Article Text

Abstract
A 53-year-old man presented with chest pain, palpitations and presyncope, without history of overt cardiac disease. The patient was alert. His heart rate was 206 beats per minute, and his blood pressure was 100/50 mm Hg. An intravenous bolus of amiodarone 150 mg was administered in the emergency department. His ECGs preamiodarone and postamiodarone are shown in figure 1. Echocardiography showed low-normal left ventricular systolic function.

(A) ECG of index arrhythmia. (B) ECG following amiodarone.
Question What should the next diagnostic test be?
Referral for electrophysiology study.
Referral for urgent coronary angiography.
12-lead ECG with posterior lead placement.
Bedside adenosine challenge.
- Broad complex tachycardia
- adenosine
Statistics from Altmetric.com
Answer: D
The differential diagnosis of broad QRS complex tachycardia includes ventricular tachycardia (VT), supraventricular tachycardia (SVT) with aberrancy and pre-excited tachycardia. There are several published algorithms for distinguishing SVT from VT, such as the frequently used ‘Brugada algorithm’.1 In this case, SVT with aberrancy is unlikely with the duration of QRS being >140 ms, monophasic R wave in V1 and R:S ratio <1 in V6.
However, differentiating pre-excited tachycardia from VT is challenging because the accessory pathways usually join the atrium to the ventricle at the level of the atrio-ventricular annulus, and thus pre-excited tachycardias may mimic VT originating from the base of the ventricle. Documentation of atrio-ventricular (AV) dissociation (eg, more QRS complexes than P waves or presence of capture/fusion beats) is the most reliable way to distinguish these arrhythmias.1
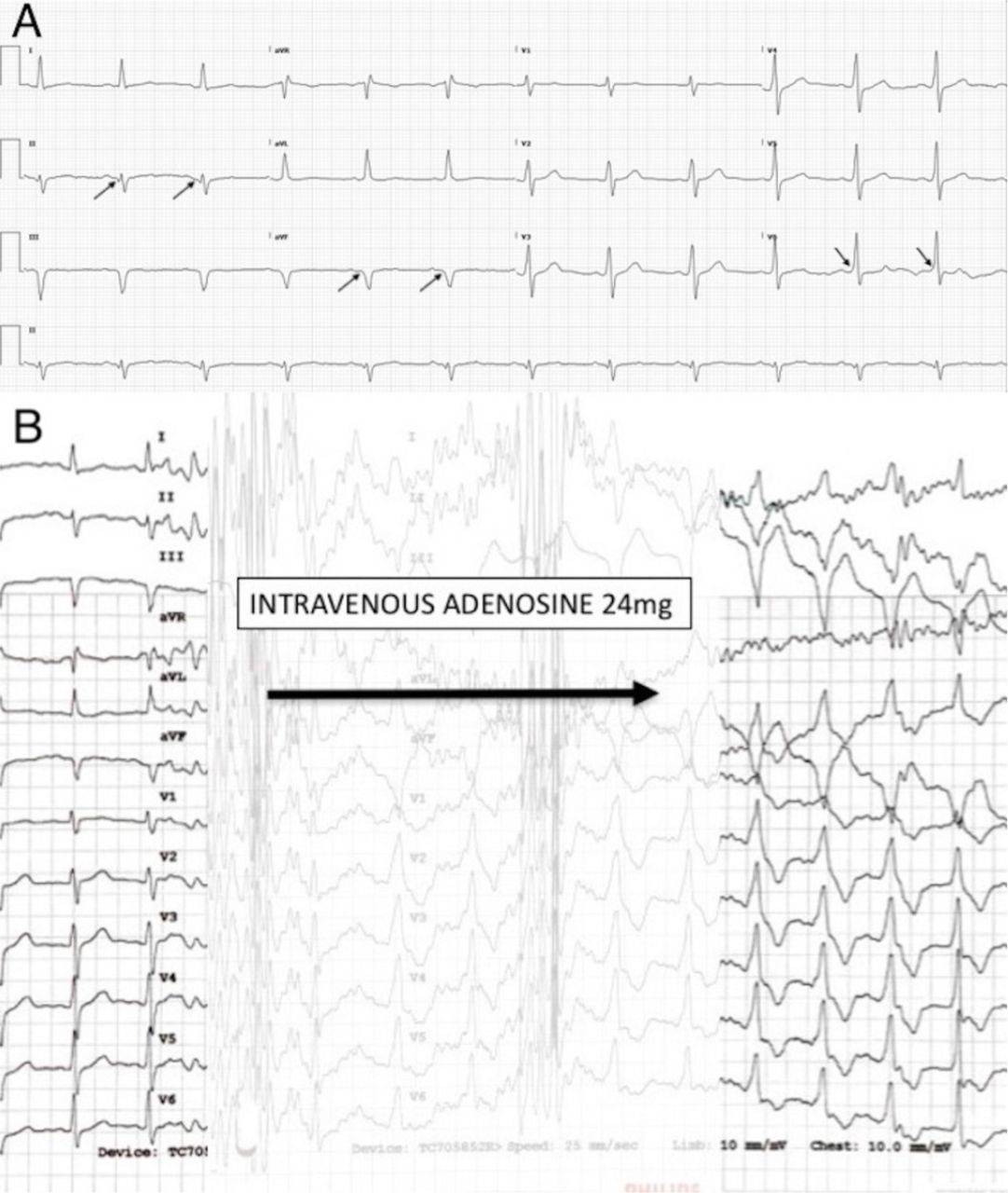
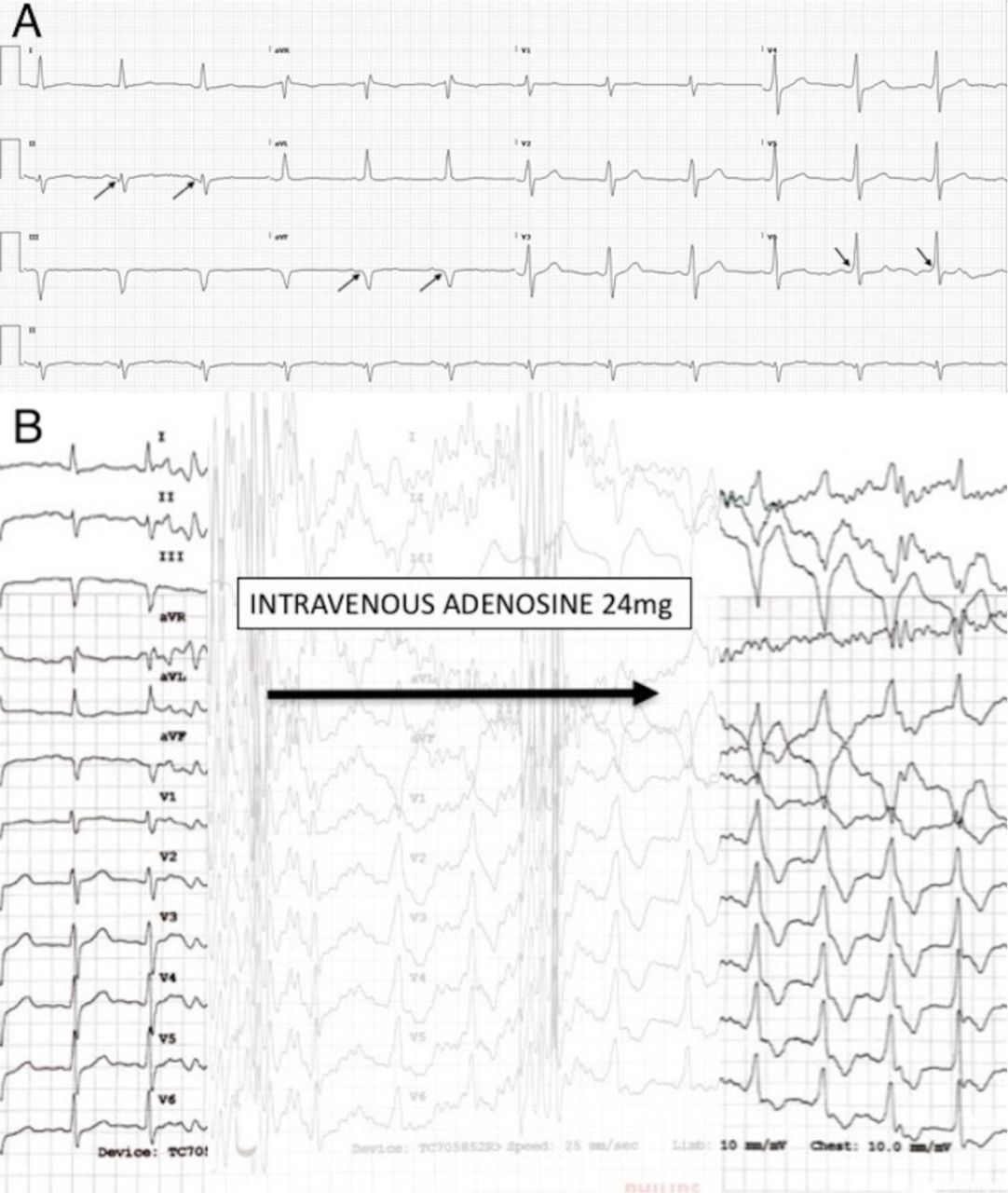
In this case, careful examination of the ECG in sinus rhythm reveals subtle slurring of the initial QRS complex, suggesting possible pre-excitation (figure 2A). Moreover, the axis of the presumed delta wave is concordant with the axis of the QRS complex during tachycardia, being superiorly directed and positive in V1. In this setting, an adenosine challenge is a cheap bedside diagnostic test which should be considered prior to more invasive investigations such as an electrophysiology study (answer A).
{kind=link}
{kind=link}
(A) Baseline ECG. Arrows point to the delta waves. (B) Rhythm strip during adenosine challenge. Arrow shows administration of adenosine.
Following adenosine administration, there was manifest pre-excitation with the QRS morphology approximating that seen during the index arrhythmia (figure 2B). An accessory pathway in the left posterior mitral annulus was confirmed at an electrophysiology study and ablation was successfully performed.
Coronary angiography (answer B) was not required once the diagnosis of pre-excited tachycardia was confirmed. Posterior lead ECG (answer C) was not required as posterior myocardial infarction was not suspected.
Footnotes
Contributors NRI, AWGJO and RWS designed the image challenge vignette, question and answer. NRI and RWS drafted the article. NRI, AWGJO and RWS critically revised the article. NRI and RWS revised the article in response to reviewer comments. NRI, AWGJO and RWS provided final approval of the version to be published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.