Article Text

Statistics from Altmetric.com
A 43-year-old man presented to the emergency department with haemodynamically compromised ventricular tachycardia necessitating electrical cardioversion. Classical “epsilon waves” noted on his initial electrocardiogram prompted an evaluation for arrhythmogenic right ventricular dysplasia. The diagnosis was confirmed with echocardiography and magnetic resonance imaging of the heart. A prompt recognition and management of this condition in the emergency department helped prevent significant mortality that may be associated with arrhythmogenic right ventricular dysplasia.
A 43-year-old man was admitted to a regional hospital elsewhere with a history of recurrent palpitations, syncope and ventricular tachycardia (VT). He was started on amiodarone, required cardioversion several times for termination of VT and was finally transferred to our hospital. He presented to the emergency department (ED) with palpitations and hypotension (BP=80/60 mm Hg). The 12-lead ECG showed wide QRS tachycardia suggesting monomorphic VT (180 bpm) of left bundle-branch block (BBB) morphology with left-axis deviation. The patient was cardioverted immediately with 200 J. The ECG during sinus rhythm showed a discrete wave (epsilon wave) just beyond the QRS complex1 and inverted T waves in the right precordial leads (fig 1).

{kind=link}
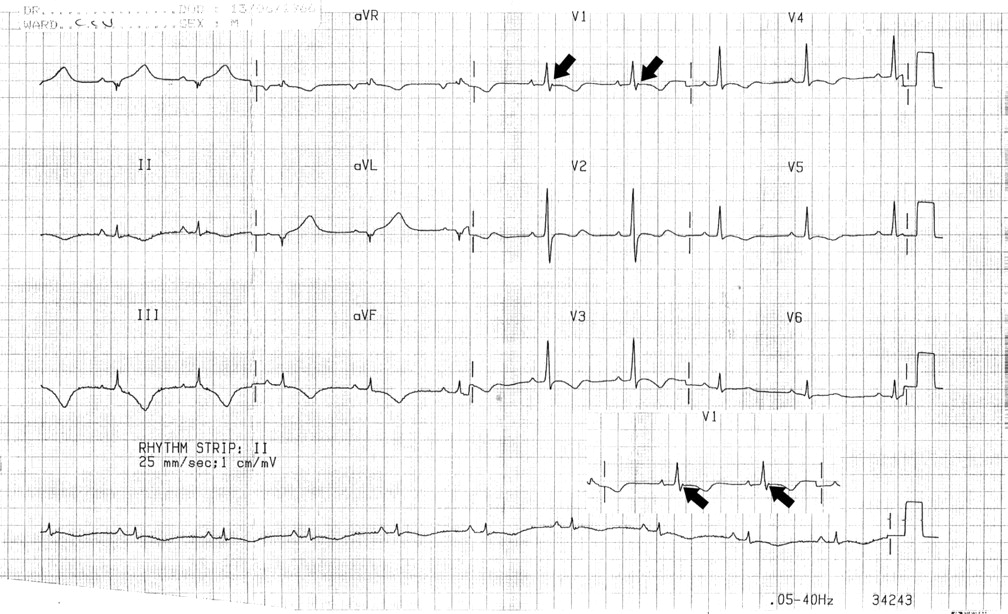
Electrocardiogram during sinus rhythm showing epsilon waves (arrows) in lead V1.
On the basis of the ECG, a diagnosis of arrhythmogenic right ventricular dysplasia (ARVD) was considered, which was confirmed by echocardiogram and magnetic resonance imaging. He was started on sotalol and subsequently underwent ICD insertion. ARVD is an under-recognised clinical entity characterised by ventricular arrhythmias and a specific ventricular pathology. The ECG is the initial investigation in the diagnostic approach of this disease. A pattern of incomplete or complete right BBB, the epsilon wave and T inversion in precordial leads are typical ECG findings in these patients. Given its uncommon occurrence and first presentation often being in ED, it is important for ED physicians to be aware of its presentation, classical ECG findings and management.
References
Footnotes
Competing interests None.
Provenance and Peer review Received.