Article Text

Abstract
Purpose The ratio of the left atrial volume index (LAVI) and late diastolic mitral annular velocity (A′) is a useful echocardiographic index for identifying advanced left ventricular (LV) diastolic dysfunction in patients with dyspnoea. We investigated the clinical implications and prognostic value of the aforementioned ratio (LAVI/A′) in patients with ST elevation (STE) or non-STE (NSTE) acute coronary syndrome (ACS).
Methods We studied 212 patients with ACS. All patients underwent electrocardiography, echocardiography and measurement of plasma B-type natriuretic peptide (BNP) level on admission. The study endpoints were hospitalisation and mortality because of heart failure (HF).
Results There was a significant, moderate positive correlation between LAVI/A′ and natural logarithm (Ln) BNP level among the participants (r=0.48, p<0.0001). During a mean follow-up of 17 months, eight patients died and nine patients were hospitalised because of HF. The receiver operating characteristics curve indicated that LAVI/A′≥3.0 predicted these events (log-rank, p=0.0021). A significant and moderate positive correlation existed between LAVI/A′ and Ln BNP level in the NSTE-ACS group (n=128; r=0.58, p<0.0001). However, the correlation between LAVI/A′ and Ln BNP level was weaker in the STE-ACS group (n=84; r=0.33, p=0.0017).
Conclusion LAVI/A′ was related to plasma BNP levels in patients with ACS, particularly in those with NSTE-ACS. This index was useful for predicting cardiac events in patients with ACS.
- cardiac function
- diastolic dysfunction
- coronary artery disease
Statistics from Altmetric.com
Introduction
Left ventricular (LV) diastolic dysfunction has been shown to be related to cardiovascular events,1 2 with left atrial (LA) size being linked to LV diastolic dysfunction and elevated LV filling pressure.3–5 The LA volume has been accepted to be a stable indicator that reflects the duration and severity of LV diastolic dysfunction.6 The LA volume is useful for monitoring cardiovascular risk and for guiding therapy.6 In addition, an increased LA volume index (LAVI) has been shown to be a powerful predictor of mortality after acute myocardial infarction (AMI).7 8 In a recent study,9 LAVI had similar predictability as LV ejection fraction (EF) for heart failure (HF) hospitalisation and mortality in ambulatory adults with coronary artery disease (CAD).
Late diastolic mitral annular velocity (A′), which is measured by tissue Doppler imaging (TDI), has been shown to be a relatively preload-independent variable for evaluating LV diastolic function.10 In patients with decreased LV function, A′ can be used to assess LA function, particularly LA systolic function.11 12 Reduced A′ velocity is a predictor of cardiac death, suggesting an important role for compensatory LA booster pump function.13 The LA volume progressively increases2 and A′ velocity decreases12 14 as the LV diastolic dysfunction advances. Park et al 15 reported that the LAVI/A′ ratio was a useful parameter for identifying advanced LV diastolic dysfunction and predicting clinical outcomes in patients with dyspnoea.
On the other hand, both LV systolic and diastolic functions, as evaluated using echocardiography, can effectively predict cardiovascular events in patients with acute coronary syndrome (ACS).16 17 Moreover, approximately 70% of patients with ACS are classified under non-ST elevation ACS (NSTE-ACS) and long-term outcomes for these patients are worse for up to 10 years after the event. Several factors are related to this, including an increased prevalence of multivessel disease, a greater likelihood of residual ischaemia and the presence of comorbidities such as diabetes and chronic kidney disease.18 19
In this study, we aimed to investigate the clinical implications and prognostic value of the LAVI/A′ ratio in patients with ST elevation (STE) ACS and NSTE-ACS. We also examined how this echocardiographic index correlated with the B-type natriuretic peptide (BNP) levels and pulmonary artery wedge pressure (PAWP).
Methods
Participants
We studied 671 consecutive patients diagnosed with ACS who were admitted to the coronary care unit of our hospital between January 2006 and May 2008. All patients underwent electrocardiography (ECG) and echocardiography, including TDI on admission, and we excluded patients with atrial fibrillation, atrial flutter or significant valvular abnormalities. Patients were eligible for inclusion if they had AMI or unstable angina pectoris (n=212; mean (SD) age, 65 (12) years; 166 men). Pulmonary artery catheters were indwelt in 46 patients.
All patients were informed of the purpose and methods of the study in detail, and they provided written informed consent.
Echocardiography
At a median of 1 day (range, 0–5 days) after admission, transthoracic echocardiography was performed using commercially available ultrasound equipment (Sonos 5500; S3 probe; Philips Medical Systems, Andover, Massachusetts, USA). The LV volume was measured at both end systole and end diastole by the biplane modified Simpson’s method with apical 4-chamber and 2-chamber views, and the LV ejection fraction (LVEF) was calculated. Subsequently, the LV end-diastolic dimensions, LV end-systolic dimensions, interventricular septal dimensions and LV posterior wall dimensions were measured from a parasternal long-axis view using conventional two-dimensional measurements.
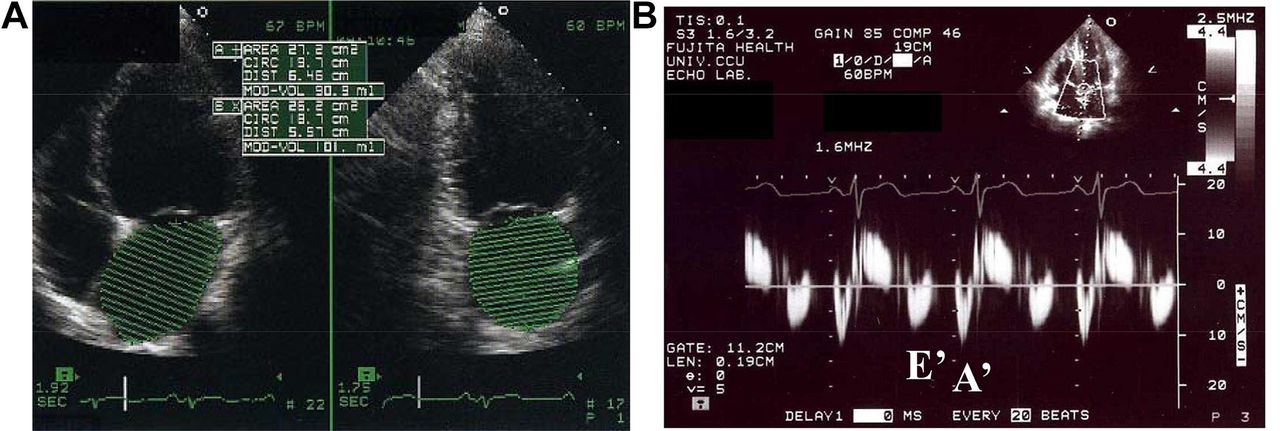
The peak velocities of early (E) and late (A) diastolic filling, E/A ratio and E-wave deceleration time were derived from pulsed wave Doppler recordings of mitral inflow. The LA volume was assessed using the biplane Simpson’s method from apical 4-chamber and 2-chamber views in end systole. LAVI was obtained by correcting for body surface area. Peak early (E′) and late (A′) diastolic mitral annular velocities were acquired at the septal site of the mitral annulus using TDI from an apical 4-chamber view (figure 1). The E/E′ and LAVI/A′ ratios were calculated.

A method of left atrial volume measurement (A) and measurement of mitral annular velocity by Doppler tissure imaging (B).
Electrocardiogram
All participants underwent 12-lead ECG on admission (FDX-4520LA, Fukuda Denshi, Tokyo, Japan). Patients with STE at the J point in two or more consecutive leads (with the cut-off point >0.2 mV in lead V1, V2 or V3 and >0.1 mV in the other leads) were defined as having STE-ACS. Patients with ST-segment depression, T-wave inversion or no ECG abnormalities were defined as having NSTE-ACS.
Plasma BNP and serum creatine kinase
After blood was drawn from the antecubital veins or femoral arteries, it was added to tubes filled with ethylenediaminetetraacetic acid for measuring the BNP levels and in plain tubes for measuring the creatine kinase (CK) levels. The tubes were then centrifuged, and the separated plasma or serum was frozen at (–)80°C until analysis. The BNP level was measured by chemiluminescence enzyme immunoassay, and the CK level was measured by an ultraviolet test.20
Pulmonary artery wedge pressure
After informed consent was obtained from appropriate patients, right heart catheterisation was performed using a 7.5-French gauge, flow-directed Swan-Ganz catheter, which was introduced through a femoral vein.
Clinical assessment and end points
Follow-up clinical information was collected by a review of medical records. The primary study end points were mortality and rehospitalisation because of HF.
Statistical analysis
Continuous variables are presented as mean±SD. Differences in the baseline characteristics between groups were determined using the Student’s t-test for continuous variables and the Χ2 test for dichotomous variables. Correlations between the LAVI/A′ ratio and natural logarithm (Ln) BNP levels as well as PAWP were assessed by linear regression analysis. Multivariate proportional hazard models were used to detect the predictors of the predefined end points. The area under the receiver operating characteristics (ROC) curve (AUC) was used to evaluate optimal cut-offs for selected outcome predictors, and predictive values were calculated. Event-free survival curves were generated using the Kaplan-Meier method, and the differences between the groups were analysed using the log-rank test. Statistical significance was defined as a p value of <0.05. We used JMP (V.8.0 for Windows, SAS, Cary, North Carolina, USA) for all statistical analyses.
Results
Correlation with clinical outcomes
During a mean follow-up at 17 (range, 0–35) months, eight patients died and nine patients were rehospitalised because of HF. Univariate predictors of the composite end points are presented in table 1. LVEF and peak E′ velocity were significantly reduced in patients with an endpoint, whereas age and the LAVI/A′ ratio significantly increased in these patients. ROC analysis revealed that an LAVI/A′ ratio of ≥3.0 was the optimal cut-off for predicting mortality and rehospitalisation because of HF in all participants (AUC=0.61, p<0.05; sensitivity and specificity, 52.9% and 80.5%, respectively).
Univariate predictors of the composite end point of mortality and HF rehospitalisation
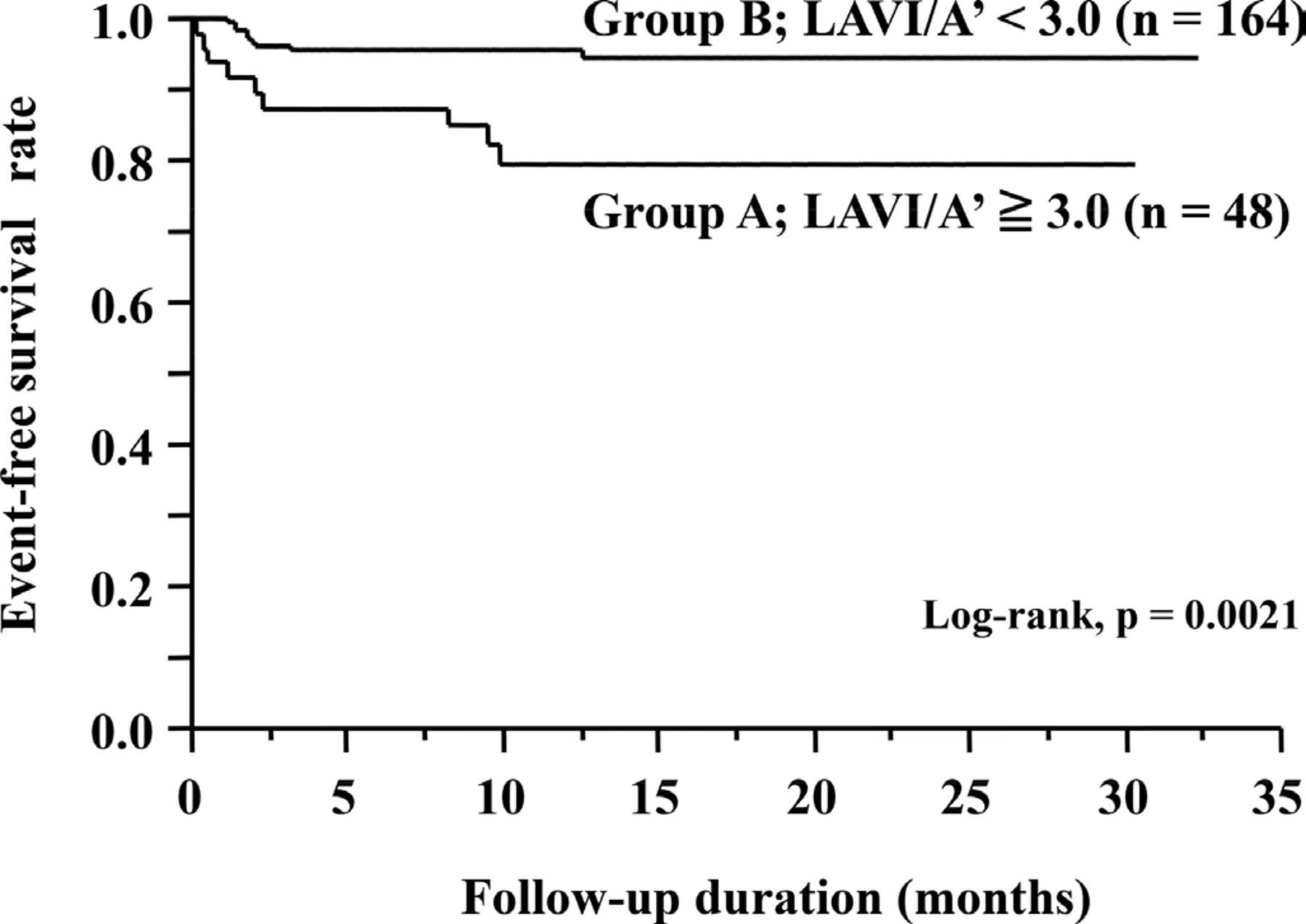
Patients were classified into two groups according to the LAVI/A′ ratio: Group A, with a LAVI/A′ ratio of ≥3.0 (n=48) and Group B with a LAVI/A′ ratio of <3.0 (n=164). The clinical characteristics and echocardiographic parameters for each group are shown in tables 2 and 3. The Kaplan-Meier survival curves for Groups A and B are shown in figure 2. The incidence of events was significantly higher in Group A (log-rank, p=0.0021). The multivariate proportional hazards analysis showed that the LAVI/A′ ratio was an independent and strong predictor of mortality and rehospitalisation because of HF (HR, 5.32; 95% CI 1.50 to 18.92; p=0.0104) (table 4).
Clinical characteristics in patients with LAVI/A′≧3.0 and with LAVI/A′<3.0 in all the subjects
Echocardiographic parameters in patients with LAVI/A′≧3.0 and with LAVI/A′<3.0 in all the subjects

Kaplan-Meier plot of survival free from mortality and HF rehospitalization.
Multivariate proportional hazards analysis predict of mortality and HF rehospitalisation
Correlations of the LAVI/A′ ratio with Ln BNP
There was a significant and moderate positive correlation between Ln BNP and the LAVI/A′ ratio among all participants (r=0.49, p<0.0001) (figure 3A); however, the correlation between the LAVI/A′ ratio and Ln BNP was stronger in the NSTE-ACS group (r=0.58, p<0.0001) (figure 3B) than the STE-ACS group (r=0.33, p=0.0017). There was also a significant positive correlation between the LAVI/A′ ratio and the PAWP result (r=0.30, p<0.0001) (figure 4).

Correlation between LAVI/A’ with Ln BNP.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between LAVI/A’ with PAWP.
Discussion
Although the LAVI/A′ ratio has previously been reported to be useful in detecting advanced LV diastolic dysfunction and predicting the prognosis in patients hospitalised with dyspnoea,15 this is the first study to show its clinical usefulness in patients with CAD. In particular, the LAVI/A′ ratio had a significant positive correlation with Ln BNP, indicating an increase in the LAVI/A′ ratio being associated with higher BNP levels.
BNP is released from the cardiac ventricles in response to myocyte stretching, and an elevation of LV diastolic pressure can increase the plasma BNP levels.21 After an AMI, elevated BNP concentrations identify patients at risk for adverse LV remodelling, LV dysfunction, HF and death, independent of age and history of HF and LVEF. Even in patients with unstable angina and no evidence of myocardial necrosis or HF, increased concentrations of BNP are associated with an increased risk of death.22 Given that BNP had a significant correlation with LV end-diastolic pressure, the LAVI/A′ ratio should increase as the LV end-diastolic pressure increases.
In this study, patients in the NSTE-ACS group had a stronger correlation with Ln BNP compared with those in the STE-ACS group. This may be explained by the fact that NSTE-ACS is more likely to occur in the setting of chronic repetitive episodes of arterial occlusion with platelet embolisation. However, STE-ACS is a result of more acute myocardial injury; therefore, the LAVI/A′ ratio may not necessarily change in parallel with the BNP levels in patients with STE-ACS. Consequently, the LAVI/A′ ratio was more correlated with Ln BNP in the NSTE-ACS group.
According to Park et al, a LAVI/A′ ratio of 4.0 was the best cut-off value for identifying advanced diastolic dysfunction.15 In contrast, we showed a lower optimal cut-off value of 3.0 for predicting cardiac events in patients with CAD. This difference may have resulted from the fact that there was no record of the aetiology of dyspnoea in the study by Park et al and that they could have included patients with a wider range of heart diseases. We consider it to be reasonable to have different cut-off values for the LAVI/A′ ratio among heart diseases and recommend that the LAVI/A′ ratio of 3.0 quoted in this study be taken in the context of our population. Further research will be needed to confirm our assertions in prospective studies.
The correlation between the LAVI/A′ ratio and PAWP was weak. This is consistent with the previous observation that the LAVI/A′ ratio may be potentially useful in the diagnosis of chronic diastolic dysfunction, whereas PAWP represents a more acute stage of elevated LV filling pressure.15
LA is exposed to LV filling pressures through the open mitral orifice during diastole; therefore, its size is influenced by the same factors that determine the diastolic filling pressure. When LV diastolic dysfunction becomes evident, the LA pressure increases to maintain adequate filling,23 and the increased atrial wall tension leads to stretching of the atrial myocardium and chamber dilatation. Therefore, the LA volume reflects the long-term exposure of the left atrium to abnormal LV diastolic function and filling pressure,5 and the LAVI itself is a stable indicator of LV diastolic function. However, LAVI is simply a manifestation of structural information, regardless of its function. In this study, LAVI was not shown to be a significant predictor of cardiac events, despite including participants without LA dilatation even among those with cardiac events, who were not considered to have severely damaged LV diastolic function. Finally, although LAVI is derived from simple morphological information, A′ reflects LA function. Thus, the LAVI/A′ ratio offers an effective measure for predicting LV diastolic dysfunction by combining both structural and functional data to detect subtler changes in LV diastolic dysfunction, particularly in patients with relatively preserved diastolic function.
The magnitude of A′ has been shown to be altered by age.24–26 However, previous studies were performed in healthy participants, and in this study of patients with ACS, there was no correlation between A′ and age. This is consistent with the evidence by Abe et al,27 who showed that a decreased A′ can result from significantly decreased functional reserves in the pulmonary venous system, from LA pump dysfunction or from a significant elevation in the LA pressure.
It is well known that the E/E′ ratio can be used to estimate PAWP and that there is a strong relationship between the two variables.28 29 The E/E′ ratio is also a powerful predictor of survival after AMI, with one report showing that a value of >15 predicts decreased survival.16 However, we did not find the E/E′ ratio to be a significant predictor, possibly because too few patients had an elevated E/E′ ratio (E/E′,>15) in this study. Although the clinical significance of mild elevations in the E/E′ ratio (ie, 8<E/E’<15) remain unclear,30 we think that the LAVI/A′ ratio provides a useful indicator of outcomes in patients without an elevated E/E′ ratio (ie, with an E/E′ ratio of <15).
Limitations
This study has several limitations. First, patients with atrial fibrillation, atrial flutter or significant valvular abnormalities were excluded. It is possible that many of these patients had LA dilatation regardless of the LV filling pressure. In addition, because A′ is produced by atrial contraction, it is absent in atrial fibrillation. Second, patients in this study were undergoing medical treatment at an intensive care unit where it is sometimes difficult to acquire good image quality because of either the use of respirators or postural limitations. It is not possible to obtain accurate LAVI values from poor quality images. Third, the number of patients may be insufficient to provide an accurate ROC analysis or true predictive values. Finally, it is important to note that this was only an initial study to demonstrate the usefulness of the LAVI/A′ ratio for predicting mortality and hospitalisation because of HF in patients with ACS. Further prospective studies with larger samples will be needed to confirm our findings.
Conclusion
The LAVI/A′ ratio is available as a new echo index which reflects LV chronic diastolic function in patients with ACS. It can predict mortality and rehospitalisation because of HF particularly in those with NSTE-ACS. An increase in the LAVI/A′ ratio suggests that the PAWP and BNP levels are elevated.
Key questions
What is already known about this subject?
Left atrial volume index (LAVI)/A′ is reported to be a useful echo parameter to identify advanced diastolic dysfunction in patients with dyspnoea.
What does this study add?
We showed that LAVI/A′ is also a helpful index in patients with acute coronary syndrome (ACS), particularly in those with non-ST elevation ACS (NSTE-ACS).
How might this impact on clinical practice?
LAVI/A′ ratio may help predict mortality and rehospitalisation because of heart failure particularly in patients with NSTE-ACS, because we found that an increase in LAVI/A′ indicated elevation in pulmonary artery wedge pressure and B-type natriuretic peptide levels, reflecting left ventricular diastolic dysfunction.
Acknowledgments
We thank Yoshimi Ohira, Ayako Takahashi, and Hideko Menjo, who are sonographers in the Emergency Medical Center in our hospital, for their devotion to the collection and assembly of the data used in this study.
References
Footnotes
Contributors HM and AY designed the study, analysed and interpreted the data and wrote the manuscript; KuS and KeS performed the experiments and collected the data. MI, TI, JI and YO reviewed and provided critical input for the manuscript. All authors contributed to writing the manuscript and gave final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.