Article Text

Abstract
The benefits of inhibiting the renin–angiotensin–aldosterone system (RAAS) are well established for left ventricular dysfunction, but remain unknown for right ventricular (RV) dysfunction. The aim of the current meta-analysis is to investigate the role of RAAS inhibition on RV function in those with or at risk of RV dysfunction. Medline, PubMed, EMBASE and Cochrane Libraries were systematically searched and 12 studies were included for statistical synthesis, comprising 265 RAAS inhibition treatment patients and 265 placebo control patients. The treatment arm showed a trend towards increased RV ejection fraction (weighted mean difference (WMD)=0.95, 95% CI −0.12 to 2.02, p=0.08) compared with the control arm. Subgroup analysis demonstrated a trend towards improvement in RV ejection fraction in patients receiving angiotensin receptor blockers compared with control (WMD=1.11, 95% CI −0.02 to 2.26, p=0.06), but not in the respective comparison for ACE inhibitors (WMD=0.07, 95% CI −2.74 to 2.87, p>0.05). No differences were shown between the two groups with regard to maximal oxygen consumption, RV end-systolic volume, RV end-diastolic volume, duration of cardiopulmonary exercise testing, and resting and maximal heart rate. Mild adverse drug reactions were common but evenly distributed between the treatment and control groups. The current meta-analysis highlights that there may be a role for RAAS inhibition, particularly treatment with angiotensin receptor blockers, in those with or at risk of RV dysfunction. However, further confirmation will be required by larger prospective trials.
- heart failure
- pharmacology
- cardiac function
Statistics from Altmetric.com
Introduction
Right ventricular (RV) dysfunction is an independent predictor of mortality in several clinical settings.1–3 The pharmacological management of left ventricular (LV) failure is well established, using a combination of ACE inhibitors (ACEI),4 angiotensin receptor blockers (ARB),5 beta-blockers6 and aldosterone antagonists.7 However, there is a paucity of data for the management of RV failure.
As discussed in the most recent American College of Cardiology/American Heart Association guidelines on the management of heart failure in patients with congenital heart disease, ACEI, ARB and beta-blockers are routinely used in the management of RV dysfunction, but there is limited evidence to support their efficacy.8 The majority of randomised controlled trials (RCTs) and cohort studies published to date, including the recent Dutch multicentre trial REDEFINE,9 have been insufficiently powered to detect significant benefits of pharmacological intervention on RV failure.10–14 Nonetheless, several studies have reported a trend towards renin–angiotensin–aldosterone (RAAS) inhibition improving RV function in the context of ejection fraction (EF), fractional shortening and end-diastolic/systolic volumes. Furthermore, numerous trials have shown that certain subgroups among those with RV dysfunction do derive significant benefits from RAAS inhibition.9 10 14
Our systematic review and meta-analysis aims to compare the effect of RAAS inhibition versus no RAAS inhibition on RV function in those with or at risk of RV dysfunction, in order to establish significant support for the clinical use of ACEI and/or ARB in this population. Based on multiple previous studies favouring the usage of these agents without achieving significance, it was hypothesised that statistical synthesis of available data would show significant improvement in RV function with RAAS inhibition.
Methods
Literature search strategy
We followed the recommended guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Meta-Analysis of Observational Studies in Epidemiology. Electronic searches using Medline, PubMed, EMBASE, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews were initially performed on 27 September 2017, and subsequently updated on 9 December 2017 to include most recently published REDEFINE trial.9 To achieve the maximum sensitivity of the search strategy, synonyms and variations of the terms ‘right ventricular failure’, ‘right heart failure’, ‘angiotensin receptor blocker’ and ‘angiotensin converting enzyme inhibitor’ and all relevant generic drug names were combined as keywords or medical subject heading terms (online supplementary figure S1). In addition to these electronic searches, the reference lists of retrieved articles and relevant review articles were examined for additional relevant studies.
Supplemental material
Selection criteria
The current analysis included all studies examining the effect of RAAS inhibition on RV function in patients with or at risk of RV dysfunction. Patients were considered to be at risk of RV dysfunction if there was (1) increased afterload (eg, pulmonary hypertension or RV outlet tract obstruction); (2) increased volume load (eg, tricuspid regurgitation or pulmonary regurgitation); (3) ischaemia or infarction of the RV; (4) dilated cardiomyopathies; or (5) repaired or palliated congenital heart diseases that predisposed to supraphysiological pressure or volume load (eg, repaired tetralogy of Fallot (ToF) or single ventricle physiology with systemic RV). Studies were excluded if the patients had concomitant LV dysfunction in order to minimise potential confounding effects of RAAS inhibition on subsequent cardiopulmonary assessment. The location of each study was examined to ensure lack of duplication bias. No limits were set on language. Only full papers were included.
Data extraction and critical appraisal of evidence
Using full-text articles, data were independently extracted by two investigators (JYC and SYL). Disagreements were resolved by the senior author (SL), who also reviewed the synthesised data. The primary outcomes of interest were pretreatment and post-treatment differences in RV EF and maximal oxygen consumption (VO2 max) between the RAAS inhibition and control groups. Where difference in outcomes was not reported, the post-treatment measurement was taken as a surrogate. Clinical endpoints, such as hospitalisation or mortality, were not analysed due to insufficient reporting by the individual studies. If multiple measurements were performed in a single study, the final measurement was extracted to detect long-term changes. The secondary outcomes included RV end-systolic and end-diastolic volumes, resting heart rate (HR rest), maximal heart rate (HR max) and exercise duration. In addition, safety data including adverse clinical effects or changes in laboratory values were collated and analysed qualitatively. Demographic data including age, gender and New York Heart Association (NYHA) class were also extracted. Study quality was assessed using the Cochrane Risk of Bias Tool for RCTs or the Newcastle-Ottawa Quality Assessment Scale for observational studies. Where the patient served as his or her own control in before-and-after treatment study designs, the before was taken as the placebo control and the after as the treatment group.
Statistical analysis
Clinical outcomes were analysed using frequentist meta-analyses, with the weighted mean difference (WMD) used as the summary statistic. In the case of RV EF, which is reported in numerous studies both as post-treatment results and changes from baseline, two separate statistical analyses were performed to test the robustness of the summary outcome. In addition to pooled analysis of all studies, three subgroup analyses were performed to further qualify potential benefits of RAAS inhibition on RV EF: (1) ACEI versus ARB; (2) effect of RAAS inhibition in those with overt RV failure versus those at risk; and (3) RCTs versus observational studies. Further stratification by underlying diagnosis was not possible due to limited number of studies available in each category.
The I2 statistic was used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values greater than 50% considered as substantial heterogeneity. This, in turn, warranted use of a random-effect model; otherwise, a fixed-effect model was used. Sensitivity analysis was performed by leave-one-out analysis. Publication bias was assessed visually by funnel plots and statistically by Egger’s test using R V.3.4.2 software (R Foundation, Vienna, Austria). All other statistical analyses were carried out using Review Manager V.5.3 software (Cochrane Collaboration, Software Update, Oxford, UK).
Results
Quality assessment
The search results are shown in figure 1 in accordance with the PRISMA flow chart. A total of 12 studies were included for primary analysis, including six RCTs9–11 13–15 and six observational studies.12 16–20 All studies reported at least one primary outcome of interest, with nine reporting RV EF and ten reporting VO2 max. In total, there were 265 patients treated with RAAS inhibition and 265 placebo patients. A summary of the selected studies and baseline patient characteristics is presented in tables 1 and 2.
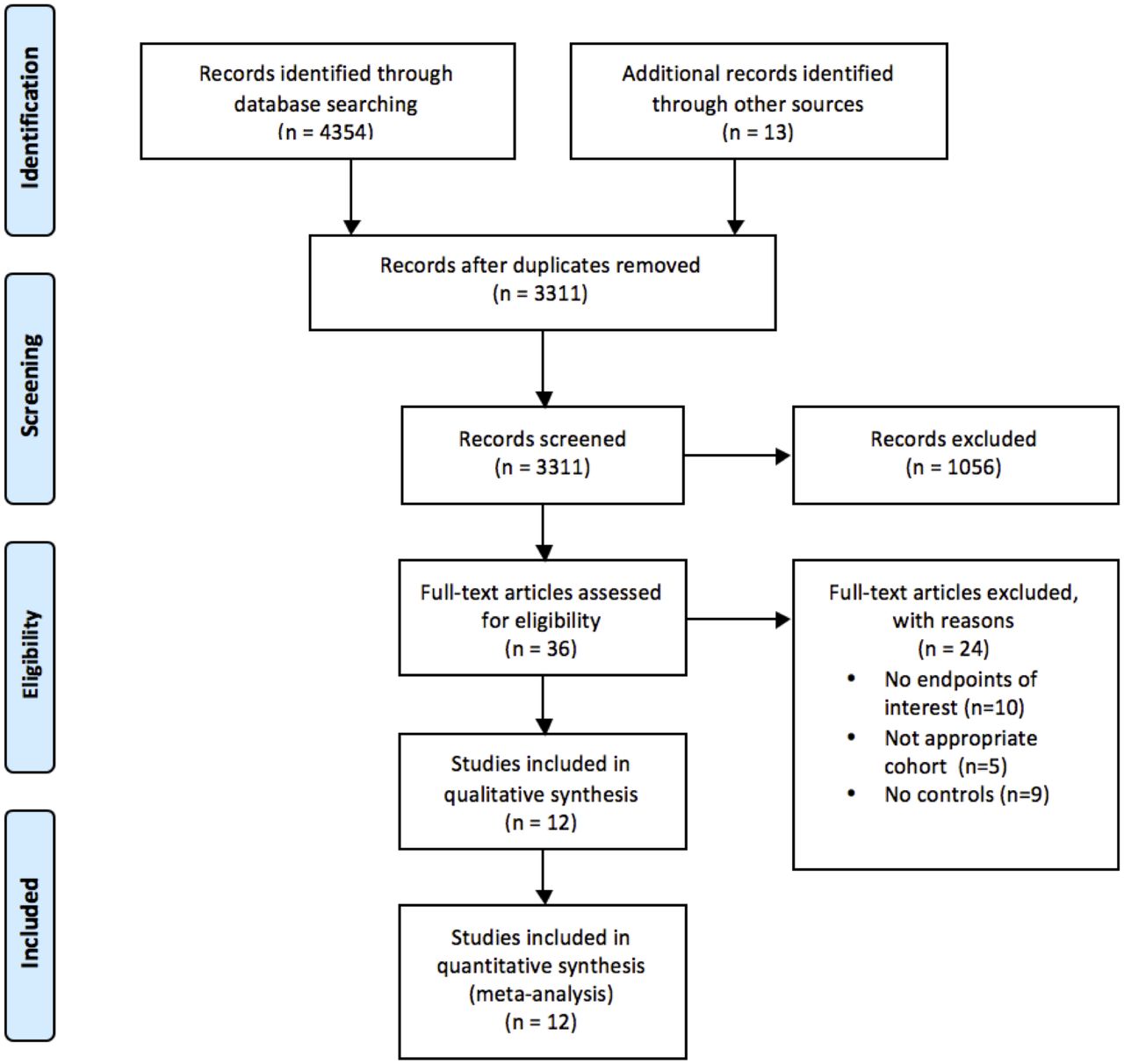
PRISMA flow diagram of studies included in data search. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary of study characteristics
Baseline patient characteristics
Bias assessment of RCTs using the Cochrane Risk of Bias Tool demonstrated that all RCTs were at low or unclear bias with regard to the primary endpoints (figure 2). The only exception was the RCT by Babu-Narayan et al,10 which did not account for attrition in the final analysis. Bias assessment of observational studies using the Newcastle-Ottawa Quality Assessment Scale demonstrated that all observational studies were of moderate to high quality (table 3).
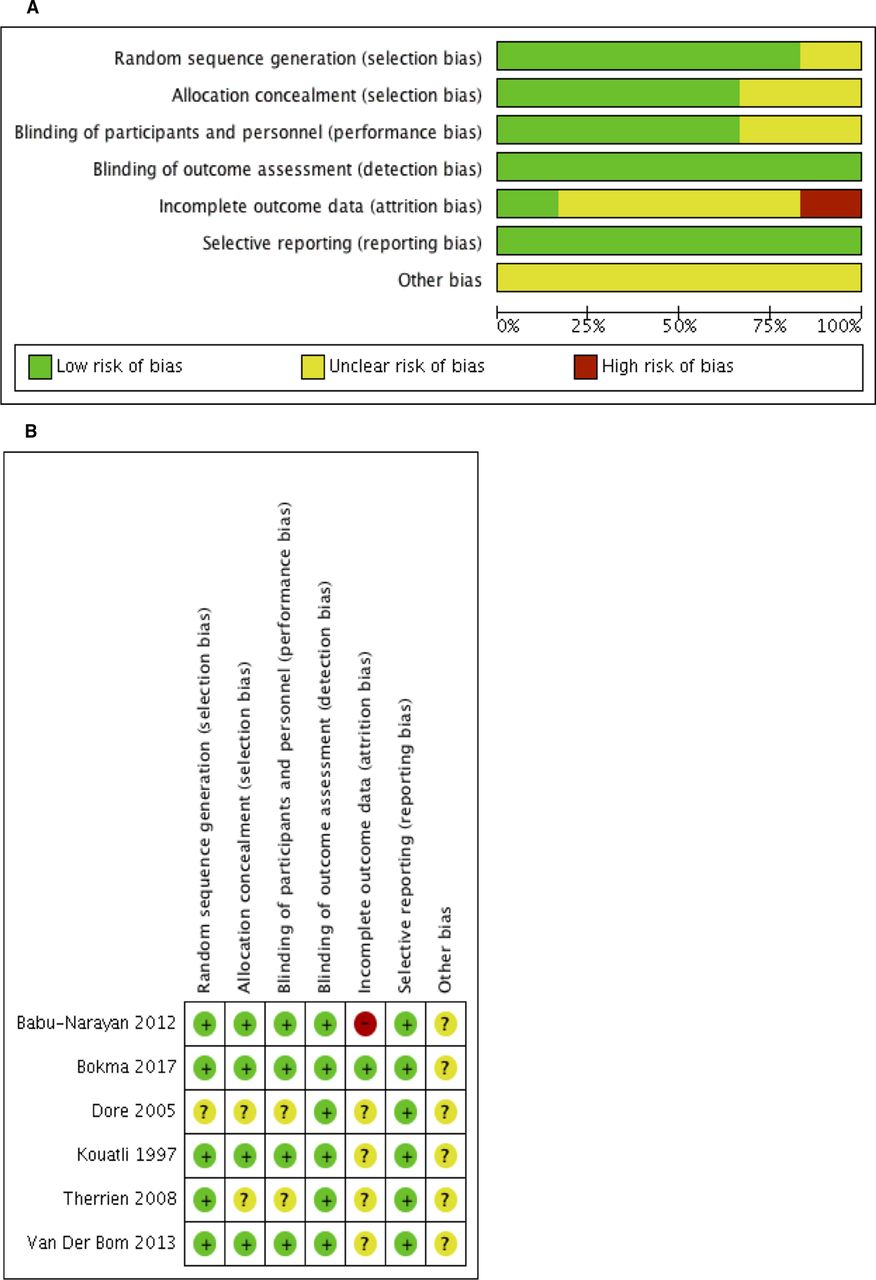
Risk of bias assessment of randomised controlled trials using the Cochrane tool, shown as (A) risk of bias graph and (B) risk of bias summary.
Assessment of selected observational studies using the Newcastle-Ottawa Quality Assessment Scale
Patient characteristics
Baseline statistics were comparable between the treatment and control groups including gender (65% vs 68% male, respectively), age (30.8 vs 30.7 years, respectively) and NYHA class (1.4 vs 1.2, respectively). There was a spectrum of underlying diagnoses that predisposed to RV dysfunction, including repaired ToF, single ventricle physiology with systemic RV and repaired transposition of the great arteries (table 1). The medical therapy included ramipril,10 13 enalapril,15 losartan9 11 and valsartan,14 accounting for 64 ACEI-treated and 147 ARB-treated patients.
Primary outcomes
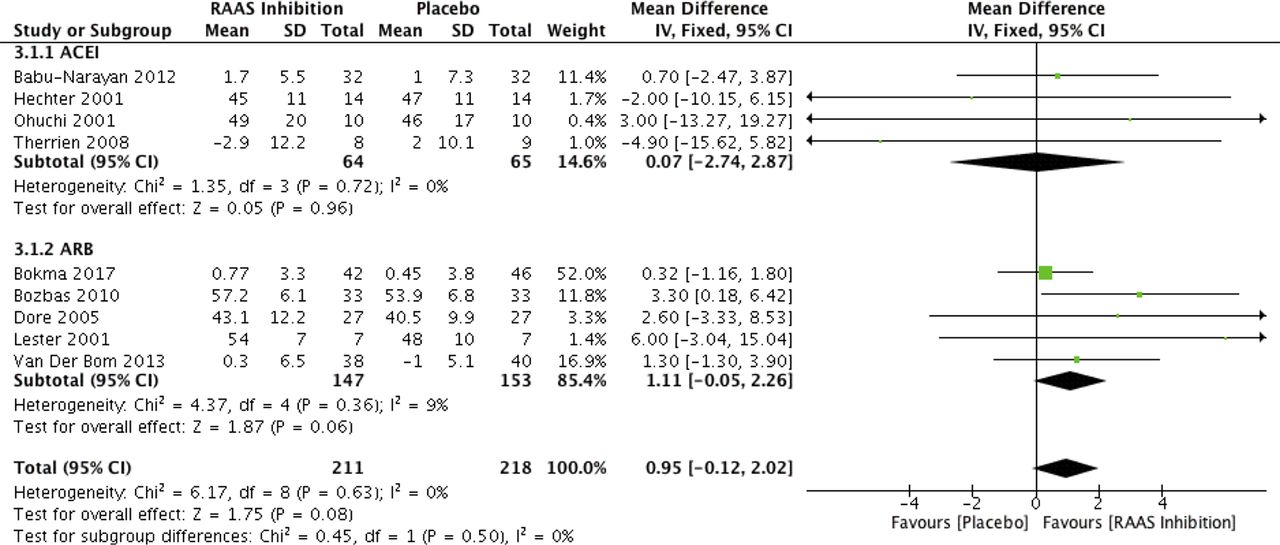
Of the nine studies that reported the outcome of post-treatment RV EF, four measured EF by echocardiography and five by cardiac MRI. There was a trend for improved RV EF in the treatment arm compared with the control arm (WMD=0.95, 95% CI −0.12 to 2.02, p=0.08; figure 3). On subgroup analysis, those treated with ARBs derived a trend towards improvement in RV EF compared with those patients given placebo (WMD=1.11, 95% CI −0.02 to 2.26, p=0.06; figure 3). However, the same pattern was not demonstrated for ACEI (WMD=0.07, 95% CI −2.74 to 2.87, p>0.05; figure 3). Subgroup analysis examining the effect of RAAS on overt RV failure versus those at risk revealed a significant benefit in those at risk of RV failure (WMD=1.64, 95% CI 0.1 to 3.19; p=0.04; online supplementary figure S2), but no benefit in those with overt failure (WMD=0.32, 95% CI −1.16 to 1.8, p>0.05; online supplementary figure S2). Subgroup analysis examining the difference between RCTs versus observational trials revealed a significant benefit of RAAS inhibition in the observational studies (WMD=2.94, 95% CI 0.21 to 5.67, p=0.03; online supplementary figure S3), but not in the RCTs (WMD=0.59, 95% CI −0.57 to 1.76, p>0.05; online supplementary figure S3).
Supplemental material
Supplemental material
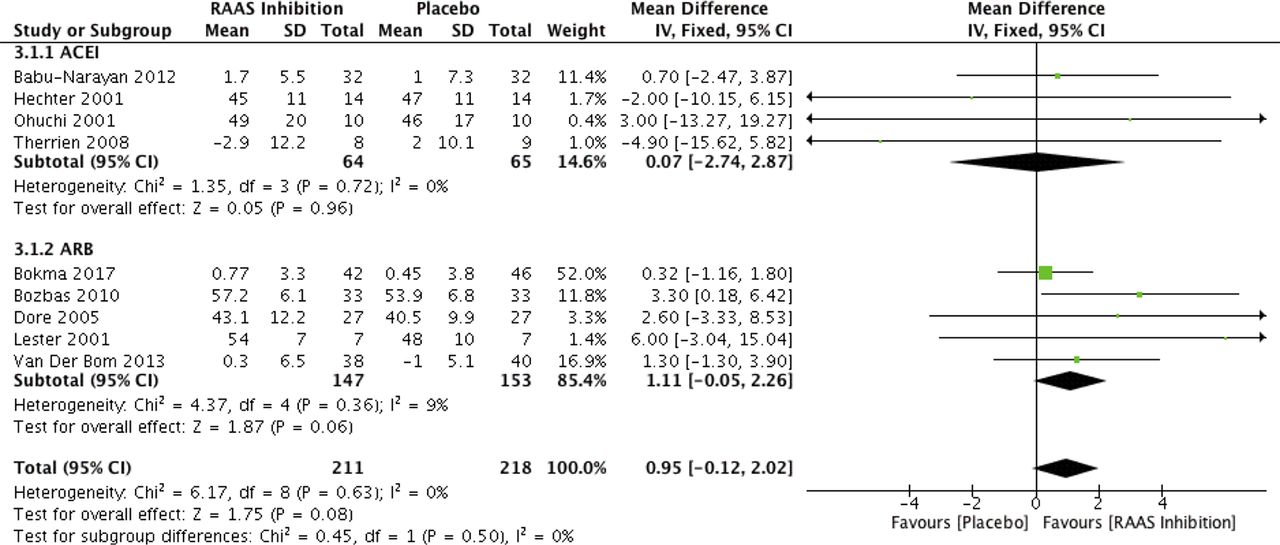
Right ventricular ejection fraction after RAAS inhibition in those with or at risk of right ventricular dysfunction. The results are further stratified by the selected agent (ACEI vs ARB). ACEI, ACE inhibitor; ARB, angiotensin receptor blocker; RAAS, renin–angiotensin–aldosterone system. IV, a random-effects meta-analysis is applied, with weights based on inverse variances.
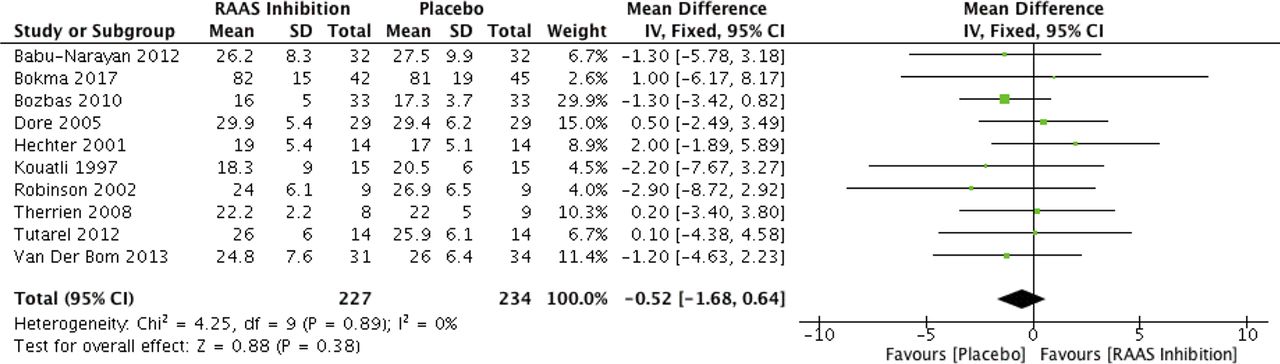
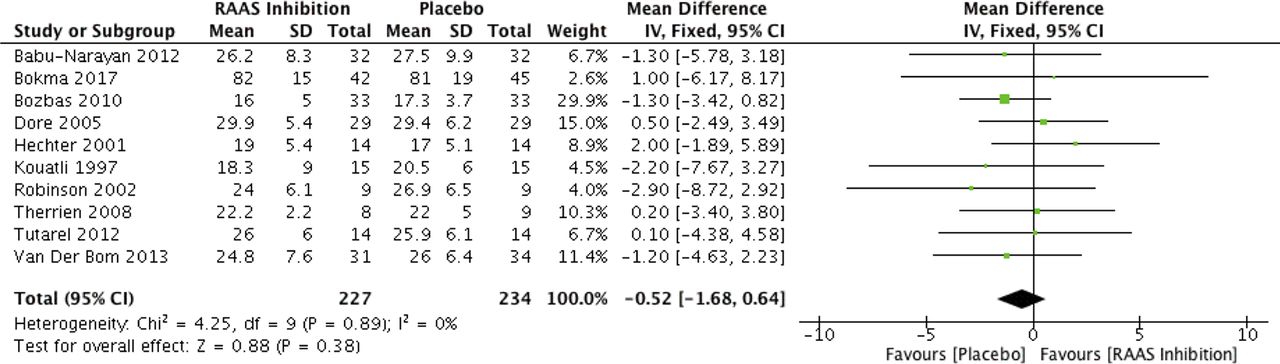
VO2 max was reported by 10 studies. Among these, two used treadmills and seven used cycle ergometer for exercise testing. VO2 max was not significantly different between the treatment and control arms (WMD=−0.52, 95% CI −1.68 to 0.64, p>0.05; figure 4). Subgroup analyses did not identify any difference in benefit between ACEI-treated and ARB-treated patients, nor between those with overt RV failure and those at risk.
![[heartasia-2018-010999-SP1.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
![[heartasia-2018-010999-SP2.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[heartasia-2018-010999-SP3.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Maximal oxygen utilisation after RAAS inhibition in those with or at risk of right ventricular dysfunction. I V , a random-effects meta-analysis is applied, with weights based on inverse variances; RAAS, renin–angiotensin–aldosterone system.
Secondary outcomes and safety outcomes
Treatment with RAAS inhibition was not associated with significant changes in RV end-systolic volume (WMD=−1.79, 95% CI −4.66 to 1.09, p>0.05) or end-diastolic volume (WMD=0.86, 95% CI −4.21 to 5.93, p>0.05). Exercise testing parameters including HR rest (WMD=1.59, 95% CI −2.9 to 6.09, p>0.05; online supplementary figure S4), HR max (WMD=−2.37, 95% CI −7.97 to 3.24, p>0.05; online supplementary figure S4) and duration of exercise (WMD=6.57, 95% CI −25.77 to 38.92, p>0.05; online supplementary figure S4) were not significantly different between the treatment and control arms.
Supplemental material
![[heartasia-2018-010999-SP4.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Safety outcomes were reported by most studies, including all six RCTs. Mild side effects from RAAS inhibition, including cough, dizziness, syncope and headache, were frequently noted but equally distributed between the control and treatment arms. Laboratory tests, such as electrolytes and renal function, were stable across all studies. Discontinuation of drug treatment due to side effects ranged from 0% to 20%, but again this was symmetrically distributed between both arms.
No heterogeneity was noted in the primary outcomes. Leave-one-out sensitivity analysis revealed no significant contribution of any single study towards the overall effect size. There was no publication bias in the primary outcomes as demonstrated by symmetrical funnel plots (online supplementary figures S5–S6). This was confirmed statistically by Egger’s test for both primary endpoints.
Discussion
RV dysfunction is strongly associated with increased mortality such as in postmyocardial infarction,1 left-sided heart failure2 and congenital heart disease.3 While the benefits of RAAS inhibition are well established for LV systolic dysfunction, its impact on right-sided heart failure is yet to be characterised.8 Our systematic review and meta-analysis is the first to analyse all available literature in this field. We demonstrated that RAAS inhibition results in a trend towards increased RV EF in patients with or at risk of RV dysfunction. This beneficial trend remained when we examined studies using ARBs only, but the same was not true for ACEIs. No changes in RV end-systolic or end-diastolic volume were seen between the treatment and control groups. Cardiopulmonary exercise testing parameters including VO2 max, exercise duration, and resting and maximal heart rate were also comparable between the treatment and control groups.
The current analysis revealed a trend towards improved RV EF among treated (RAAS inhibition) compared with control patients for the duration of follow-up. Previous trials examining the effect of RAAS inhibition on RV function have been scarce and often plagued by low cohort sizes, thereby producing non-significant or conflicting results.10 11 13 14 The very recent Dutch multicentre trial (Right vEntricular Dysfunction in tEtralogy of Fallot: INhibition of the rEnin-angiotensin-aldosterone system, REDEFINE) investigating the role of long-term treatment with losartan in 95 patients with repaired ToF and proven RV dysfunction found no treatment benefits in terms of RV EF, exercise capacity and N-terminal pro-brain natriuretic peptide.9 Likewise, a study of valsartan in adults with repaired transposition of the great arteries with systemic RV failed to identify any benefit of RAAS inhibition on RV function.14
In addition to low cohort numbers, another possible reason for the lack of treatment effect observed in the literature is that RAAS inhibition only produces benefits in certain groups with RV dysfunction. Consequently, the broad selection of patients in the previous studies may have masked any potential benefit in specific groups. van der Bom et al 14 showed that there was no benefit of valsartan treatment in a pooled cohort of patients with repaired transposition of the great arteries. However, there was a benefit in those patients with symptomatic right-sided heart failure, with both RV EF and VO2 max declining significantly in the control group compared with the treatment group.14 Previous RCTs have also shown benefits of RAAS inhibition in those with restrictive10 and non-restrictive RV physiology.9 Finally, it is possible that RAAS inhibition has a lesser role in RV failure due to intrinsic biological differences between the RV and LV, and their interactions with RAAS.21 22 In the current analysis, the benefit of the treatment failed to reach significance (p=0.08). This builds on the recent REDEFINE trial results, whereby in a broader group of patients with RV dysfunction there is still a lack of definitive evidence supporting the use of ACEI or ARB. The trend identified in the current analysis, however, should serve as impetus for further prospective trials sufficiently powered to detect clinically meaningful benefits.
Despite the lack of direct effect on RV EF by RAAS inhibition, previous studies have noted improvements in other parameters, which correlate with improvements in ventricular function. Babu-Narayan et al 10 found that treating patients with repaired ToF with 6 months of ramipril resulted in significantly increased RV long-axis shortening compared with controls. Improvements in NYHA class and exercise tolerance have also been reported.18 23 Furthermore, on biochemical testing, it has been shown that in a cohort of patients with repaired ToF with dilated RV, cilazapril produced a dose-dependent reduction in brain natriuretic peptide,24 which correlated with LV and RV dysfunction, in addition to being a useful clinical marker for risk stratification in left-sided heart failure.25 Reduced RV EF has also been associated with increased rate of arrhythmia,26 and future trials should seek to investigate potential benefits of RAAS inhibition on these events.
There are several limitations in our analysis. First, there are differences in the length of follow-up among the studies, varying from 10 weeks to 3 years. However, based on prior results demonstrating LV remodelling within 6–12 weeks of initiating RAAS inhibition,27 28 the current analysis satisfies the minimum follow-up requirements by extrapolation. Therefore, our results potentially underestimate the long-term improvements in RV function with RAAS inhibition. Second, despite all studies recruiting only patients with or at risk of RV dysfunction, the underlying diagnoses do vary and the impact of this should be further explored in future investigations. Third, four of the selected studies employed echocardiography to measure RV EF.11 12 16 18 Due to the asymmetrical geometry of the RV, the lack of standardised views in echocardiography can be unreliable compared with cardiac MRI.29 This could potentially mask significant treatment effects. Fourth, a small proportion of patients had relatively normal RV function at baseline. This would underestimate the effect of RAAS inhibition that we observed in our analysis since RAAS activation is more prominent in those with significant ventricular dysfunction.30 Finally, two of the included trials11 15 were crossover in design without adequate washout period between crossover, leading to potential confounding effects.
The current systematic review and meta-analysis demonstrates that there may be a role for RAAS inhibition, specifically treatment with ARBs, in those with or at risk of RV dysfunction. However, the trends observed in the current study should be confirmed by larger prospective trials.
Supplemental material
![[heartasia-2018-010999-SP5.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
Supplemental material
![[heartasia-2018-010999-SP6.jpg]](https://heartasia.bmj.com/content/heartasia/10/1/e010999/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Acknowledgments
None
References
Footnotes
Contributors JYC: data extraction, analysis and interpretation plus manuscript draft and critical revision. SYK and KP: data extraction and analysis DC: data interpretation and critical revision. SL: conception of study, data analysis and interpretation and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.