluation of simple strategies for echocardiography based diagnosis of RHD cases. Mirabel et al [54] showed a sensitivity of 73% for RHD case detection in children and a positive predictive value of 92% for a simplified echocardiographic criteria (single mitral regurgitation jet-length criterion) as compared to a reference criteria based on combination of Doppler and morphological features of rheumatic mitral and aortic valves. Further, the high echocardiographic prevalence of RHD reported from Kenya, Cambodia, Mozambique and India is difficult to accept clinically. If correct, between 10 to 20/ 1000 adults around the age of 30 to 40 y should have RHD in these countries. It is possible that echocardiographic prevalence rates of RHD may either be grossly wrong or extremely large number of deaths due to RHD occur in <20 y age group for which there are no documentary evidences.
Further, one third of RHD cases put on penicillin prophylaxis reverted to normal in Bikaner (India) and Nicaragua [44, 55]. Even in the absence of penicillin prophylaxis, no progression of majority of subclinical RHD lesions from Ballabgarh (India) was observed after a relatively short follow up [51]. These studies indicate the need to investigate the natural course of subclinical RHD lesions and eventual clinical outcomes through large prospective studies in different regions of the world.
Preventing RF
As GAS infection of pharynx is primarily responsible for rheumatic fever, prevention of initial episode of acute rheumatic fever (ARF) requires proper diagnosis and treatment of GAS pharyngitis.
Diagnosis of GAS Pharyngitis
Differential diagnosis of GAS pharyngitis from other bacterial and viral pharyngitis is difficult as none of the clinical findings is specific for GAS pharyngitis. As per AHA statement [56] and Indian consensus guidelines [57] on RF, clinical findings suggestive of GAS pharyngitis are sudden onset of sore throat, pain on swallowing and fever of varying degree (usually from 101°F to 102°F) with headache; abdominal pain, nausea, and vomiting also occur in children. Additional clinical findings like beefy swollen, red uvula, scarlet fever rash, soft palate petechiae, tonsillopharyngeal erythema with and without exudates and tender, enlarged anterior cervical nodes may also be considered [56]. AHA statement recommends that epidemiological findings like 5–15 y age group, history of exposure to GAS pharyngitis, high prevalence of GAS infection in the community and the winter and spring seasons of the year needs to be considered [56]. As accurate clinical diagnosis of GAS pharyngitis is difficult from pharyngitis of different origins, a throat culture or rapid antigen detection test (RADT) are recommended [56–58], which however does not differentiate between GAS pharyngitis and carrier state. A selective use of culture and RADT in cases where clinical and epidemiological findings suggest GAS pharyngitis allows differentiation between a GAS pharyngitis and carrier state [53], thereby limiting antibiotic usage. Additional laboratory tests include antistreptolysin O (ASO), antideoxyribonuclease B, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and complete blood counts [56, 57] .
Diagnostic Criteria for RF
The guidelines for diagnosis of ARF first described by Jones [59] in 1944 divide the clinical features into major and minor manifestations. The major manifestations were carditis, joint symptoms, subcutaneous nodules, and chorea. Since then the guidelines have gone through several revisions with the latest statement in 1992, largely in response to the decreasing incidence of RF in USA [60]. The American Heart Association (AHA) in its Jones Criteria workshop in 2000 [60], WHO 2004 guidelines [44] and 2008 Consensus Indian Guidelines [57] reaffirmed the adequacy of the 1992 ‘Jone’s Criteria Updated’. AHA guidelines [61] recognized that strict adherence to the Jones criteria in endemic regions may result in under-diagnosis which would hamper the treatment of patients with recurrent episodes of RF. Further, monoarticular arthiritis and echocardiographic evaluation for management of RHD may be considered in endemic parts of the world. Significantly, National Heart Foundation of Australia (NHFA) and the Cardiac Society of Australia and New Zealand (CSANZ) review uses subclinical evidence of RHD on echocardiography and mono-arthritis to increase the sensitivity for identification of cases in high risk groups (with ARF incidence rate of >30 per 100,000 per year in 5–14 y old and RHD prevalence rate of 2 per 1000 in all age groups) [62]. The guidelines issued by various agencies since 1992 update of Jone’s criteria are compared in Table 2. It is evident that the Indian Guidelines [57] did not take epidemiological settings into consideration, nor was use of echocardiography for detection of subclinical carditis advocated. At this juncture, it appears that echocardiography may be helpful in placing this neglected disease in nation’s health agenda but whether such patients should be put on secondary penicillin prophylaxis to prevent recurrence of RF is debatable [63, 64]. Only large prospective studies on a cohort of subclinical carditis with and without benzathine penicillin prophylaxis may provide clues to this paradox.
Prevention of RF: Primary and Secondary Prevention
The primary prevention of RF involves treatment of GAS infections whereas the secondary prevention of RF is to prevent colonization of pharynx with GAS and recurrent attacks of RF. Antibiotics are administered continuously to patients with a previous attack of RF or documented evidence of RHD [56, 57]. Penicillin is the drug of choice as in spite of its usage for more than 60 y, GAS resistant to this antibiotic has never been documented [65]. There are number of guidelines for the management of RF and RHD including 2004 WHO Guidelines [44], 2008 Consensus Indian Guidelines [57], 2006 NHFA and CSANZ Review [62] and 2009 AHA statement on RF [56]. Table 3 compares these guidelines. The guidelines mainly vary as to the weight at which the dose of benzathine benzylpenicillin dose is increased, which further depends on the prevalence rates of disease in the population. The selection of the treatment regime is based on its ease of adherence to the recommended regimen (frequency of daily administration, duration of therapy, and palatability), bacteriologic and clinical efficacy, spectrum of activity of the selected agent and potential side effects and the cost.
Challenges in Primary Prevention of RHD
The cost effectiveness of penicillin prophylaxis as primary and secondary prevention tools vs. the surgical interventions required for surgical valve management in RHD has been documented in developing countries. In a low socio-economic population of Brazil, the direct, indirect, and total costs to society per 100 patients throughout the entire disease duration has been estimated to be US$ 271/patient/year, US $48/patient/year and US $319/patient/year respectively [66]. In India, the direct, indirect, and total costs for primary, secondary and tertiary prevention of RF/RHD have been calculated in the 5 to 15 y population (n = 178,069) of Pondicherry (Census 2001; total population 974,345) [67]. As the disease of non-affluent sections of society is expected to be largely catered by government hospitals in India, therefore, the costs used for treatment/procedure are based on the rates in government setup of JIPMER, Pondicherry. The study estimated that the total cost (including direct and indirect costs) of primary prevention of RF/RHD required for Pondicherry (12,55,386 episodes of sore throat at 7.05 per child year or 1,69,166 total episodes of sore throat due to GAS) will be 190 million rupees/year (1 million rupees = 20,000 US$) vs 160 million rupees/year for secondary prevention and tertiary management of 1068 RHD cases will require 280 million rupees/year in Pondicherry alone. The cost of operation alone on an average is around Rs 60,500 per procedure [67] and poses a financial burden to the family. This was also shown by the ICMR study “Jai Vigyan Mission Mode project on RF/ RHD”; financial constraints was cited as the cause for not undertaking cardiac intervention in 57% and 63.6% of RHD cases in Chandigarh and Vellore (unpublished) in which cardiac intervention was required. Thus, it is important to undertake primary/secondary prevention and control measures at population level for reducing the burden of RF/RHD.
Though primary prevention of RF/RHDs through penicillin prophylaxis theoretically sounds good, it is actually difficult to undertake [68] due to:
-
(i)
Difficulties in differential diagnosis of GAS pharyngitis from other pharyngitis based on history and clinical findings
-
(ii)
Requirement of laboratory infrastructure and trained manpower for identification of GAS sore throats through culture
-
(iii)
Requirement of large number of GAS pharyngitis sore throats to be treated for preventing RF though only 0.3% to 3% of the GAS pharyngitis convert to rheumatic fever
-
(iv)
Concerns regarding widespread usage of antibiotic for treatment of GAS sore throats may actually provide an environment for selective pressure for new antimicrobial resistance to develop.
Despite these drawbacks, primary prevention of RF was successfully implemented in Costa Rica and Cuba by using: clinical algorithms which eliminated the need for throat swab cultures for confirmation of GAS pharyngitis; single intramuscular injection of benzathine penicillin in clinically diagnosed cases of GAS sore throat and; advocacy for the need for prevention of GAS pharyngitis in community [68]. Though, it will be important to replicate this model in India, methodologies will have to be tailored to the local needs including methods addressing considerably large number of asymptomatic GAS carriers (1.3 to 20%) among school-age children in the country [5, 6, 16, 17].
Secondary Prophylaxis for Prevention of RF in Developing Countries
Keeping the limitation of primary prophylaxis in view, it is evident that an anti-streptococcal vaccine can be a potent tool for primary prevention of RF. Given the marked heterogeneity in GAS strains circulating in India [3–9], as mentioned earlier, the development of M protein N terminal based vaccine specific to the settings of a developing country like India is going to be extremely challenging. Efforts for vaccine development based on non M protein antigens including carbohydrates, C5a peptidase and fibronectin binding protein are underway globally. Discussion on different strategies being used worldwide for development of vaccine against GAS [69, 70] is beyond the scope of current review. As development of a country specific vaccine against GAS remains a distant possibility, concerted efforts need to be made towards other effective public health prevention and control measures.
Secondary prophylaxis involving administration of benzathine penicillin G injections every 2 to 3 wk for years together in patients with history of RF to prevent recurrent episodes, through RF RHD registries, is cost effective and practical in developing countries like India. Such a RF RHD registry based program will require a continuous supply of benzathine penicillin in all Indian States. In the ICMR study, the Centres faced difficulty in providing benzathine penicillin to RF/RHD patients due to shortage of this drug in the market. Further, some states like Tamil Nadu have prohibited use of injectable penicillin and only oral penicillin is available. The shortage in supplies of benzathine penicillin and fear of allergic reaction to benzathine penicillin contribute towards inadequate treatment of RF patients. As compliance to benzathine penicillin is of utmost importance in secondary prevention of RF an advocacy of the following facts among physicians, general public and policy makers may be helpful in decreasing the fear of allergic reactions:
-
i.
Allergic reaction to penicillin is rare in children [55, 71] and occurs only in a small percentage of individuals.
-
ii.
Allergic reactions can be circumvented by obtaining careful history regarding allergic reaction to penicillin and administration of the injection by medical practitioner only.
Management of this disease in ‘National Program for Prevention and Control of Cancer, Diabetes, CVD and Stroke’ in India will go a long way in reduction of this preventable cardiac disease of the pediatric population.
In conclusion, RHD remains a disease of public health concern. The role of echocardiography in diagnosis of RHD in patients without clinical symptoms of carditis needs to be investigated to understand the course of subclinical valvular regurgitation and the pathology of RF. Also, given the resource constrained settings of a developing country like India, there is an urgent need for development and evaluation of simple strategies for echocardiography based diagnosis of RHD cases for carrying out RHD surveillance in a school setting. Primary prophylaxis for treatment of GAS pharyngitis and secondary prophylaxis for RF prevention are available. The challenge will be to develop a model suitable to India for primary prophylaxis and establish nationwide registry program for administering secondary prophylaxis to prevent recurring RF episodes in India. Such a program will help in prevention of this preventable pediatric cardiac disease.
References
Lancefield RC. The antigenic complex of Streptococcus haemolyticus. I. Demonstration of a type-specific substance in extracts of Streptococcus haemolyticus. J Exp Med. 1928;47:91–103.
Facklam RF, Martin DR, Lovgren M, et al. Extension of the Lancefield classification for group A streptococci by addition of 22 new M protein gene sequence types from clinical isolates: emm103 to emm124. Clin Infect Dis. 2002;34:28–38.
Sharma M, Shah B, Dhaliwal RS. Heterogeneity of community based pediatric GAS isolates from India: Challenges to the multivalent vaccine approach. International Congress Series. 2006;1289:49–53.
Dey N, Mcmillan DJ, Yarwood PJ, et al. High diversity of group A streptococcal emm types in an Indian community: the need to tailor multivalent vaccines. Clin Infect Dis. 2005;40:46–51.
Lloyd CA, Jacob SE, Menon T. Pharyngeal carriage of group A streptococci in school children in Chennai. Indian J Med Res. 2006;124:195–8.
Kumar R, Vohra H, Chakraborty A, et al. Epidemiology of group A streptococcal pharyngitis & impetigo: a cross-sectional & follow up study in a rural community of northern India. Indian J Med Res. 2009;130:765–71.
Sagar V, Bakshi DK, Nandi S, Ganguly NK, Kumar R, Chakraborti A. Molecular heterogeneity among north Indian isolates of Group A streptococcus. Lett Appl Microbiol. 2004;39:84–8.
Menon T, Lloyd C, Malathy B, Sakota V, Jackson D, Beall B. 12.emm type diversity of beta - a hemolytic streptococci recovered in Chennai, India. J Med Microbiol. 2008;57:540–2.
Dhanda V, Kumar R, Thakur JS, Chakraborti A. emm type distribution pattern of group A streptococcus in north India: need for a new preventive approach. Indian J Med Res. 2010;132:741–4.
Smith TD, Wilkinson V, Kaplan EL. Group A streptococcus-associated upper respiratory tract infections in a day-care center. Pediatrics. 1989;83:380–4.
Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5:685–94.
Rammelkamp CH, Denny FW, Wannamaker LW. Studies on the epidemiology of rheumatic fever in the armed Services. In: Thomas L, ed. Rheumatic fever. Minneapolis: University of Minnesota Press; 1952. pp. 72–89.
Siegel AC, Johnson EE, Stollerman GH. Controlled studies of streptococcal pharyngitis in a pediatric population - Factors related to the attack rate of rheumatic fever. N Engl J Med. 1961;265:559–66.
Spagnuolo M, Pasternak B, Taranta A. Risk of rheumatic-fever recurrences after streptococcal infections. Prospective study of clinical and social factors. N Engl J Med. 1971;285:641–7.
Dajani AS. Current status of nonsuppurative complications of group A streptococci. Pediatr Infect Dis J. 1991;10:S25–27.
Rajkumar S, Krishnamurthy R. Isolation of group A β hemolytic streptococci in the tonsillopharynx of school children in Madras city and correlation with their clinical features. Jpn J Infect Dis. 2001;54:137–9.
Menon T, Shanmugasundaram S, Kumar MP, Kumar CP. Group a streptococcal infections of the pharynx in a rural population in south India. Indian J Med Res. 2004;119:171–3.
Smeesters PR, Vergison A, Campos D, de Aguiar E, Miendje Deyi VY, Van Melderen L. Differences between Belgian and Brazilian Group A Streptococcus Epidemiologic Landscape. PLoS ONE. 2006;1:e10.
McDonald MI, Towers RJ, Andrews RM, Benger N, Currie BJ, Carapetis JR. Low rates of streptococcal pharyngitis and high rates of pyoderma in Australian aboriginal communities where acute rheumatic fever is hyperendemic. Clin Infect Dis. 2006;43:683–9.
Carapetis JR, Currie BJ. Group A streptococcus, pyoderma, and rheumatic fever. Lancet. 1996;347:1271–2.
Parks T, Smeesters PR, Steer AC. Streptococcal skin infection and rheumatic heart disease. Curr Opin Infect Dis. 2012;25:145–53.
Bland EF, Jones TD. Rheumatic fever and rheumatic heart disease - A twenty year report on 1000 patients followed since childhood. Circulation. 1951;4:836–43.
Padmawati S. Rheumatic fever and rheumatic disease in development countries. Bull World Health Organization. 1978;56:543–50.
Roy SB, Bhatia ML, Lazaro EJ, Ramalingaswami V. Juvenile mitral stenosis in India. Lancet. 1963;2:1193–5.
Cherian G, Vytilingam KI, Sukumar IP, Gopinath N. Mitral valvotomy in young patients. Br Heart J. 1964;26:157–66.
Marijon E, Iung B, Mocumbi AO, et al. What are the differences in presentation of candidates for percutaneous mitral commissurotomy across the world and do they influence the results of the procedure? Arch Cardiovasc Dis. 2008;101:611–7.
Mardini MK. Rheumatic fever and its cardiac manifestations in children: an update. KFSH Med. 1981;1:131–9.
Andy JJ, Soomro RM. The changing incidence of juvenile mitral stenosis and natural history of rheumatic mitral valvulitis inAl Baha, Saudi Arabia. Ann Trop Paediatr. 2001;21:105–9.
Altamimi S, Khalil A, Khalaiwi KA, Milner R, Pusic MV, Al Othman MA. Short versus standard duration antibiotic therapy for acute streptococcal pharyngitis in children. Cochrane Database Syst Rev. 2009;1:CD004872.
Carapetis JR. Rheumatic heart disease in Asia. Circulation. 2008;118:2748–53.
Grover A, Dhawan A, Iyengar SD, Anand IS, Wahi PL, Ganguly NK. Epidemiology of rheumatic fever and rheumatic heart disease in a rural community in northern India. Bull World Health Organ. 1993;71:59–66.
Kumar P, Garhwal S, Chaudhary V. Rheumatic heart disease: a school survey in a rural area of Rajasthan. Indian Heart J. 1992;44:245–6.
Vashistha VM, Kalra A, Kalra K, Jain VK. Prevalence of rheumatic heart disease in school children. Indian Pediatr. 1993;30:53–6.
Patel DC, Patel NI, Patel JD, Patel SD. Rheumatic fever and rheumatic heart disease in school children of Anand. J Assoc Physicians India. 1986;34:837–9.
Avasthi G, Singh D, Singh C, Aggarwal SP, Bidwai PS, Avasthi R. Prevalence survey of rheumatic fever (RF) and rheumatic heart disease (RHD) in urban & rural school children in Ludhiana. Indian Heart J. 1987;39:26–8.
Agarwal AK, Yunus M, Ahmad J, Khan A. Rheumatic heart disease in India. J R Soc Health. 1995;115:303–4. 309.
Thakur JS, Negi PC, Ahluwalia SK, Vaidya NK. Epidemiological survey of rheumatic heart disease among school children in the Shimla Hills of northern India: prevalence and risk factors. J Epidemiol Community Health. 1996;50:62–7.
Thakur JS, Negi PC, Ahluwalia SK, Sharma R, Bhardwaj R. Congenital heart disease among school children in Shimla hills. Indian Heart J. 1995;47:232–5.
Gupta I, Gupta ML, Parihar A, Gupta CD. Epidemiology of rheumatic and congenital heart diseases in school children. J Indian Med Assoc. 1992;90:57–9.
Jose VJ, Gomathi M. Declining prevalence of rheumatic heart disease in rural schoolchildren in India: 2001–2002. Indian Heart J. 2003;55:158–60.
Periwal KL, Gupta BK, Panwar RB, Khatri PC, Raja S, Gupta R. Prevalence of rheumatic heart disease in school children in Bikaner: an echocardiographic study. J Assoc Physicians India. 2006;54:279–82.
Community control of rheumatic fever and rheumatic heart disease. Report of ICMR task force study. New Delhi: Indian Council of Medical Research; 1994.
Jai Vigyan Mission mode project on community control of RHD. Non-communicable diseases. Indian Council Med Res Annu Rep 2007–08; pp 63–4.
Rheumatic fever and rheumatic heart disease: report of a WHO Expert Consultation, Geneva, 29 October–1 November 2001. WHO Technical Report Series; 923. WHO. Geneva 2004. http://www.who.int/cardiovascular_diseases/resources/en/cvd_trs923.pdf (Accessed 3rd March 2012)
Carapetis JR, Hardy M, Fakakovikaetau T, et al. Evaluation of a screening protocol using auscultation and portable echocardiography to detect asymptomatic rheumatic heart disease in Tongan schoolchildren. Nat Clin Pract Cardiovasc Med. 2008;5:411–7.
Jaffe WM, Roche AH, Coverdale HA, McAlister HF, Ormiston JA, Greene ER. Clinical evaluation versus Doppler echocardiography in the quantitative assessment of valvular heart disease. Circulation. 1988;78:267–75.
Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiographic screening. N Engl J Med. 2007;357:470–6.
Anabwani GM, Bonhoeffer P. Prevalence of heart disease in school children in rural Kenya using colour-flow echocardiography. East Afr Med J. 1996;73:215–7.
Paar JA, Berrios NM, Rose JD, et al. Prevalence of rheumatic heart disease in children and young adults in Nicaragua. Am J Cardiol. 2010;105:1809–14.
Bhaya M, Panwar S, Beniwal R, Panwar RB. High prevalence of rheumatic heart disease detected by echocardiography in school children. Echocardiography. 2010;27:448–53.
Saxena A, Ramakrishnan S, Roy A, et al. Global burden of cardiovascular disease Prevalence and outcome of subclinical rheumatic heart disease in India: The RHEUMATIC (Rheumatic Heart Echo Utilisation and Monitoring Actuarial Trends in Indian Children) study. Heart. 2011;97:2018–22.
Marijon E, Celermajer DS, Tafflet M, et al. Rheumatic heart disease screening by echocardiography: the inadequacy of World Health Organization criteria for optimizing the diagnosis of subclinical disease. Circulation. 2009;120:663–8.
Reményi Bo, Wilson N, Steer A. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease— an evidence-based guideline. Nat Rev Cardiol. 2012;9:297–309.
Mirabel M, Celermajer DS, Ferreira B et al. Screening for rheumatic heart disease: evaluation of a simplified echocardiography-based approach. Eur Heart J Cardiovasc Imaging. 2012. http://ehjcimaging.oxfordjournals.org/content/early/2012/04/19/ehjci.jes077.abstract. (Accessed 5th June 2012)
Bhaya M, Beniwal R, Panwar S, Panwar RB. Two years of follow-up validates the echocardiographic criteria for the diagnosis and screening of rheumatic heart disease in asymptomatic populations. Echocardiography. 2011;28:929–33.
Gerber MA, Baltimore RS, Eaton CB, et al. Prevention of rheumatic fever and diagnosis and treatment of acute streptococcal pharyngitis: A scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: Endorsed by the American Academy of Pediatrics. Circulation. 2009;119:1541–51.
Working Group on Pediatric Acute Rheumatic Fever and Cardiology Chapter of Indian Academy of Pediatrics, Saxena A, Kumar RK, Gera RP, Radhakrishnan S, Mishra S, Ahmed Z. Consensus guidelines on pediatric acute rheumatic fever and rheumatic heart disease. Indian Pediatr. 2008;45:565–73.
Bisno AL, Gerber MA, Gwaltney Jr JM. Kaplan EL, Schwartz RH. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2002;35:113–25.
Jones TD. The diagnosis of rheumatic fever. JAMA. 1944;126:481–4.
Dajani AS, Ayoub E, Bierman FZ, et al. Guidelines for the diagnosis of rheumatic fever: Jones criteria, updated 1992. Circulation. 1993;87:302–7.
Ferrieri P, for the Jones Criteria Working Group. AHA scientific statement proceedings of the Jones Criteria workshop. Circulation. 2002;106:2521–3.
National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand. Diagnosis and management of Acute Rheumatic fever and Rheumatic heart disease in Australia – An evidence based review. 2006. http://www.racgp.org.au/Content/NavigationMenu/ClinicalResources/RACGPGuidelines/DiagnosisandmanagementofacuterheumaticfeverandrheumaticheartdiseaseinAustralia/NHFA-CSANZ_ARF_RHD_2006.pdf Accessed on 2nd March 2012.
Marijon E, Ou P, Celermajer DS, et al. Echocardiographic screening for rheumatic heart disease. Bull World Health Organ. 2008;86:84.
Marijon E, Celermajer DS, Jouven X. Management of patients with subclinical rheumatic heart disease. Int J Cardiol. 2009;134:295–6.
Horn DL, Zabriskie JB, Austrian R, et al. Why have group A streptococci remained susceptible to penicillin? Report on a symposium. Clin Infect Dis. 1998;26:1341–5.
Terreri MT, Ferraz MB, Goldenberg J, Len C, Hilário MO. Resource utilization and cost of rheumatic fever. The Journal of Rheumatology. 2001;28:1394–7.
Soudarssanane MB, Karthigeyan M, Mahalakshmy T, et al. Rheumatic fever and rheumatic heart disease: primary prevention is the cost effective option. Indian J Pediatr. 2007;74:567–70.
Karthikeyan G, Mayosi BM. Is primary prevention of rheumatic fever the missing link in the control of rheumatic heart disease in Africa? Circulation. 2009;120:709–13.
Marijon E, Mirabel M, Celermajer DS, Jouven X. Rheumatic heart disease. Lancet. 2012;379:953–64.
Steer AC, Batzloff MR, Mulholland K, Carapetis JR. Group A streptococcal vaccines: facts versus fantasy. Curr Opin Infect Dis. 2009;22:544–52.
International Rheumatic Fever Study Group. Allergic reactions to long-term benzathine penicillin prophylaxis for rheumatic fever. Lancet. 1991;337:1308–10.
Conflict of Interest
None.
Role of Funding Source
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shah, B., Sharma, M., Kumar, R. et al. Rheumatic Heart Disease: Progress and Challenges in India. Indian J Pediatr 80 (Suppl 1), 77–86 (2013). https://doi.org/10.1007/s12098-012-0853-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-012-0853-2