Article Text

Statistics from Altmetric.com
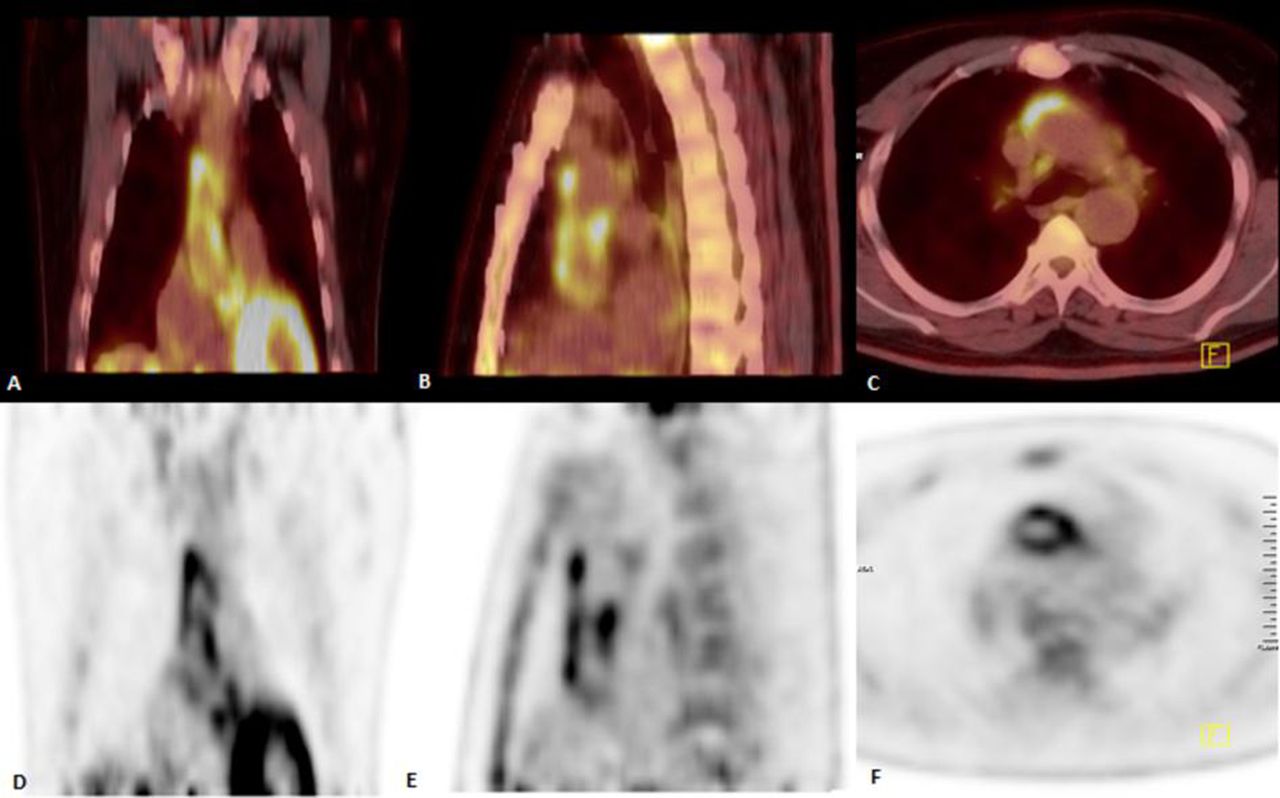
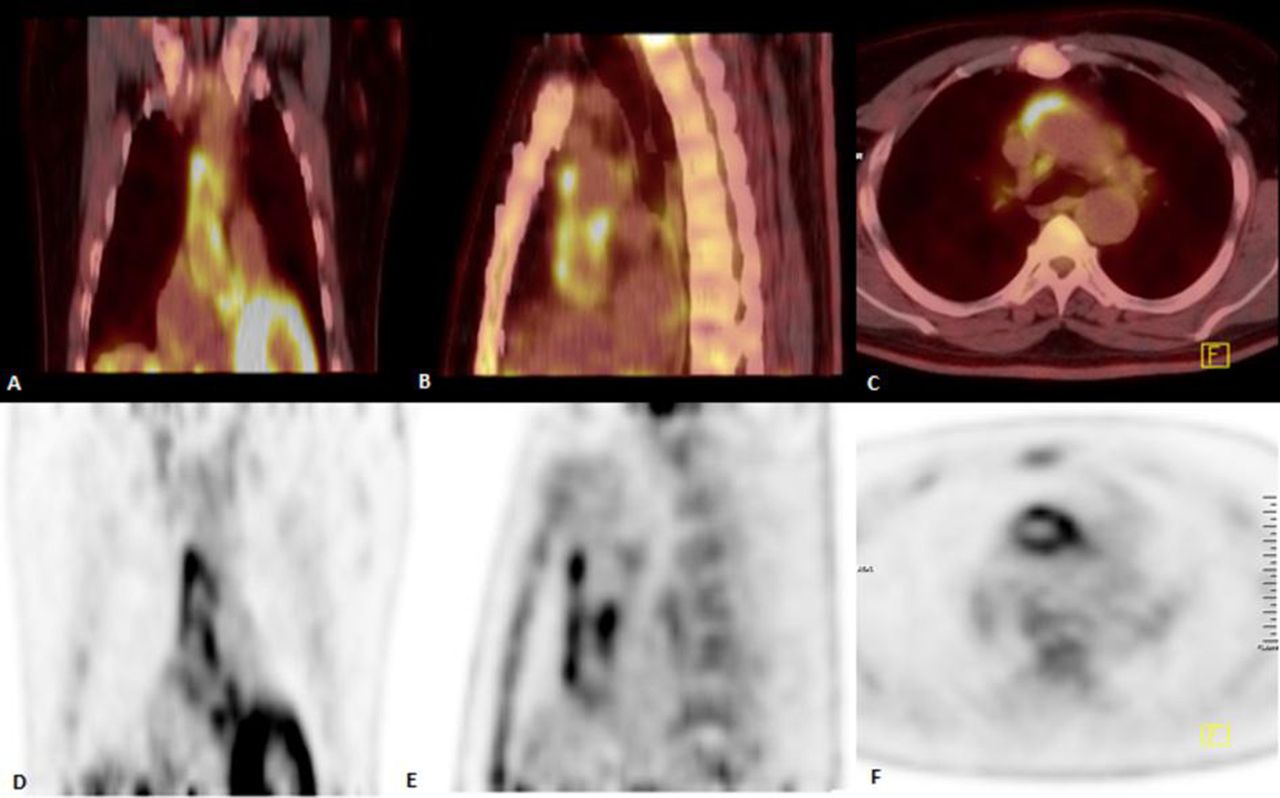
A 59-year-old man was admitted for fever of unknown origin. Fever was associated with chills. His medical record revealed the history of aortic valve replacement 11 years earlier, as well as enterococcal endocarditis 4 months prior to the current admission. The patient was found to have normal left ventricular size with borderline systolic function, left ventricular hypertrophy, right ventricle at the upper limit of normal size, mild systolic dysfunction and mild transvalvular aortic insufficiency on transthoracic echocardiography; while no vegetations were observed on transesophageal echocardiography. Sequential blood cultures were negative; however, a blood culture sample obtained 5 days prior to last admission was shown to be positive for enterococci. In addition, persistently increased levels of erythrocyte sedimentation rate and C reactive protein at 48 mm/hour and 39 mg/L were noted, respectively. Subsequently, the patient underwent fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-18 FDG-PET/CT) in search for the origin of the fever, which depicted increased radiopharmaceutical uptake in the aortic root with upward extension to the ascending aorta (figure 1), without any abnormal uptake of the prosthetic aortic valve in the non-attenuation corrected images. Rest of the whole body scan was unremarkable. Based on scan pattern, compatible with aortitis, the patient underwent antibiotic treatment with ampicillin/sulbactam. Fever immediately disappeared, and the inflammatory parameters as we all as patient’s clinical situation improved. The patient is currently receiving antibiotics to fulfil the 8 weeks duration.
{kind=link}
A 59-year-old man referred for fever of unknown origin following aortic valve replacement. Coronal (A), sagittal (B) and axial (C) hybrid F-18 FDG PET/CT images together with coronal (D), sagittal (E) and axial (F) F-18 FDG PET views demonstrate increased metabolic activity in the aortic root with upward extension to the ascending aorta, which is mostly consistent with vasculitis.
Multiple imaging modalities, providing different and often complementary findings among a wide array of aortitis presentations and potential complications, are used in the evaluation of both inflammatory and non-inflammatory aortic diseases. Inflammatory cell infiltration of different levels of aortic wall, caused by various immunological, infectious or traumatic factors, as the presenting cause of aortitis, is the rationale for nuclear imaging including F-18 FDG PET, which applies the metabolic accumulation of F-18 FDG in the inflammatory milieu, mainly in monocytes. Limited spatial resolution of PET and its inability to provide precise anatomic characterisation warrant coregistration of CT or MRI for anatomic localisation. Inconclusive CT findings in the early stages of aortitis indicate the need for a more sensitive modality.1 PET is known to be the most sensitive test for detection of the early vessel inflammation.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Not required.
Contributors AE-A and ME were involved in the clinical management of the patient. SH drafted and AE-A and ME revised the manuscript.