Article Text

Statistics from Altmetric.com
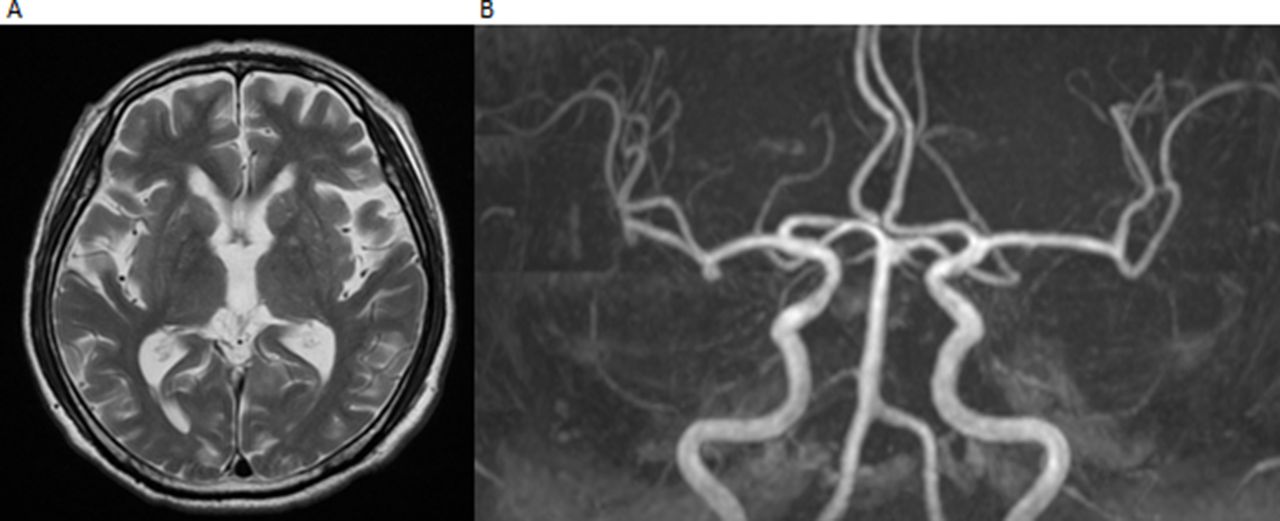
A 75-year-old man with a history of diabetes mellitus presented with chest pain. He was diagnosed with acute ST-elevation myocardial infarction. Emergent coronary angiography revealed proximal left anterior descending (LAD) artery occlusion. Primary percutaneous coronary intervention (PCI) was then performed. During aspiration thrombectomy, he went into cardiopulmonary arrest. Cardiopulmonary resuscitation (CPR) was started immediately. Recovery of spontaneous circulation was obtained after 7 min of CPR while PCI of the LAD was being performed simultaneously. A drug-eluting stent was deployed over the culprit lesion and the occluded artery was reperfused. After PCI, whole-body CT was performed because of transient haemodynamic instability. Non-contrast CT after PCI showed high-density areas in the cortex, putamen, caudate nucleus and subarachnoid space of the right cerebral hemisphere (figure 1A). No neurological symptoms were observed because the patient was intubated. CT imaging on hospital day 2 showed disappearance of the high-density areas (figure 1B). MRI on hospital day 12 revealed no particular abnormalities (figure 2A). Magnetic resonance angiography showed no intracranial artery occlusions (figure 2B). He recovered completely without any neurological deficits or cardiac complications. We diagnosed contrast-induced encephalopathy (CIE). CIE is a reversible neurological complication associated with contrast administration.1 In acute ischaemic or haemorrhagic stroke, abnormalities remain on follow-up imaging, whereas they disappear in CIE. CIE after PCI is an extremely rare complication.1 We emphasise the need for increased awareness of CIE in patients with acute coronary syndrome undergoing PCI. It is noteworthy that CIE mimicked an ischaemic or haemorrhagic stroke.
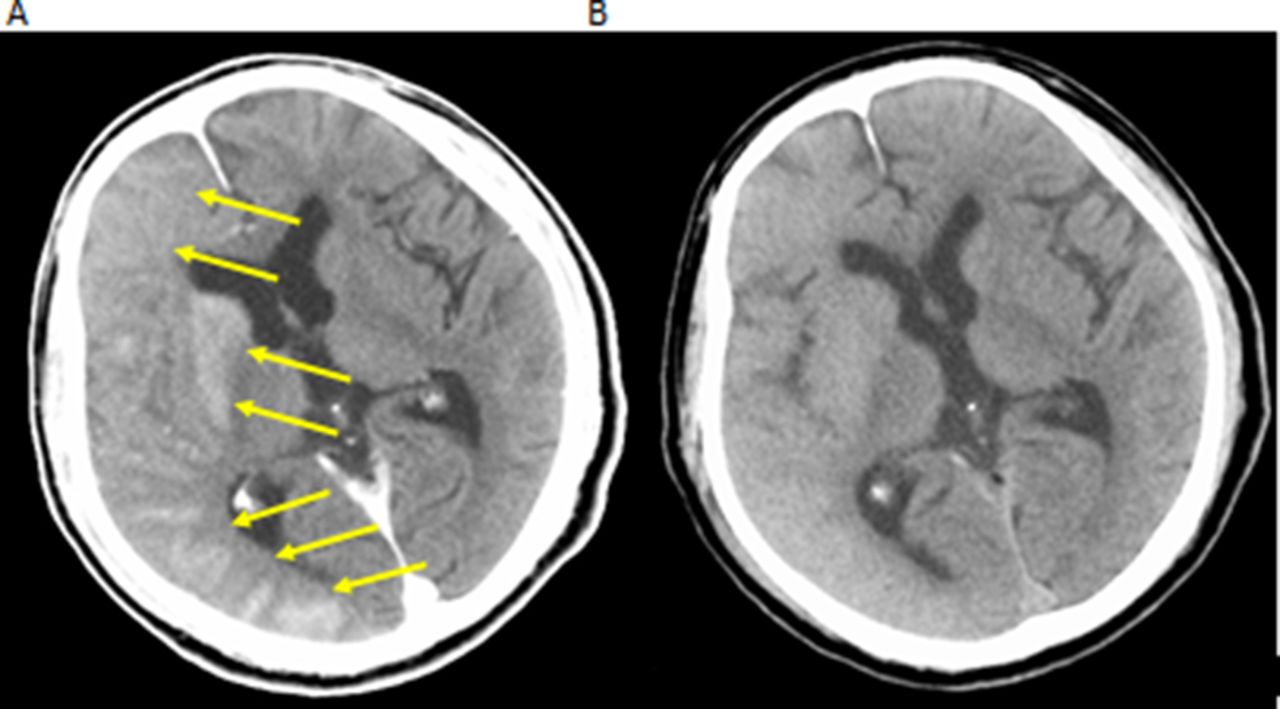
(A) CT imaging after percutaneous coronary intervention showed high-intensity areas in the cortex, putamen, caudate nucleus and subarachnoid space (arrows), mimicking subarachnoid haemorrhage. (B) CT imaging on hospital day 2 revealed reduced oedema and disappearance of the high-density areas.
{kind=link}
{kind=link}
(A) T2-weighted MRI on hospital day 12 showed no abnormalities suggestive of cerebral infarction or subarachnoid haemorrhage. (B) Magnetic resonance angiography showed no intracranial artery occlusions.
Footnotes
Contributors All the authors were involved in the clinical management of the patients. SH drafted and MK revised the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.