Article Text

Abstract
In China, poor cardioprotective medication adherence is a key reason for the high mortality rate of coronary heart disease (CHD). The aims of this systematic review are to (1) describe and synthesise factors that influence medication adherence among Chinese people with CHD, (2) evaluate the current status of intervention studies, and (3) discuss directions of future research to improve medication adherence. A comprehensive search using PubMed, Cumulative Index to Nursing and Allied Health Literature, Embase, Scopus, Global Health and PsycINFO was undertaken to describe poor adherence in China. Thirty-three eligible articles were included in the study. The review shows that there are multiple contributing factors to poor medication adherence, including patients’ sociodemographic characteristics, health status and medication characteristics. In addition, from patients’ perspective, lack of medication-related knowledge, such as the name, function, dosage and frequency, contributes to poor adherence. From physicians’ perspective, a gap exists between CHD secondary prevention guidelines and clinical practice in China. Follow-up phone calls, educational lectures, booklets and reminder cards were common methods found to be effective in improving medication adherence. This systematic review indicates that cardioprotective medications were commonly prescribed as secondary prevention medication to patients with CHD in China, but adherence to these medications gradually decreased during a follow-up period. Therefore, more research should be conducted on how to establish high-quality health educational programmes aimed at increasing patients’ medication adherence.
- medication adherence
- coronary heart disease
- china
Statistics from Altmetric.com
Introduction
Poor medication adherence among patients with coronary heart disease (CHD) is a global public health concern.1 This is particularly the case in China2 3 given the large size of patient population and the significant health disparities in access to care across its regions.4 CHD is the second leading cause of death in China,5 6 leading to over 1.5 million deaths each year.5 Cardioprotective medications, including antiplatelet drugs, beta-blockers, calcium channel blockers, statins and ACE inhibitors, are an essential treatment modality for CHD7 and can significantly reduce the mortality rate of this disease.3 8–12 However, poor adherence to cardioprotective medications is a public health threat in China.2 13 Many previous studies highlighted the importance of medication adherence in preventing cardiovascular diseases and the factors related to medication non-adherence, but none of them systematically summarised the factors among Chinese patients with CHD. Moreover, in China, there is a significant gap between factors found in the literature that related to medication non-adherence and interventions taken to tackle the problem in practice. Many previous studies investigated the factors that contributed to medication non-adherence, but did not propose specific interventions to improve medication adherence. A deeper understanding of the interplay of factors related to adherence to cardioprotective medications among the Chinese population is needed in order to develop interventions that will appropriately target this phenomenon.14 15 Therefore, the aims of this systematic review are to (1) describe and synthesise factors that influence medication adherence among Chinese people with CHD, (2) evaluate the current status of intervention studies, and (3) discuss directions of future research to improve medication adherence. The findings from this review may provide insights to address the issue of medication non-adherence globally.
Methods
Search strategy
We chose the databases PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Scopus, Global Health and PsycINFO as primary data sources for this review, as together they provide a comprehensive coverage of research in health-related disciplines. Two authors (ZN and LD) searched each database using keywords and algorithms that included the following: (coronary heart disease OR coronary artery disease), and (China OR Chinese), and (adherence OR compliance OR persistence OR discontinue OR underuse OR non-adherence OR non-compliance OR comply OR compliant OR adhere). An academic health centre reference librarian provided key assistance in building the combination of index and search terms that were applied to each database (table 1). No restrictions were applied on publication date. The first author (ZN), who is a native Chinese speaker, ran another search within a Chinese database, the China National Knowledge Infrastructure (CNKI), and used the Chinese keywords ‘yao wu yi cong xing’ (药物依从性) and ‘guan xin bing’ (冠心病), meaning medication adherence and coronary heart disease.
Search trial on PubMed, CINAHL, Embase, Scopus, Global Health and PsycINFO
Inclusion and exclusion criteria
We included articles that met the following criteria: (1) focus on adherence to at least one of the following cardioprotective medications: antiplatelet drugs, beta-blockers, calcium channel blockers, statins and ACE inhibitors/angiotensin receptor blocker; (2) Chinese samples with CHD living in China; and (3) peer-reviewed articles published in English or Chinese. Studies that included samples of Chinese patients living in Hong Kong, Taiwan and Macao were excluded, as these areas are historically dominated by foreign cultures, and thus their social structures and healthcare systems are different from that in mainland China.
Search outcomes
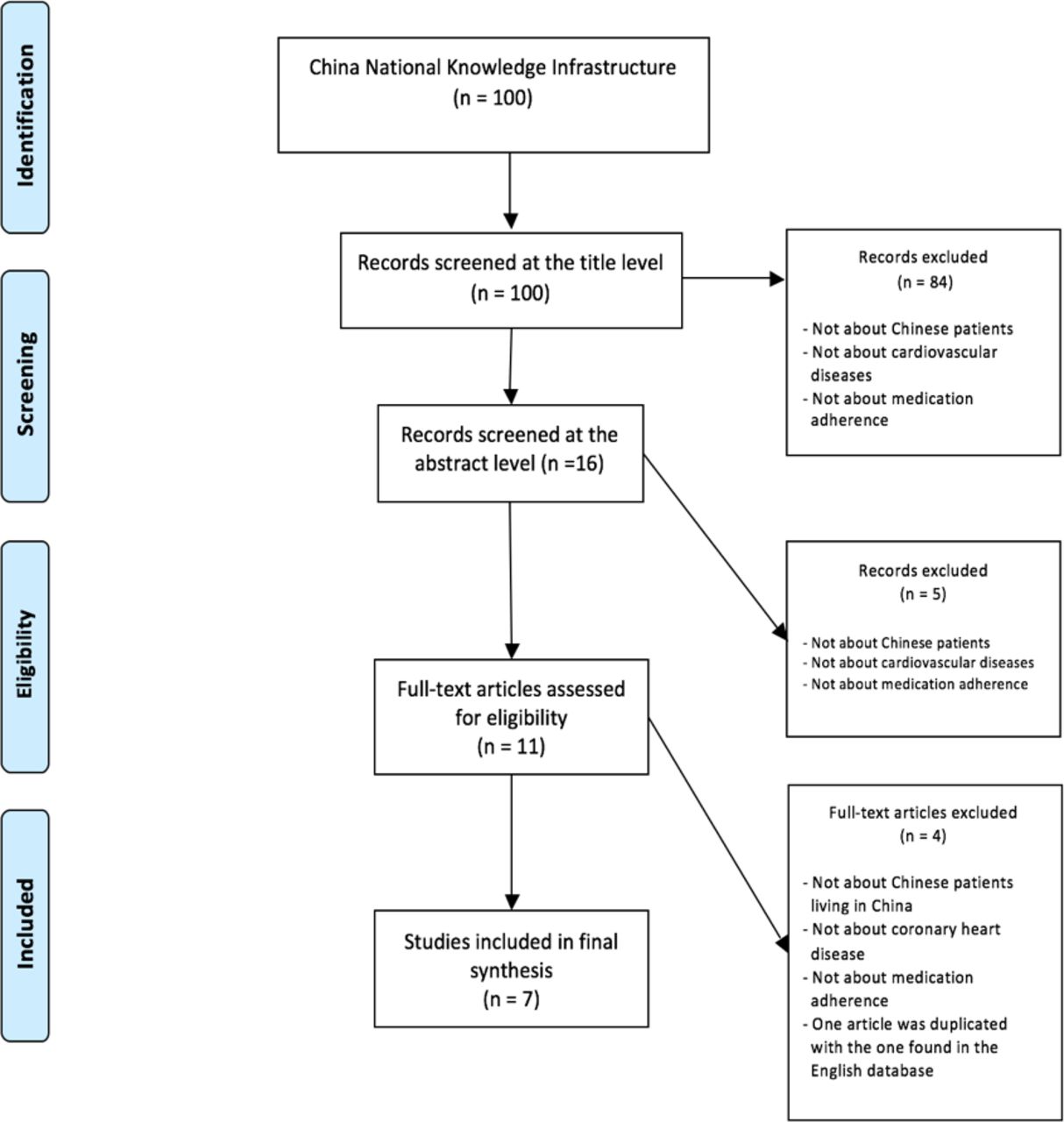
Our search resulted in the following: 173 articles from PubMed, 23 from CINAHL, 320 from Embase, 54 from Scopus, 56 from Global Health and 8 from PsycINFO. From the resulting 634 articles, 168 duplicates were removed, yielding 466 results. Afterwards, the first and the second authors (ZN and LD) screened the 466 titles independently and compared and discussed their results until agreement was reached, yielding 134 articles for subsequent abstract screening. After evaluating the abstracts of the 134 articles, 80 articles were excluded based on the preset inclusion criteria. The full texts of the remaining 54 articles were then examined and 26 articles met the full inclusion criteria (figure 1). The search of Chinese literature in CNKI yielded 100 related articles. After screening the titles, abstracts and full texts, seven articles were included (figure 2). Together, a total of 33 articles were used in this study. Later, we used a set of criteria to assess the quality of evidence provided by each of the included 33 studies. These criteria included study design, sample selection, measures, statistical analyses, reporting, content and utility (table 2).
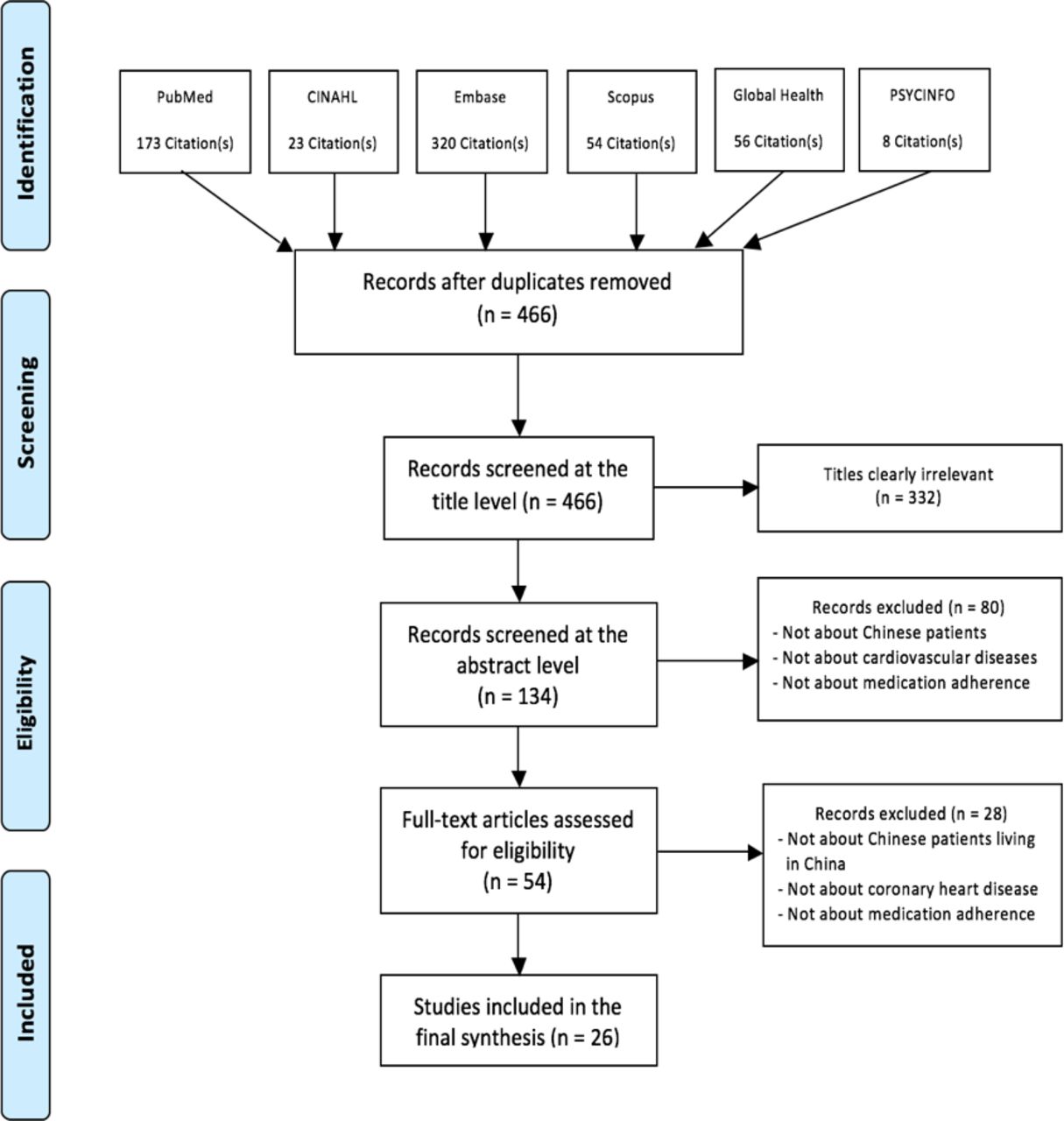
Literature review flow chart for English database. Adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram.50 CINAHL, Cumulative Index to Nursing and Allied Health Literature.
{kind=link}
{kind=link}
Literature review flow chart for Chinese database. Adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram.50
Quality appraisal of included studies
Findings
Study characteristics
The 33 articles included in this systematic review came from the medical, nursing and pharmacological disciplines. A range of study designs were employed from cross-sectional studies (n=22) and longitudinal studies (n=2), to randomised controlled trials (n=9) (table 3). In total, 52 008 participants were included in this systematic review, with only 18 278 (35.14%) women. Importantly, participants were from over 508 medical institutions located in over 17 Chinese provinces (out of a total of 34 provincial-level administrative units), with almost all studies conducted in hospitals located in urban areas of China. Only two studies were conducted in rural areas. There was significant heterogeneity between the studies in terms of instruments used to measure medication adherence, making a robust meta-analysis or statistical analysis difficult to conduct. Thus, a qualitative summary of the findings is presented. We organised our findings with three core themes: (1) Lack of knowledge and follow-up care are barriers to medication adherence; (2) patients’ sociodemographic characteristics, health status and medication characteristics influencing adherence; and (3) various intervention methods used for improvement of medication adherence. Subthemes are presented within each of these three core themes.
Summary of studies included in review
Lack of knowledge and follow-up care are barriers to medication adherence (12 articles)
Patients’ lack of knowledge (five articles)
Our systematic review revealed that patients’ lack of knowledge about their medications was a substantial barrier to adherence. For example, Wang and Li16 investigated the adherence to statins among 1368 elderly patients with CHD over 80 years of age, and found that lack of knowledge of CHD and statins was the main factor influencing their adherence to statins. Participants did not understand the importance of taking medications over the long term, did not know the morbidities of CHD and did not understand that statins can prevent CHD.16 Similarly, Li17 found that lack of knowledge of CHD was significantly related to poor adherence to statins among patients. Lack of knowledge was also a barrier to adherence among patients with uncontrolled cholesterol levels. Ding et al18 found that of 903 patients with CHD, 18.2% did not take statins. One major reason for those patients to not take statins was because they lack knowledge related to statins; they did not know that they should routinely control their low-density lipoprotein-cholesterol level by statins. Finally, Zhao et al19 conducted a descriptive correlational study among 159 participants with CHD and revealed that up to 38% of the participants were non-adherent and that lack of knowledge about medication and disease was significantly associated with non-adherence. Patients with good knowledge of the medication and disease were more likely to adhere to medication instructions.19 Dai20 surveyed 200 patients with CHD living in a Chinese rural area and found that medication adherence was low among those patients living in rural China, with only 6.4% of the participants adhering to their cardioprotective medications. Factors that contributed to poor medication adherence included poor communication between healthcare providers and patients, healthcare providers not fully explaining CHD and medications, and patients’ lack of clarity on factors to pay attention to while taking medications.20
Physicians’ practice and the lack of follow-up care regarding medication-taking behaviours (nine articles)
In China, there is a lack of proper follow-up care regarding medication-taking behaviours among patients with CHD. Bi et al2 investigated 2973 patients with acute coronary syndromes in 49 hospitals in China on their medication-taking behaviour at the time of hospitalisation and one year after hospital discharge. Bi et al2 found that sustained use of medications among participants was suboptimal; the use of recommended cardioprotective medications continued to decrease over time. Eighty per cent of non-adherent participants reported that they did not take antiplatelets after discharge because they did not receive follow-up information from physicians that they need to continue to take medications.2 Similarly, Hu et al21 and Li et al22 conducted large multicentre studies surveying statin usage in outpatients with CHD and found that, although statins were prescribed for outpatients by physicians, the rate of achieving the target cholesterol level was low. The possible reason for this suboptimal health outcome was lack of follow-up care for patients.
Zhang et al12 studied the long-term beta-blocker therapy after hospital discharge among patients with CHD and found that only 49% participants consistently used beta-blocker after discharge and 22% participants never used it, although consistent use of beta-blocker can lower mortality and cardiovascular events. Base on this finding, Zhang et al12 recommended that improving long-term medication adherence among patients with CHD is necessary, and to improve this long-term adherence actions should be taken to promote patients’ follow-up care regarding medication-taking behaviours and to improve physicians’ prescribing practices. In more recent studies, Wang et al23 and Li et al24 found that physicians’ prescribing practices could influence patients’ medication-taking behaviours and health outcomes. The results from Jiang et al13 supported these findings. Jiang et al13 studied 837 physicians from cardiology departments in 35 tertiary hospitals in China and found that a gap between guideline requirements (American Heart Association/American College of Cardiology Guidelines for Secondary Prevention for Patients with Coronary and Other Atherosclerotic Vascular Disease) and clinical practice in CHD secondary prevention contributed to poor medication adherence in China. Likewise, Ding et al18 and Wang et al23 found that a disparity between guidelines and physicians’ prescribing practices for patients with CHD exists in China. Xu et al’s25 study showed that physicians from traditional Chinese medicine hospitals were less likely to prescribe beta-blockers and ACE inhibitors for patients with CHD in comparison with physicians from West medicine hospitals in China. Overall, our review showed that physicians’ prescribing practices can influence patients’ medication-taking behaviours, and lack of follow-up care for patients with CHD regarding medication-taking behaviours was a consistent barrier to medication adherence among Chinese patients with CHD.12 22–25
Patients’ sociodemographic characteristics, health status and medication characteristics influencing adherence
Sociodemographic characteristics that are associated with adherence
Age (five articles)
Several studies3 16 17 26 27 have demonstrated a link between older adults and poor adherence to cardioprotective medication. For example, Jin et al3 found that among Chinese patients with acute coronary syndrome, medication non-adherence was common among older patients aged 65 and above. Li et al26 also found that adherence to statins was low among older adults. To further analyse adherence to statins in elderly patients, Wang and Li16 chose 1368 elderly patients aged over 80 years with CHD and found that older patients have poor medication adherence, and the authors surmised that memory loss or inability to remember medication name, dosage, route and time may be a key explanatory factor. More recently, two studies17 27 found older age (>60) to be a main influencing factor contributing to Chinese patients’ poor adherence to cardioprotective medications.
Gender (one article)
Medication adherence can be different among male and female patients with CHD. Yang et al28 compared medication adherence between male and female patients with CHD and found that female participants had better adherence to aspirin, beta-blockers and ACE inhibitors/angiotensin II receptor blockers, while there was no significant difference between female and male participants in adherence to statins.
Education (eight articles)
Seven out of eight studies3 16 17 20 27 29–31 revealed that a low educational level is a main influencing factor that contributes to poor medication adherence. Wang and Li16 investigated the reasons behind this relationship and found patients with a high educational level (>high school) are more likely to gather information about their medications; therefore, they have a better understanding and knowledge of statins. This better understanding contributed to better medication adherence.16 However, Jiang et al29 surveyed 5047 outpatients with stable angina from 298 hospitals in 15 Chinese provinces and found that patients with a high school or lower education level had higher beta-blockers adherence than those with a college degree. This result is different from our general finding that patients with a higher educational level are more likely to have better medication adherence.
Income (six articles)
Our review shows that low income was consistently found to be a factor related to medication non-adherence.3 Li32 explored cardioprotective medication adherence among 271 patients with CHD and revealed that patients with high family income (>¥50 000 per year) have significantly better medication adherence. Further, studies16 17 investigated patients with CHD on their adherence to statins and found that finances are an influencing factor to medication adherence. Studies30 33 on adherence to other cardioprotective medication such as antiplatelets also found the same result. Huang et al30 investigated the factors influencing medication adherence among 262 patients with CHD who received percutaneous coronary intervention and found that poor adherence to antiplatelets a year after hospital discharge was correlated with low economic status. Liu et al33 investigated the main cause of non-adherence to ticagrelor, an antiplatelet decreasing the risk of myocardial infarction,34 and found that low economic status is a main cause of non-adherence.
Medication cost/insurance (four articles)
Many studies3 17 30 31 in our review found that high medication cost was related to poor medication adherence. For example, Zhang and Chen31 investigated 500 patients with CHD on their adherence to antiplatelet therapy and revealed that high medical payment was related to poor adherence. Specifically, patients having public medical insurance had higher medication adherence than patients who had rural cooperative medical care or needed to pay medical care out of own pocket.30 31 Similarly, Jin et al3 and Li17 found that medication cost was an influencing factor that contributed to poor adherence. Participants with no insurance or who had to pay medication out of pocket had poorer medication adherence.17
Health status in relationship with adherence
Comorbidity (four articles)
Our review suggests that patients with CHD with comorbidity are more likely to have poor medication adherence. Zhang and Chen31 studied 547 patients with CHD on their adherence to dual antiplatelet therapy 1 year after they underwent percutaneous coronary intervention and revealed that having comorbidities contributed to low medication adherence. Similarly, Chen et al35 studied the association between heart function and medication adherence and found that patients with CHD with reduced left ventricular ejection fraction had lower medication adherence. Furthermore, Jin et al3 found that the higher the number of comorbidities, the greater the chance of medication non-adherence. Li et al26 found that statin use was low among certain high-risk patients with CHD, including those with hypertension or diabetes, even though the benefits of statin are great among this population.
Discharge (seven articles)
Medication adherence among Chinese patients with CHD often drops significantly after discharge from the hospital. Zhuang et al27 studied 348 discharged patients with CHD about their adherence to antiplatelet therapy and revealed that medication adherence gradually decreased after patient discharge. Similarly, Li et al26 found that among 13 150 patients with CHD, continued use of statin dropped substantially over time. Atkins et al36 also found that among 236 patients with CHD, continued use of cardioprotective medications declined over time. This result is similar to findings from two previous studies.3 32 The two studies found that recommended cardioprotective medications were commonly underused among Chinese patients with CHD one year after hospital discharge. To further investigate the relationship between discharge and medication adherence, Zhang and Chen31 and Huang et al30 investigated the factors influencing medication adherence among patients with CHD who received percutaneous coronary intervention. They found the same results: adherence to antiplatelet dropped over time.30 31 In summary, our review found that the longer the time after discharge, the poorer the medication adherence.
Medication characteristics that are related to adherence
Adverse effects (five articles)
Adverse effects are associated with decreased medication adherence among patients with CHD. This was supported by several studies in our review.3 17 20 26 33 Dai20 surveyed 200 Chinese patients with CHD and found that the fear of adverse effects of cardioprotective medication was a barrier to adherence. Jin et al3 investigated the main influencing factors to medication non-adherence among patients with CHD and found the fear of adverse effects such as sexual dysfunction, depression and fatigue were a confirmed factor. Similarly, Liu et al33 investigated the main cause of the non-adherence to ticagrelor, an oral antiplatelet drug decreasing the risk of myocardial infarction,34 and found that adverse effect of ticagrelor, such as haemorrhage, is one main cause. Li17 studied 138 patients with CHD on their adherence to statins and found that adverse effects of statins are indeed a factor contributing to poor adherence. Taking statins over time can influence the musculoskeletal system, neurological system and liver dysfunction.17 To further study the association of adverse effects and non-adherence to statins, Li et al26 categorised 16 860 patients into different risk levels. They found that statin use was low among high-risk patients with CHD even though the absolute benefits of using statins are high among this population. Li and colleagues thought this might be because of a treatment-risk paradox. Treatment-risk paradox is a phenomenon in which patients at high risk for adverse events receive less-intensive treatment than do patients at lower risk.37
Number of discharge medications (two articles)
Two studies in our review found that the greater the number of discharge medications patients received, the greater the chance of medication non-adherence. Li17 studied 138 patients with CHD on their adherence to statins and found that using multiple medications was an influencing factor that contributed to poor adherence. Also, Dai20 surveyed 200 patients with CHD living in a Chinese rural area and found that using multiple medications was a factor that contributed to poor medication adherence.
Interventions to improve medication adherence vary in methods
Our systematic review found that researchers explored various interventions to improve adherence to cardioprotective medication of patients with CHD. Follow-up phone calls, educational lectures, booklets and reminder cards were common methods found to be effective in improving medication adherence. Education and reminders are two key components of all interventions.
Follow-up phone calls (five articles)
Making follow-up phone calls to remind patients to take medications or give consultations on medication usage is the most common method we found in the review. Du et al38 randomised 964 patients with CHD into an intervention or control group. Participants in the intervention group received medical consultations from a cardiologist through phone calls at 3, 6, 12 and 36 months postdischarge. The study found that the intervention group had significantly better medication adherence.38 Similarly, Li et al39 used phone call interviews to educate participants with myocardial infarction on relevant knowledge after discharge and found this intervention was effective in improving medication adherence. Telephone follow-up was used in many randomised controlled trials.40–42 For example, Jiang et al40 tested the effectiveness of a nurse-led cardiac rehabilitation educational programme in improving health behaviours among 167 randomly selected patients with CHD. In the programme, an experienced cardiac nurse provided patients with professional follow-up through telephone calls to monitor, facilitate and reinforce self-management practice of the patients. Patients who received the intervention demonstrated a significantly better performance in medication adherence.40 Similarly, Cao et al43 conducted a randomised controlled trial to test the effectiveness of a hospital–community partnership transitional programme on medication adherence. In the programme, family physicians and home nurses made structured telephone calls after patient discharge to reinforced health self-management behaviours and remind timely outpatient visits to hospital, whereas patients in the control group received routine care. Cao et al43 found that the intervention group had significantly higher medication adherence scores than the control group at 30 days and 90 days after discharge.
Zhao et al41 examined the impact of using a clinical pharmacist support programme on medication adherence among patients receiving multidrug therapy for CHD in China. Compared with a usual care control group, the intervention group received pharmacist support that included medication review, patient education, lifestyle management, discharge guidance and telephone follow-up. Patients in the intervention group showed better medication adherence.41 Zhao and Wong44 tested the effectiveness of a nurse-led postdischarge transitional care programme for patients with CHD that included a community nurse who followed up with participants’ adherence behaviour for 4 weeks. Compared with the control group, which received routine care, the intervention group had significantly better adherence to their medications.44
Booklet (three articles)
Giving a booklet for patients to refer important information of CHD and their medication was found to be effective in our review. However, none of the three studies used booklet alone; booklet was used with other interventions to improve medication adherence, such as follow-up phone calls, educational session or individual face-to-face education. Wu et al45 found patients in an intensive management group had better medication adherence than patients who received routine care. A booklet of CHD was provided to participants in the intensive management group. With such a booklet, patients can learn CHD-relevant knowledge from it. The booklet increased participants’ awareness of taking medications. Similarly, Jiang et al40 provided a healthy heart booklet that covered medication management to patients with CHD to facilitate and reinforce their medication adherence. Zhao et al42 investigated whether a pharmaceutical care intervention can improve medication adherence. In this intervention, an instructional list of each medication was provided to patients.
Medication memo card (one article)
A medication memo card was found to be an effective method to improve medication adherence. Li et al39 conducted a randomised controlled trial to improve medication adherence of patients with CHD. Intervention in the study included giving a medication memo card to participants with a physician’s prescription and time of taking medications.39 This method improved patients’ medication adherence.
Short message service (one article)
Using a sample of 280 outpatients, Fang and Li46 examined the effectiveness of an electronic messaging support service programme as a means of providing discharged patients with reminders and coronary artery disease-related health information. Fang and Li46 found that compared with the control group who received phone calls, the group who received medication reminders via short message service (SMS) had better cumulative adherence to lipid-lowering therapy after 6 months of the programme.
Mobile app (one article)
Fang and Li46 built a public platform on one of the most popular mobile apps in China called WeChat. From a computer, healthcare providers regularly released to the WeChat platform CHD-related information on cardioprotective medication, including its function, method of use and side effects. Patients in the experimental group had open access to all information on the WeChat platform.46 Fang and Li46 found that compared with the control group, the experimental group had better cumulative adherence to lipid-lowering therapy after 6 months of the programme.
Educational session/individual face-to-face education (six articles)
Jiang et al40 tested the effectiveness of a nurse-led, hospital-initiated, cardiac rehabilitation educational programme to improve health behaviours of 167 patients with CHD, including medication adherence. The cardiac rehabilitation programme of this study was started in the hospital and maintained to 12 weeks after discharge, consisting of seven educational sessions covering (1) CHD and self-management principles, (2) medication management, (3) angina prevention and management, (4) physical exercise, (5) dietary management, (6) smoking cessation and (7) family support. Patients who received this intervention demonstrated a significantly better performance in medication adherence.40 In addition, educating participants’ family members improved medication adherence. Li et al39 conducted a randomised controlled trial to improve medication adherence. Interventions for the experimental group included educating participants’ family members on how to care for patients with myocardial infarction at months 1, 3, 6, 9 and 12 postdischarge.39 Individual face-to-face education provided by healthcare providers also can improve medication adherence.41 Zhao et al41 examined the impact of using a clinical pharmacist support programme on medication adherence among patients receiving multidrug therapy for CHD in China. Compared with a usual care control group, the intervention group received pharmacist support that included individual face-to-face patient education. As a result, patients in the intervention group showed significantly better understanding of the importance of medication adherence and improved medication adherence.41 Similarly, in the study conducted by Zhao et al,42 Cao etal,43 and Zhao and Wong,44 healthcare providers gave medical directions and explained the importance of taking cardioprotective medications to patients. The result was that the medication adherence rate was higher in the pharmaceutical care group.42
In addition to investigating the advantages of each intervention, disadvantages of the interventions were rarely mentioned in the reviewed studies. Only one study46 discussed that mobile apps and SMS require patients to have access to a cellular data network; therefore, these interventions may be less applicable to patients in rural areas who do not have access to smart phones or cellular networks, or who are illiterate.
Discussion
Cardioprotective medications were commonly prescribed as secondary prevention medication to patients with CHD in mainland China.2 In this systematic review, we found that adherence to these medications gradually decreased during a follow-up period.2 13 35 This finding is a critical public health issue in China because long-term pharmaceutical therapy is essential for the treatment of CHD, and non-adherence to cardioprotective medications could render futile any effort to treat CHD47 and cause severe adverse health outcomes. In this review, we synthesised the findings to provide a clearer understanding of factors related to poor adherence, which we organised into several key themes. Also, we summarised all interventions that have been taken to improve medication adherence. The impact of the lack of medication-related knowledge among patients with CHD cannot be underemphasised and served as a barrier to medication adherence. Future programmes aimed to improve medication adherence should develop interventions to improve patients’ knowledge of their medications, such as function, frequency and dosage. Our review showed that, in China, lack of proper follow-up care for patients with CHD regarding their medication-taking behaviours is also a barrier to medication adherence; therefore, to improve medication adherence, interventions should be taken to promote follow-up care. Future interventions aimed to improve medication adherence should increase access to care and care delivery of patients with CHD after their discharge from hospitals. This systematic review found that medication-taking reminders and educational materials were the two core components for successful interventions aimed to improve medication adherence. Therefore, future interventions should adopt these two core components.
Also, our review showed that physicians’ prescribing practices can influence patients’ medication-taking behaviours and health outcomes; therefore, factors that compromised physicians’ prescribing practices should be studied. Several studies13 23 24 in this review mentioned that physicians’ knowledge deficiency of prevention guidelines was a factor. One possible reason for this knowledge deficiency could be the poor and slow dissemination of current guidelines. To improve this gap, a Chinese translation of current international guidelines could be helpful. Because most updated guidelines are made in the USA and Europe, they are written in English. Most Chinese physicians cannot read English or do not have time to read English guidelines. Finally, hospitals in mainland China should provide cardiologists, particularly young cardiologists, with further training opportunities on cardiology prevention and rehabilitation. Patients’ lack of follow-up care may also be related to the healthcare system in China. The included studies did not provide direct evidence to support this point, but empirical evidence from other studies has shown that patients with CHD prefer to use hospitals rather than local primary healthcare clinics for treatment.48 Under the current system, most physicians in large hospitals are required to see a great number of patients each day, and they may not have a sufficient amount of time to provide advice to patients on medication adherence. Future studies should investigate the association of the number of patients seen by a physician on follow-up care and medication adherence.
We found that adherence is contingent on patients’ health and demographic characteristics, including age, education, comorbidities, number of medications prescribed, adverse effects and insurance. This finding is consistent with those found in other countries. For example, Du et al8 studied the impact of medication adherence on clinical outcomes through summarising studies conducted in Canada, USA, Argentina, Brazil, Italy, Paraguay and Spain. Du et al8 found that frequency, insurance coverage, patient education and follow-up were factors that can influence medication adherence. Similarly, Ho9 summarised studies from multiple nations and found that age, side effects, regimen complexity, low literacy and social support were related to medication adherence. Overall, patients from more affluent backgrounds and with access to care were likely to have better medication adherence. Many interventions have been tested by researchers to improve medication adherence. Unimodal interventions were less successful than multimodal interventions because medication non-adherence was often related to multiple factors.9 In our systematic review, we found a similar result that interventions to improve medication adherence varied in methods, but that education and reminder were the consistent key components of all interventions.
We used a set of criteria to assess the quality of evidence provided by each of the included 33 studies. These criteria included study design, sample selection, measures, statistical analyses, reporting, content and utility.49 Our review revealed a significant variation in the quality of reviewed studies. Overall, studies published in English journals provided more methodological details than those published in Chinese journals. The major limitations to some of the 33 studies included using non-representative samples, unstandardised assessment measures and an insufficient number of longitudinal findings. Therefore, findings from this review are not conclusive.
However, they provide a foundation from which to conduct future research. In particular, findings suggest the following: (1) More research should be conducted on how to establish high-quality health educational programmes aimed to increase patients’ medication adherence. (2) In China, educating patients to take medications is the responsibility of healthcare providers. However, this review found that many Chinese physicians did not provide patients advice on the importance of medication adherence. This might be due to physicians’ insufficient or not up-to-date knowledge of cardioprotective medications or due to physicians’ lack of time allocated for each patient. Further, no articles in this review explored nurses’ and pharmacists’ knowledge of cardioprotective medications. To further explore the reasons for poor cardioprotective medication adherence among patients with CHD in mainland China, future studies should focus on the roles of all healthcare providers on patient education and prescribing patterns. Improving discharge prescription of cardioprotective medications and promoting long-term patient adherence are critically needed in China. (3) Many studies in this review were conducted in urban areas of China. Given that there is a big difference in medical care between urban areas and rural areas of China, future research should study medication adherence among patients with CHD living in rural China. (4) In the meantime, income and cost are consistently found to be associated with medication adherence. China is in the process of undergoing healthcare reform and extending health insurance coverage in rural areas. Demonstration projects are needed to examine the cost-effectiveness of health insurance extension on medication adherence. More robust studies are needed to examine the mediator and moderator factors associated with medication adherence using longitudinal data.
Acknowledgments
We thank Jamie Conklin, Research and Education Librarian at Duke University Medical Center Library, for assistance in building the combination of index and search terms.
References
Footnotes
Contributors All authors contributed to the conception and design of the study. ZN, LD and Dr. Ryan Shaw were responsible for the data acquisition and analysis. All authors contributed to data interpretation and to writing and approving the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.