Article Text

Abstract
Objectives Myeloperoxidase, an abundant leucocyte enzyme, is elevated in culprit lesions that have ruptured in patients with sudden cardiac injury. Multiple lines of evidence suggest an association between myeloperoxidase and inflammation and acute coronary syndrome. Myeloperoxidase has been proposed as a potent risk marker and diagnostic tool in acute coronary syndrome (ACS). Recent studies have reported the potential use of myeloperoxidase in acute coronary syndrome, but limited reports are available on its utility in different groups of ACS in the emergency department. Therefore the circulating levels of serum myeloperoxidase in patients with acute coronary syndrome and control subjects were studied.
Design and setting The levels of serum myeloperoxidase were measured by ELISA in 485 patients admitted to emergency care unit, of which 89 patients were diagnosed as non-cardiac chest pain (NCCP). The levels of myeloperoxidase were significantly increased in patients with ACS when compared with controls and NCCP. From the receiver operator characteristic (ROC) curve analysis, the optimum value above which myeloperoxidase can be considered positive was found to be 48.02 U/ml. The area under the curve was found to be 0.956 with 95% CI (0.934 to 0.973) (p<0.0001). A combination analysis of ROC curves of troponin, creatine kinase MB (CK-MB) and myeloperoxidase showed myeloperoxidase to be highly significant. Multivariate analysis revealed myeloperoxidase to be an independent diagnostic marker for early diagnosis of ACS.
Conclusion Myeloperoxidase, in contrast to troponin and CK-MB, identified patients at risk of ischaemic events, even in the absence of myocardial necrosis, thus highlighting its potent usefulness for risk stratification among patients presenting with chest pain.
Statistics from Altmetric.com
Myeloperoxidase is a well-known enzyme, primarily released by activated neutrophils characterised by powerful pro-oxidative and proinflammatory properties. Multiple lines of evidence have suggested the predictive value of serum myeloperoxidase in patients presenting to the emergency department with chest pain and also prognostic capacity of the adverse cardiac outcomes over 30 days to 6 months.1 2 Particularly in the setting of unstable angina, which mainly circumvents these events, myeloperoxidase serves to be a potent risk predictor. The vital role of myeloperoxidase is the host innate defence by the synthesis of oxidants such as hypochlorous acid (HOCL). However, this enzyme and the products of the enzyme-catalysed reactions play a significant role in the process of atherogenesis. Myeloperoxidases render LDL atherogenic and HDL dysfunctional. It also catalytically consumes nitric oxide contributing to the endothelial dysfunction.
Recent findings have demonstrated the potential mechanisms by which myeloperoxidase may promote plaque instability. In vitro studies have demonstrated that myeloperoxidase-derived HOCl promotes the activation of latent matrix metalloproteinase-7 via oxygenation of a thiol residue in the enzyme cysteine residue.3 Activated matrix metalloproteinases destabilise the plaque, which undergoes thinning and subsequent breakdown of the overlying fibrous cap.
The purpose of this study was to evaluate the diagnostic capacity of myeloperoxidase for early classification of patients with acute coronary syndrome at the emergency unit and also to analyse the enhanced prediction of ACS on combined assessment of troponin I, creatine kinase MB (CK-MB) and myeloperoxidase.
Methods
Research subjects
The study was carried out at the Department of Biochemistry and Clinical Lab, International Centre for Cardio Thoracic and Vascular Diseases, Frontier Lifeline & Dr KM Cherian Heart Foundation, Chennai, India. The patients were enrolled in the study upon arrival to the emergency department with chest pain. Written informed consent was obtained from the study subjects, and the study was approved by the Institutional Ethics Committee
The study group included 485 patients admitted to CCU with manifestations suggestive of acute myocardial ischaemia, including those with chest pain with or without radiation, palpitations, shortness of breath, lower jaw pain, left arm pain, epigastric pain, hypotension and other symptoms suggestive of angina. Twelve-lead ECG and all demographic details of the patients were recorded. Of the 485 patients admitted to CCU, 297 patients had acute coronary syndrome (98 patients with ST-segment elevation, 99 patients without ST segment elevation and 100 patients with unstable angina) with a mean age of 55 (SD 11) and 76% of them being males. Remaining 188 patients were diagnosed as non-cardiac chest pain (NCCP) with a mean age of 52 (11) and 67% being males. Among 99 healthy volunteers with no clinical evidence of heart disease had a mean age of 50 (12) and the proportion of males being 63%. Patients with liver, kidney disorders, brain ischaemia and tumour were excluded from the study.
Study protocol
Venous blood was drawn from patients admitted to CCU within 4–6 h after symptom onset, into plain tubes (without anticoagulant) and allowed to clot for 30 min before centrifugation. Serum was separated and stored at −40°C until analysis, and the samples were thawed only once.
Biochemical analyses
Serum myeloperoxidase was measured using ELISA (Aeskulisa, Wendelsheim, Germany). The concentrations of troponin I and CK-MB were determined by MEIA (Abott Axsym, Munich) and IFCC Method. Troponin I levels above 0.1 ng/ml and CK-MB levels above 25 U/l were considered positive. Biochemical parameters such as lipid profile, glucose, urea, creatinine, total protein and haemoglobin were analysed using a fully automated analyser (Biochemical Andlyzer, Randox Instruments, Crumlin, UK). The patients' medical histories were recorded.
Statistical analysis
Statistical evaluations were performed using SPSS software 9.0 (SPSS, Chicago). A receiver operator characteristic (ROC) curve analysis was done using MedCalc 9.6 (MedCalc Software, Mariakerke, Belgium). Data are expressed as mean (SD) for continuous variables and percentage (%) for categorical variables. Significances between subgroups were analysed using the Kruskal–Wallis test. p Values below 0.05 were considered statistically significant. A multivariate logistic regression was performed to determine a single marker which can independently diagnose the incidence of ischaemic events.
Results
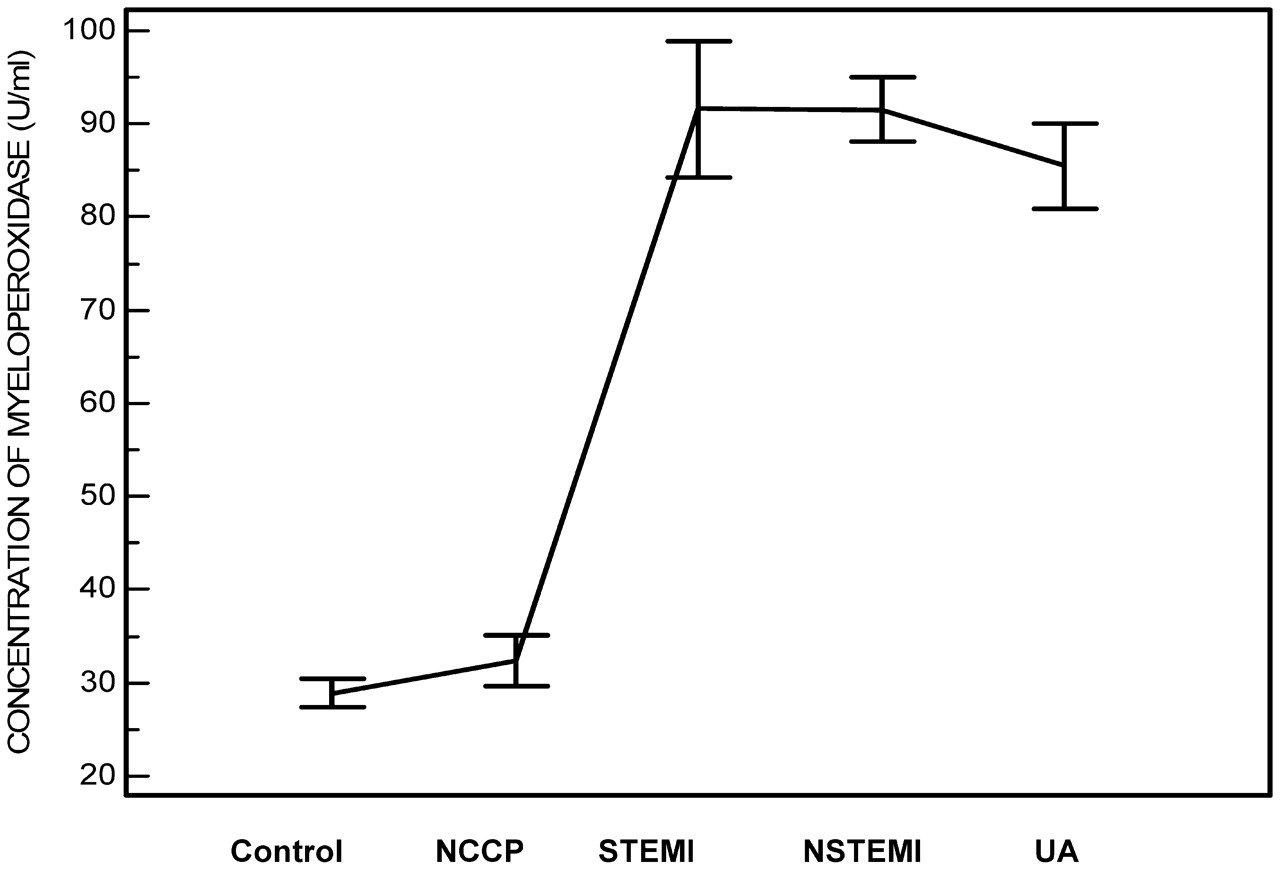
The patients' clinical characteristics and biochemical parameters are listed in table 1. The mean myeloperoxidase levels in ST-segment elevation myocardial infarction (STEMI) patients (91.58 (36.15)), non-ST-segment elevation myocardial infarction (NSTEMI) patients (90.51 (17.25)) and unstable angina (UA) patients (85.49 (23.19)) were significantly higher than non-cardiac chest pain (NCCP) patients (32.44 (13.02)) and also healthy volunteers (28.87 (7.76)) (p<0.001) (table 2). Figure 1 shows the mean myeloperoxidase levels in different groups. The mean myeloperoxidase values in patients and controls are shown in fig 2.
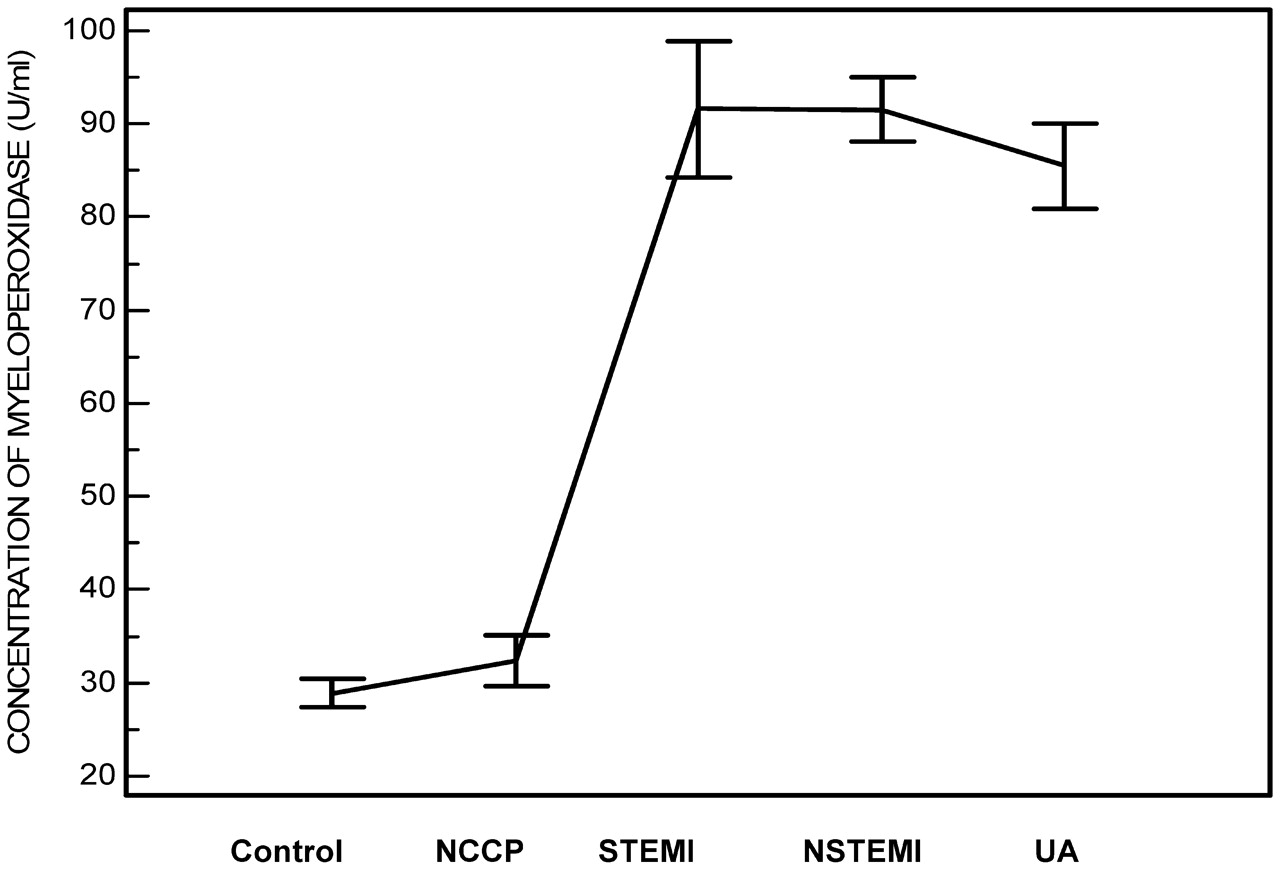
Myeloperoxidase levels in serum of control, non-cardiac chest pain (NCCP) and subgroups of acute coronary syndrome patients (unstable angina (UA), ST segment elevation myocardial infarction (STEMI) and non-ST segment elevation myocardial infarction (NSTEMI)).
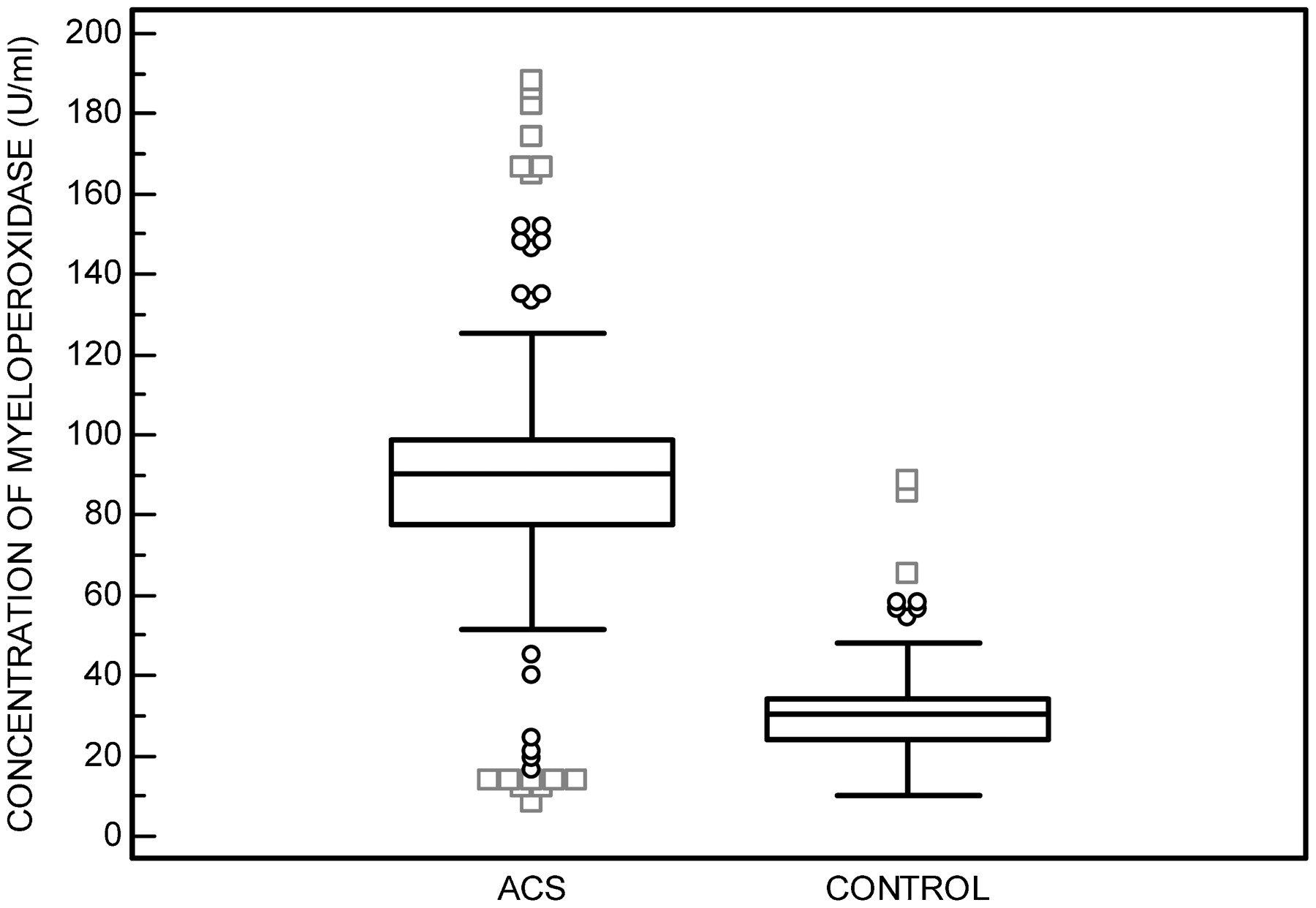
Myeloperoxidase levels in serum of control and acute coronary syndrome patients.
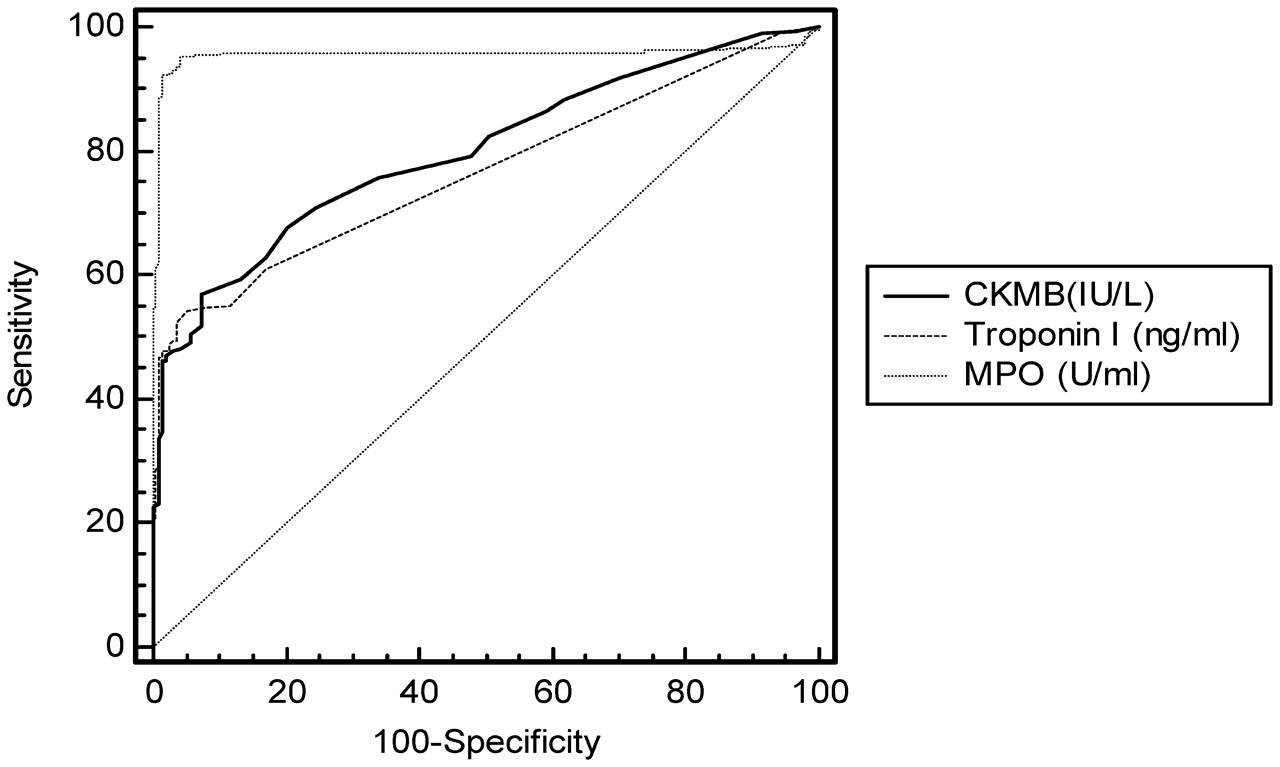
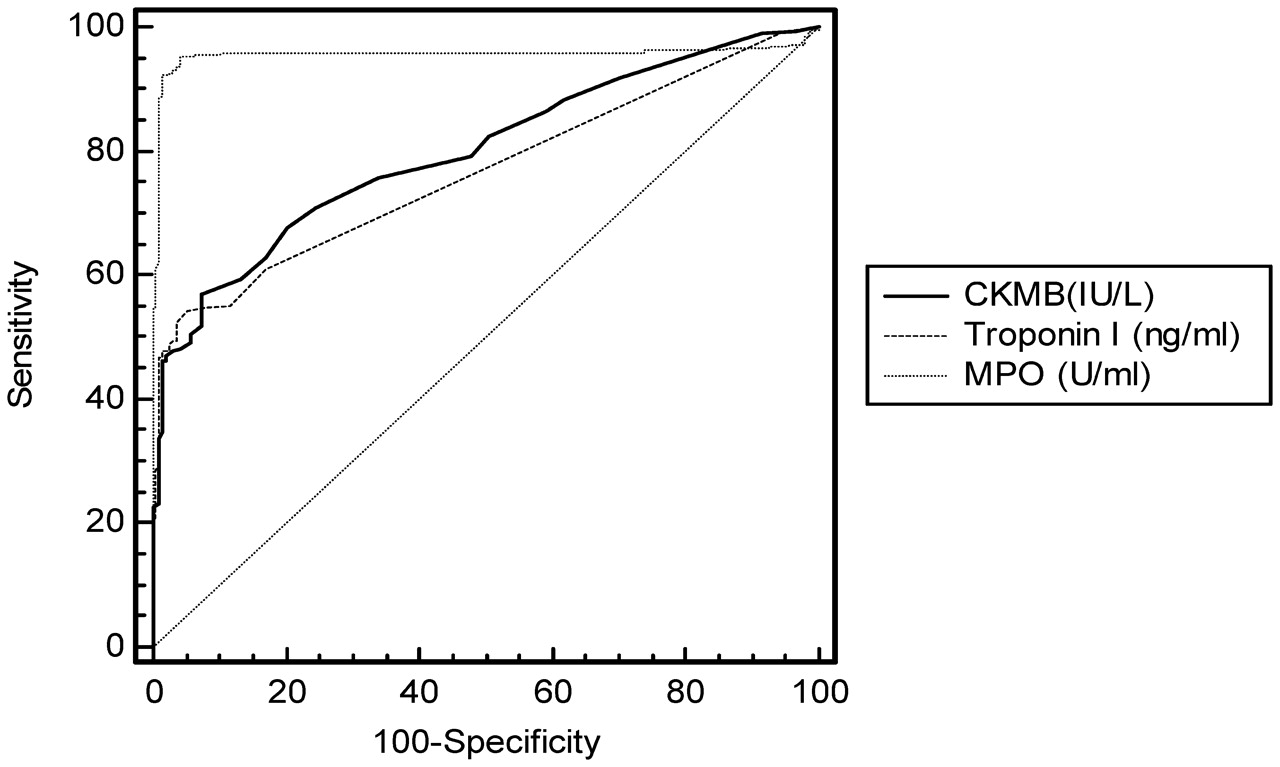
From the ROC curve, the optimum value above which myeloperoxidase can be considered positive was found to be 48.02 U/ml (fig 3). The area under the curve was found to be 0.956 with 95% CI (0.934 to 0.973) (p<0.0001). The observed sensitivity and specificity were found to be 95% and 96% respectively. A combination analysis of ROC curves of troponin, CK-MB and myeloperoxidase showed myeloperoxidase to be highly significant (fig 4). A comparison of sensitivity, specificity, area under curve and 95% CI is given in table 3. Multivariate analysis revealed myeloperoxidase to be an independent analytical tool for diagnosis of acute coronary syndrome (table 4).

Receiver operator characteristic curve analysis for the assay of myeloperoxidase.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operator characteristic curve analysis of myeloperoxidase (MPO), troponin I and creatine kinase MB (CKMB).
Discussion
Patients who present to the emergency department without the evidence of myocardial necrosis are a diagnostically challenging group for risk stratification. Recently, MPO has been proposed as a useful risk marker and diagnostic tool in ACS and in patients admitted to the emergency room for chest pain.4 Low MPO levels were observed in circulating neutrophils of patients with acute myocardial infarction (AMI) and unstable angina (UA), and therefore high MPO levels in circulation when compared with chronic stable angina and variant angina. Troponin takes 4–6 h to rise during myocardial injury, whereas myeloperoxidase is elevated at baseline levels (even within 2 h after symptom onset) in patients initially negative for troponin. In the study by Biasucci and coworkers, CK-MB and troponin release did not correlate with MPO release, and the MPO content was measured using a Coulter counter, which is just an index of the amount of myeloperoxidase but not a quantitative measure.5
Previous studies have suggested that MPO measurements might have clinical utility for identifying risk of imminent cardiac events in a mixed cohort of acute cardiac and non-cardiac patients where ACS is not yet confirmed.6 However, Brennan et al have assessed the plasma levels of MPO to be a predictor of the risk of cardiovascular events in patients presenting to CCU. Zhang et al7 also observed higher values of MPO in patients with coronary artery disease than in controls. Our results were in complete agreement with the above-mentioned studies, since significant increases in MPO levels were observed in acute coronary syndrome patients than controls. These findings suggest that myeloperoxidase levels may be useful in triage in the emergency department, and elevated levels of myeloperoxidase may be a marker for unstable angina preceding myocardial necrosis. A striking feature observed in the previous studies were increased MPO levels even at negative troponin values, thus suggesting MPO to be a powerful marker of plaque instability.
The ROC analysis results demonstrated by Brennan et al showed a higher sensitivity, specificity, negative predictive value and positive predictive value of MPO (65.7%, 60.7%, 53.3% and 72.2%) when compared with troponin, CK-MB and CRP. Our results showed a much higher sensitivity, specificity, negative predictive value and positive predictive value (table 3), thus suggesting MPO to be a powerful marker to aid early classification of patients with ACS. MPO when combined with troponin seemed to be highly significant in the diagnosis of ACS, though the CK-MB and MPO combination was also found to be significant.
MPO not only aids in risk stratification but also predicts the risk of cardiac events during the 30-day and 6-month follow-up, especially in patients with negative troponin.1 2 Several studies have also investigated the value of MPO in predicting long-term outcomes.6 8 9 In the study by Mocatta et al, higher MPO levels were measured in AMI patients and a significant association of MPO with follow-up events was found. Interestingly, they observed MPO to have an incremental prognostic value over ejection fraction and BNP. One study by Meuwese et al10 evaluated the association of MPO levels with the risk of future coronary artery disease in apparently healthy individuals.
The ROC curve analysis of our study showed a higher area under the curve for MPO, and the mean values are also significantly elevated in ACS patients. No studies have carried out an ROC curve analysis in the South Indian population to arrive at a diagnostic cut-off value and shown a significant difference between NCCP and STEMI, NSTEMI and UA. Relatively higher MPO levels were observed in STEMI than in NSTEMI and UA. This may be due to elevated WBC levels in this group. MPO is pivotally involved in the pathogenesis of atherosclerosis. Apart from its major role in microbicidal activity, it also oxidises LDL, initiates lipid peroxidation, consumes nitric oxide as a substrate and also promotes endothelial dysfunction.11 12 In addition, MPO is associated with progression of carotid atherosclerosis in patients with HDL levels below 49 mg/dl.13 This is the first report to our knowledge in the Indian population wherein different groups namely STEMI, NSTEMI, UA and NCCP in comparison with healthy controls have been studied using the analytical value of myeloperoxidase. However, the smaller sample size is the constraint of the study, and attempts are in progress to investigate a larger sample size in each group which would definitely prove myeloperoxidase as a potential investigative marker.
In the study by Baldus et al,2 myeloperoxidase remained an independent and powerful predictor of cardiac risk at both 30 days and follow-up, in the multivariate analysis which included baseline characteristics and markers (troponin, vascular endothelial growth factor, CRP, sCD40L and white blood cell count). In our study, myeloperoxidase was found to be an independent diagnostic tool with a high odds ratio (p<0.001) (table 4). Troponin, total cholesterol, HDL, diabetes and family history of coronary artery disease were also found to be significant. Out of the total study population (485), 297 subjects were diagnosed as ACS, of which myeloperoxidase was positive in 267 samples in comparison with troponin (161) and CK-MB (169). In contrast, false negatives are still undesirable outcomes. Multivariate logistic regression was done to determine an independent marker capable of diagnosing the occurrence of ACS in the emergency department.
In conclusion, the present study revealed myeloperoxidase to be an independent investigative marker in patients with ACS, even at low troponin levels. This suggests that myeloperoxidase unmasks states of acute inflammation in the coronary circulation indicative of increased neutrophil activation, which ultimately precedes myocardial injury. Myeloperoxidase unravels the pathophysiology of ACS and also enables a better understanding of ACS to further consider this enzyme for risk stratification in patients with ACS and encourage the development of pharmacological strategies to modulate the catalytic activity of this enzyme.
Acknowledgments
The authors wish to thank the nursing staff, all the technicians of the Department of Biochemistry and Blood Bank for all the help rendered for sample collection and analysis, and C Raja for all the statistical analyses of the data. Special thanks to ET Thomas, Purchase Manager for the prompt procurement of reagents and chemicals.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Institutional Ethics Committee, International Centre for Cardiothoracic and Vascular Diseases, Dr KM Cherian Heart Foundation (a unit of Frontier LifeLine Pvt Ltd).
Provenance and Peer review Not needed