Article Text

Abstract
Objective Our objective was to assess the relations between apparent temperature and incidence of acute coronary syndrome (ACS) in Rasht, Iran.
Methods We used a time-series analysis to investigate the relationship between apparent temperature and hospital admission from 2005 to 2014. Distributed lag non-linear models were used to estimate the association between ACS hospitalisation and apparent temperature. To examine the high-temperature effect on ACS hospital admission, the relative risk of ACS hospital admission associated with high temperature, the 99th percentile of temperature (34.7°C) compared with the 75th percentile of temperature (26.9°C), was calculated. To assess the cold effect on ACS hospital admission, the relative risk of ACS hospital admission associated with cold temperature, the first percentile of temperature (−0.2°C) compared with the 25th percentile of temperature (8.2°C), was evaluated.
Results The cumulative effect of hot exposure on ACS admissions was statistically significant, with a relative risk of 2.04 (95% CI 1.06 to 4.16). The cumulative effect of cold temperature on ACS admissions was found to be non-significant. The highest risk of ACS admission in women was in 38°C (RR, 2.03, 95% CI 1.04 to 4.18). The effect of hot temperature on ACS admission occurred immediately (lag 0) (RR, 1.09, 95% CI 1.001 to 1.19).
Conclusions The high apparent temperature is correlated with a higher ACS admission especially on the same day. These findings may have implications for developing intervention strategies to reduce and prevent temperature-related morbidity especially in the elderly.
- coronary artery disease
- acute coronary syndrome
- atherosclerosis
- public health
- Education
Statistics from Altmetric.com
Introduction
Climate change is an issue of great importance for public health.1 Climate change affects all sections of the community and influences human health by direct and indirect pathways. The four key sectors that will be affected by climate change are water, food, settlement and health. The heat-related mortality is the most direct health impact of global warming.2 Although well-studied investigations about the effect of hot temperature on acute coronary syndrome (ACS) in developed countries have been conducted,3 there is a paucity of research on this problem in low-income and middle-income countries such as Iran.4 An Extreme event weather, such as heatwaves and cold spells, is associated with increased cardiovascular diseases (CVDs), respiratory diseases and renal diseases, leading to mortality and morbidity.5 Ambient temperatures, including minimum, maximum and mean temperatures, are used to assess the impact of temperature on health.6
ACS is one of the most common causes of death in patients with CVD characterised by an acute onset of myocardial ischaemia resulting in myocardial death.7 The spectrum of ACS includes unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI).8 There are few studies about which particular cardiovascular disorders are most influenced by hot and cold spells.9 Increases in hospital admissions of ACS during extreme heat are mostly attributed to hyperthermia, dehydration, heat stroke, ischaemic stroke, diabetes, and fluid and electrolyte imbalances.10 Several possible physiological changes have been proposed to explain the seasonal variation of ACS incidence, including changes in clotting mechanisms, lipid levels, and blood pressure which is associated with physiological changes like increased plasma viscosity.11
The significant relationship between temperatures and ACS incidence suggests that cold temperature may play an important role in the incidence of ACS.12 Previous studies reported that exposure to cold weather would be increased in temperature-related mortality from coronary artery disease.13 Cold temperature causes vasoconstriction, which increases blood pressure and the risk of cardiovascular events. Exposure to cold and hot temperatures puts stress on the cardiovascular system, especially in vulnerable people such as the elderly, and increases the risk of ACS.14
There has been a significant increase in the incidence of coronary artery diseases in Iran in recent years.15 The high incidence of coronary artery disease (CAD) and associated morbidity and mortality in Iran is one of the most concerning public health issues. In Iran, the prevalence of coronary artery disease is higher than Western countries, and there is limited information in regard to coronary risk factors in Iran.15 Due to the lack of studies, the association between metrological variables and incidence of CVD has not been well evaluated in the Iranian population. Our objective was to assess the relationship between apparent temperature and incidence of ACS using time-series analyses.
Methods
This study was conducted in Rasht, the centre of the Guilan province, which is the biggest city located in the north of Iran. This city has a humid subtropical climate with relatively high temperatures in summer and mild winters and occasional winter storm with rainfall coming from convectional thunderstorm activity. The municipality has an area of 180 km2 with more than one million people (Census 2016) at 37.2682° latitude and 49.5891° longitude (figure 1).

The map of Rasht city.
Hospital admission data
Data on the daily counts of admissions for ACS such as unstable angina pectoris (UAP), STEMI and NSTEMI were obtained from the only cardiovascular hospital in Rasht during the period 2005–2014. There is one specialised cardiovascular hospital in Guilan province named Dr Heshmat, Medical and Research Centre. We selected patients with ACS according to the International Classification of Diseases V.10 (I20.0, UAP; I21.0–I21.9, STEMI and NSTEMI).
Meteorological data
The daily data of weather conditions included the minimum (°C), maximum (°C) and mean of temperature (°C), dew point (°C), barometric pressure (mbar), humidity (%), and speed of the wind (m/s) over the 10-year period gathered from the Rasht meteorological centre.
We recruited apparent temperature as exposure variable that combined heat and high humidity, which is a composite index of human discomfort. This index characterises the physiological experience better than ambient temperature because it captures the physiological experience better than temperature alone and also has been used in other studies assessing morbidity and mortality.16 17 With the increase in dew points, the apparent temperature exceeds the actual temperature and the increase in physiological heat stress. The apparent temperature (AT) was calculated with the following formula:
AT=−2.653+(0.994×Ta)+ (0.0153×Td2)16
where Ta is air temperature and Td is dew point temperature.
Data analysis
We used a time-series regression to investigate the relationship between apparent temperature and hospital admission. Previous studies have reported that the association between temperature and mortality is non-linear and might be delayed in time.18 The risk of hospitalisation will be increased on the same day and on several following days.14 19 All data analyses were performed using the R V.3.3.3 software. The ‘dlnm’ package was used to fit the distributed lag non-linear model (DLNM). Spearman’s correlation coefficients were used to explore the monotonic relation between daily admissions of patients with ACS and apparent temperatures. DLNMs were used to estimate the association between ACS hospitalisation and lags of apparent temperature, adjusted for time trends using natural cubic splines, the day of the week and holidays with the R package dlnm. To assess possible delayed associations, we examined the impact of apparent temperature up to 20 days before the admissions.20 21 A quasi-Poisson regression model combined with a DLNM was used to assess the impact of daily apparent temperature on admission at different lag days. This matrix is obtained by the combination of the exposure–response function with a natural cubic spline with three internal knots placed at the 10th, 75th and 90th percentiles of city-specific apparent temperature distributions, and the lag-response function modelled with a natural cubic spline with three internal knots placed at equally spaced values in the log scale.19
The effects of high temperature on ACS admission for each 1°C increase in temperature from the 75th (26.9°C), 90th (30.8°C), 95th (32.5°C) and the 99th (34.7°C) percentiles generally and also based on age and gender were investigated. Also the effects of low temperature on ACS admission for 1°C decrease from the 25th (8.2°C), 10th (4.7°C), 5th (2.6°C) and the 1st (−0.2°C) percentiles generally and based on age and sex were evaluated.22
To examine the high-temperature effect on ACS hospital admission overall and based on age and sex, the relative risk of ACS hospital admission associated with high temperature, the 99th percentile of temperature (34.7°C) compared with the 75th percentile of temperature (26.9°C), was calculated. To examine the cold effect on ACS hospital admission overall and based on age and sex, the relative risk of ACS hospital admission associated with cold temperature, the first percentile of temperature (−0.2°C) compared with the 25th percentile of temperature (8.2°C), was evaluated.23 We used the mean apparent temperature in the present study.
Sensitivity analysis was performed to test the robustness of our main results by changing the location of knots for exposure–response, and 5–20 lag days for apparent temperature, 6–10 df for time trend, 3–10 df for relative humidity and atmospheric pressure were used, respectively.
Results
The results of the DLNM model are provided linking climatological data with the daily incidence of ACS for the total population, men, women and subjects under and over 65 years of age. In the 3653-day period from 20 March 2005 to 20 March 2015, there were 15 094 ACS admissions, among them 2893 cases with UAP and 12 201 with myocardial infarction. The mean daily ACS admission was 5.38±3.9, and the average daily apparent temperature was 17.38°C±9.98°C (table 1). The time-series plot of ACS admission and apparent temperature showed the seasonal variation of exposure and response outcome in 10 years of study, with high admission in summer (figure 2).
Description of daily weather and characteristics of patients with acute coronary syndrome in 2005–2014 in Rasht

Time-series plot of acute coronary syndrome (ACS) admission and apparent temperature.
In figure 2 , the left graphs show the percentage change of ACS admission for each 1°C temperature drop in the 25th (8.2°C) , 10th (4.7°C), 5th (2.6°C) and 1st (−0.2°C) percentiles of temperature overall and based on age and sex, respectively.
Our finding showed that with 1°C decrease in temperature in the 25th, 10th, 5th and 1st percentiles, the percentage of ACS admission decreased in all cases, men, women and people over 65 years, but increased in people under 65 years old.
In figure 3, the right graphs show the percentage change of ACS admission for each 1°C increase in temperature in the 75th (26.9°C), 90th (30.8°C), 95th (32.5°C) and 99th (34.7°C) percentiles of temperature overall and based on age and sex, respectively.
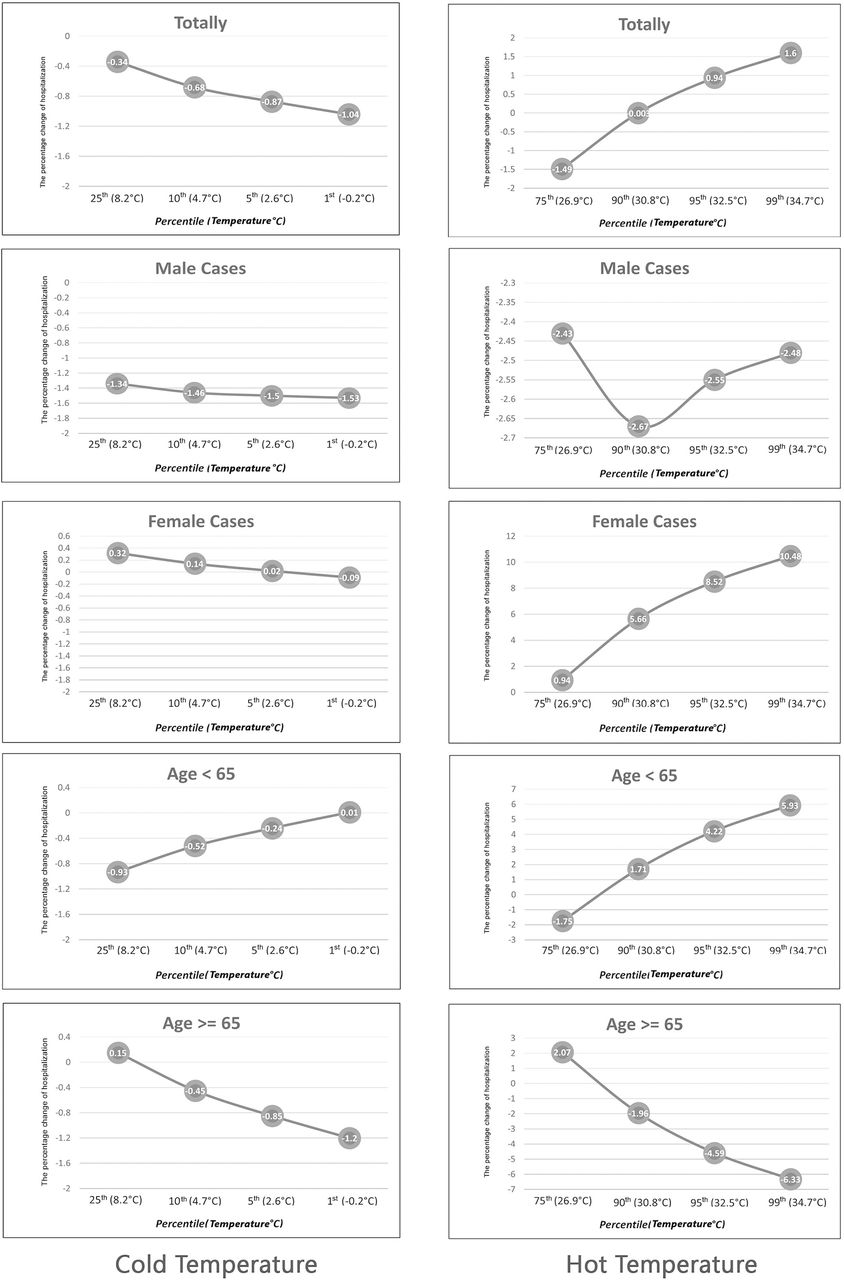
The percentage change of acute coronary syndrome admission related to temperature.
Figure 3 shows that changes in temperature from moderate (75th percentile) to hot (99th percentile) induced ACS admission increase in all cases, women and people under 65 years old.
The heat effect on ACS admission was significant, while the cold effect was not significant. The relative risk of heat exposure on ACS admissions was 2.04 (95% CI 1.06 to 4.16) and for cold exposure was 0.87 (95% CI 0.66 to 1.14), which was not significant (tables 2 and 3). The highest risk of ACS hospitalisation in women was in 38°C (RR, 2.03, 95% CI 1.04 to 4.18), but in men was non-significant in any temperature. The overall effect of heat and cold exposure on ACS admissions based on age was estimated and was not significant.
The cumulative effects of hot temperature on acute coronary syndrome with 99th percentile of temperature (34.7°C) compared with the 75th percentile of temperature (26.9°C)
The cumulative effects of cold temperature on acute coronary syndrome with the first percentile of temperature (−0.2°C) compared with the 25th percentile of temperature (8.2°C)
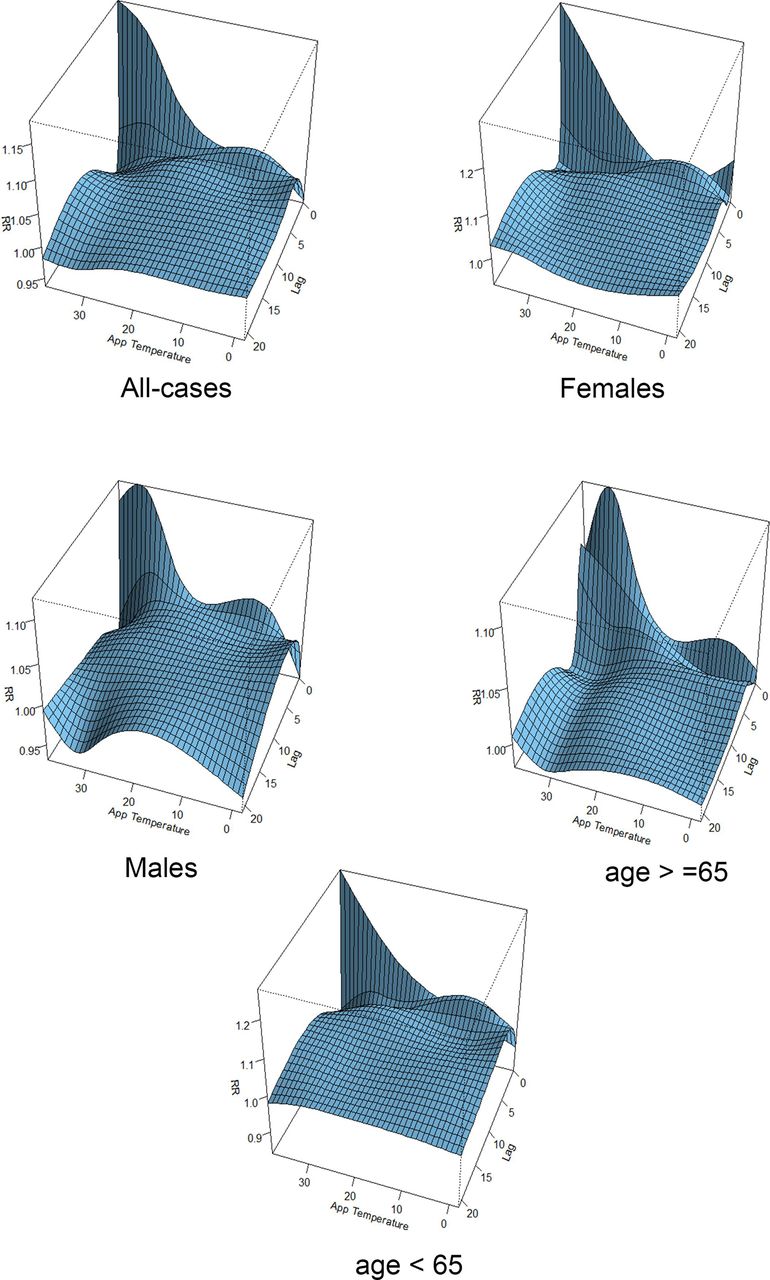
The distributed non-linear lag surface revealed exposure–lag response association with a non-linear relationship between apparent temperature and ACS admission, indicating higher admission risk at hot temperatures (figure 4). The graphs present the relative risk by lag 0–20 days in all cases, men, women, under 65 and over 65 years old.

Relative risks of acute coronary syndrome admission by daily mean apparent temperature (°C) and days of lag.
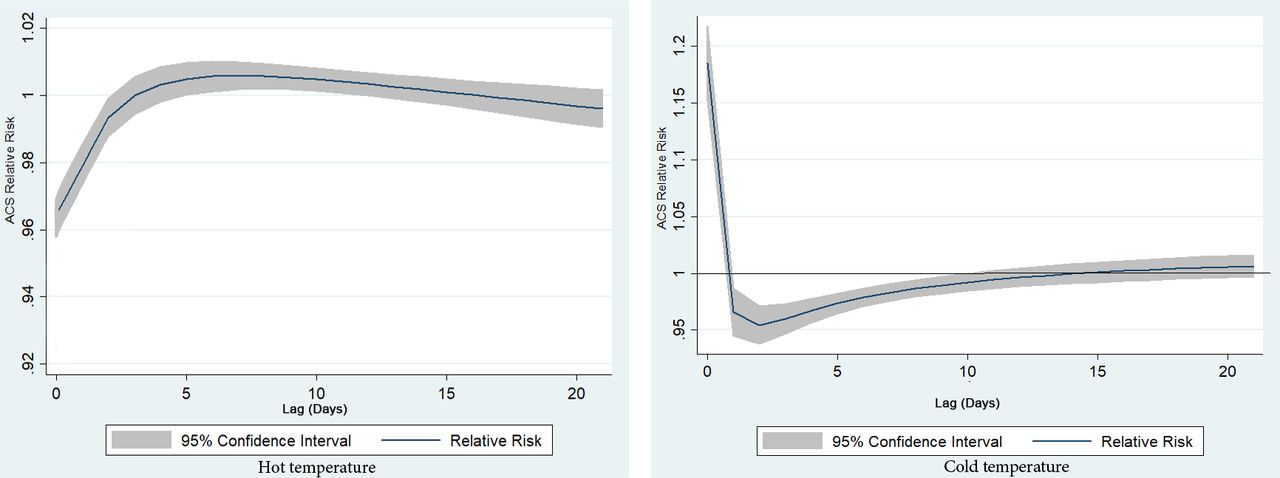
Figure 5 shows the lag structures of apparent temperature effect over the same day up to 20 days before. Our findings showed immediate effects of hot temperatures on ACS admission, with the significant effects on the current day (lag 0).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The effect of mean apparent temperature (°C) on acute coronary syndrome admission along lag days.
The overall effect of hot temperature on ACS admission relative risk on the same day was 1.09 (95% CI 1.001 to 1.19), 1.11 (95% CI 0.96 to 1.28) and 1.08 (95% CI 1.02 to 1.23) in all cases, men and women, respectively (table 2).
Sensitivity analysis was performed in this study for modelling choices. The effect estimates of ACS admission due to temperature were similar when we changed the places of knots for temperature–admission relation and when 5–20 lag days for apparent temperature, 6–10 df for time trend and 3–10 df for relative humidity and air pressure were used, respectively.
Discussion
This study examined the relationships between apparent temperature and ACS hospitalisation in Rasht, the centre of the Guilan province, in the northern part of Iran, between 2005 and 2014. This study indicated that the extremely hot temperatures increased the risk of ACS hospitalisation, but the cold temperature did not show any effect on ACS admission. This result is consistent with other investigations indicating hot weather is responsible for the most part of the temperature-related ACS admission.24 In contrast, a study reported the occurrence of acute myocardial infarction was associated with low temperatures,25 and the study conducted by Wolf et al 3 showed that the risk for the occurrence of myocardial infarction was similar in winters and summers, which was non-significant. On the other hand, many previous studies showed both hot and cold temperatures increased the risk of ACS admission especially for myocardial infarction.14 One of the reasons for the contradiction in the results of our study and with other studies is the use of the apparent temperature index, which is a composite index of human discomfort due to combined heat and high humidity in this study. At higher humidity, the apparent temperature exceeds the ambient temperature and increases physiological heat stress.16 Moreover, exposure to high temperature could increase plasma viscosity, cholesterol levels in serum, changes in vascular tone, autonomic nervous system response, and ultimately increases the tendency to clot in the vessels.11 26
In this study, the highest relative risk of ACS admission in all cases and women were 28°C and 38°C, respectively. In this regard, Lee et al 27 reported a rapid increase of acute myocardial infarction (AMI) over 32°C and 29.6°C, respectively. Our study showed seasonal variations in ACS admission so that the highest rate of admission was in summer. Consistent with this finding, Nastos et al 24 in Crete Island, Greece, reported the same pattern. In contrast, many other studies reported that the occurrence of myocardial infarction is associated with the winter season.28
The difference between the results of this study and a number of previous studies26 could be due to the weather conditions of Rasht, with mild winters and hot and humid summers. The high humidity is known to increase risks because physiological responses for heat dispersion such as sweating are limited.29
This study has also explored the lag effects of temperature on ACS up to 20 days. The strongest relationship between high apparent temperature and ACS was on the same day, which is consistent with other studies.14 The effect of hot temperature on the elderly was immediate (lag 0–1) but was delayed (lag 0–14) in men. According to previous studies, the temperature variability had delayed effect on health.18 The study conducted by Huang et al 30 showed that the effect of the cold temperatures had a long lag period of 10–25 days, while hot temperatures had a short lag period of only 1–3 days. The ageing phenomena induces some physiological changes in thermoregulation and homeostasis, along with the prevalence of chronic conditions, which cause vulnerability to cold and heat.26
Considering global warming and the high air temperature in recent years in Iran, especially in northern Iran, policy makers, the local community and the public should strengthen awareness of the harmful effect of hot temperature on health, especially for vulnerable people, in the northern areas of Iran.
One of the strengths of this study is the application of apparent temperature instead of ambient temperature. This index combined heat and humidity, which is a composite index of human discomfort. It has long been recognised that the sensation of feeling hot or cold is not dependent on air temperature alone. During winter, humidity makes the temperature feel colder (we feel colder in a more humid climate). In summer, the humidity makes it feel hotter (we feel hotter in a more humid climate). Furthermore, we used DLNM here. The major advantage of this method is that it is flexible enough to simultaneously describe a non-linear exposure–response association and delayed effects or harvesting effect.31
There are some limitations in this study. We did not have data about air pollutants for the study period in Guilan province; therefore, we could not assess this confounder’s effect in this study. Of course, Guilan province due to geographical location, such as proximity to the Caspian Sea and having appropriate wind and monsoon rain, has low pollutants levels.
Also in hospital-recorded data, there was no information on air conditioning use and the location where people spent most of their time. The lack of available data on the amount of fluid intake and the health status of subjects under study was another limitation of the present study.
Conclusion
We investigated the effect of apparent temperature on ACS admissions. A detrimental effect of high apparent temperature on ACS admissions was observed. We found stronger high-temperature effect on ACS on the same day. These findings may help to better understand the relationship between temperature and morbidity in order to assist in developing effective public health intervention measures to prevent and reduce temperature-related mortality. Adaptation strategies such as using air conditioners in summer, adequate hydration, as well as a well-established early warning system and emergency service seem to reduce the amount of ACS morbidity and mortality.
Key messages
What is already known about this subject?
Despite studies that examined the relationship between temperature and cardiovascular disease in some countries, especially developed countries, little has been done in low-income and middle-income countries such as Iran.
Also, most studies have examined cardiovascular disease in general, while in our study the relationship between temperature variability and acute coronary syndrome was specifically investigated.
What does this study add?
The majority of ACS admission was caused by hot temperature. The strongest relationship between high apparent temperature and ACS was on the same day. The time-series plot of ACS admission and apparent temperature, showed the seasonal variationof exposure and response outcome in 10 years of study.
How might this impact on clinical practice?
Adaptation strategies such as adequate hydration, as well as a well-established early warning system and emergency service seem to reduce the amount of ACS morbidity and mortality.
Acknowledgments
This study was part of a PhD thesis supported by Tehran University of Medical Sciences (TUMS).
References
Footnotes
Present affiliation The present affiliation of Mohammad Taghi Moghadamnia is: Department of Medical - Surgical Nursing, Guilan University of Medical Sciences, Guilan, Rasht, Iran
Present affiliation The present affiliation of Ali Ardalan is: Harvard Humanitarian Initiative, Harvard University, Massachusetts, cambridge, United States
Contributors All authors of the manuscript certify that they had the same contribution in writing the manuscript. MTM: developing and planning the research idea and preparing the final manuscript. AA: supervision and responsibility for the organisation. AM: responsibility for conducting a literature search. KN: conduct and reporting of the work. MSY: analysis of data and preparing the primary draft on outputs.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.