Article Text

Abstract
Background The importance of registries for collaborative quality improvement has been overlooked in low/middle-income countries (LMIC). Aga Khan University Hospital (AKUH) in Pakistan joined the Congenital Cardiac Catheterization Project on Outcomes-Quality Improvement (C3PO-QI) in March 2017 with the goal of leveraging international collaboration to improve patient care and institutional standards.
Methods The C3PO-QI key driver-based approach was used, with certain modifications, for process re-engineering in AKUH’s congenital cardiac catheterisation laboratory (CCL) to reduce radiation exposure during cardiac catheterisation procedures (the primary outcome of C3PO- QI). Educating staff and standardising procedural documentation were the principal goals of the process re-engineering. Data survey was used to assess staff knowledge, attitude and practice before and after the initiative. Additionally, case demographics and outcomes were compared between AKUH and C3PO-QI centres.
Results There was an increase in appropriate recording of radiation surrogates (0%–100%, p=0.00) and in the percentage of cases that met the established benchmark of ‘Ideal documentation’ (35% vs 95%, p=0.001). There was also an increase in self-reported staff interest during the case (25% vs 75%, p=0.001). AKUH versus C3PO-QI data showed similar demographic characteristics. There was a slight over-representation of diagnostic cases (42% vs 32%) as compared with interventional (58% vs 68%) at AKUH. Furthermore, interventional procedures were predominately PDA and ASD device closures (n=19 and 15, respectively). The frequency of adverse events were the same between AKUH and collaborative sites.
Conclusion Collaborative efforts between developed and LMIC CCL are significant in advancing system-level processes.
- congenital heart disease
- paediatric interventional cardiology
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Collaborative quality assessment is a common practice in developed countries through the use of multicentre registries.
What does this study add?
This will be the first report from a low/middle-income country (LMIC) on the impact of international collaboration and the resulting improvement of institutional practices in a low-resource setting.
How might this impact on clinical practice?
By adopting the key driver diagram, any centre in an LMIC can evaluate and improve their radiation and procedural safety practices.
Introduction
In cardiac catheterisation for congenital heart disease (CHD), a concerted effort is being made to transition from registries to quality improvement (QI) collaboratives. Such collaboratives have been shown to improve quality of care and help assess performance that is risk stratified for better comparisons.1 2 A classic example of such a transition is the Congenital Cardiac Catheterization Project on Outcomes (C3PO), a US-based multicentre registry launched in 2006 which assesses and compares outcomes while exploring measures of procedural efficacy.3 In 2013, the C3PO collaborative moved beyond benchmarking and towards practice improvement through various QI initiatives (C3PO-QI),4–7 specifically reducing radiation exposure in paediatric cardiac catheterisation cases.8 Significant decreases in radiation exposure have resulted from this collaborative.
Experience from the International Quality Improvement Collaborative (IQIC) has also shown significant improvement in outcomes related to CHD surgeries in low/middle-income countries (LMIC), illustrating the success of collaboratives between developed countries and LMICs.9 A significant number of patients with CHD in LMICs who undergo CHD surgery also undergo cardiac catheterisation. The challenges in LMICs are unique and complex, including a lack of resources, late presentation of disease, inadequate skills and training,10 11 non-standardised documentation and a lack of system support.12–15 No registries or formal collaboratives exist to highlight these unique issues and their effects on procedural outcomes. Similarly, no collaboratives, such as those that exist for congenital cardiac surgery like the IQIC, have been established for the congenital cardiac catheterisation laboratory (CCL). The Aga Khan University Hospital (AKUH) joined the C3PO-QI as the first site from an LMIC, thus establishing the first such collaboration, in March 2017. The objective of this paper is (1) to demonstrate how association with a QI-based registry helps improve processes in CCL present in an LMIC and (2) to compare catheterization laboratory data at AKUH with the cumulative C3PO-QI participants.
Methods
This is a comparative, cross-sectional descriptive study. This QI initiative project was conducted in the CCL of AKUH in Karachi, Pakistan, between September 2016 and November 2017, and was divided into three phases. The preintervention phase (September 2016 to February 2017) was compared with a postintervention phase (June 2017 November 2017). Interventions took place between March 2017 to May 2017 (implementation phase).
Identification of key drivers
AKUH is a 644-bed tertiary care teaching hospital in Karachi, Pakistan, catering to all aspects of paediatric and adult diseases. The CCL has two single plane cameras and all resources (equipment and staff) are shared between paediatric and adult cases. Inappropriate radiation exposure was observed in congenital cardiac CT which led to an effort towards decreasing radiation exposure for CHD cases in any modality associated with radiation exposure. The principal investigator of C3PO-QI was contacted and AKUH joined the collaborative as its only international site in March 2017.
An internal audit of our system was performed to assess our readiness to join C3PO-QI. The following gaps were identified related to processes in our CCL pertaining to congenital cardiac catheterisations procedure:
Knowledge of radiation, its surrogates and efforts to reduce radiation exposure in the CCL were lacking. Only fluoroscopy time (FT) was used to track radiation. Standardised tracking of staff radiation exposure (proper dosimetry batch monitoring) and equipment radiation safety (lead apron cracks, availability of thyroid guards) were inadequate.
Inadequate procedure-related documentation, especially of adverse events and procedure efficacy assessment.
No standardised precase discussion that led to staff disinterest and a lack of case-related knowledge.
No quality metrics were tracked and the mortality/morbidity meetings were irregular.
Based on these factors, we identified the following four key drivers vital to improving safety practices:
Promotion of safe radiation practices.
Adequate staff education.
Documentation optimisation.
Sustainability of standard practices.
Interventions specifically targeting the above-mentioned key drivers were designed and executed (figure 1).
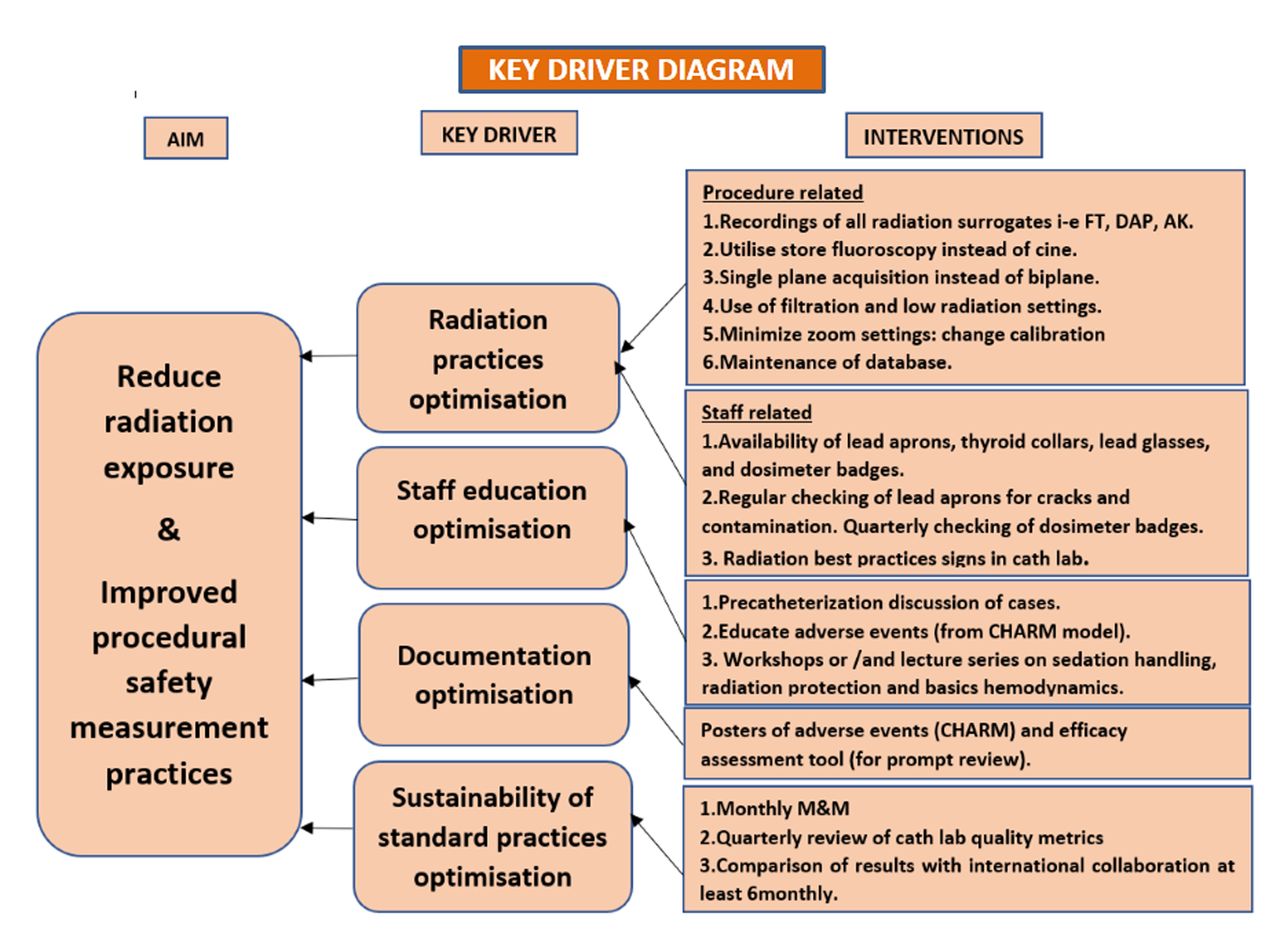
Key driver diagram with aim, key drivers and detailed interventions.
Interventions
An introductory lecture session was arranged for the CCL staff to introduce C3PO-QI, its objectives, data variables and the importance of joining the collaborative. This was done to familiarise the staff and get their buy-in by encouraging feedback and questions regarding the collaborative. The following specific interventions were then implemented (table 1).
Key drivers with their specific interventions
Definitions (adequate vs inadequate) of outcome metrics
Data collection
General variables that were collected included: age in years, gender, weight, height, diagnosis (physiological and STS), procedure type (diagnostic vs interventional), radiation surrogates (fluoroscopic time, air kerma, dose area products (DAP)) and details of adverse events, including categories (sedation or airway related, catheterisation related, access related, angioplasty, device, stent, coil, ablation, biopsy and valvuloplasty-related problems), event preventability (preventable, possibly preventable, not preventable) and event seriousness (levels 1–5).
Assessment of the QI initiative
The following outcome metrics were used to assess the interventions implemented for the described key drivers.
The following outcome metrics were used to assess the interventions implemented for the described key drivers: (1) documentation of radiation protection; (2) staff radiation protection; (3) operator techniques (for radiation practices optimisation); (4) self-interest and knowledge of CCL staff (staff education optimisation); and (5) catheterisation report documentation (documentation optimisation).
Outcomes were defined as adequate and inadequate as described in table 2.
A questionnaire-based Knowledge, attitude, practices (KAP) survey (online supplementary appendix A) was conducted among 20 people, including nursing staff, technologist, cardiologists and trainee fellows. This survey assessed the knowledge and attitude regarding radiation surrogate, protection and information regarding congenital cardiac cases.
Supplemental material
Comparison of AKUH versus collective C3PO-QI cases
Data from June 2017 to November 2017 of all patients with CHD who underwent cardiac catheterisation were entered into the C3PO-QI database. Variables that were used for comparison of AKUH versus C3PO-QI cumulative data included age (<1 year, 1–4 years, 5–9 years, 10–15 years and >15 years), case type (interventional vs diagnostic), radiation exposure (DAP/kg) and occurrence and severity of adverse events.
Various metrics (FT, air kerma, DAP, and so on) exist to determine the amount of radiation exposure during cardiac catheterisation.7 In pediatrics, the stochastic risk of radiation is the main concern rather than deterministic effects.4 DAP is the product of the air kerma dose and the cross-sectional area exposed to the X-ray beam (μGy-M2).5 DAP provides a better measure of the stochastic risk associated with cardiac catheterisation and has become a widely adopted method of radiation exposure reporting.4 8 When accounting for radiation, it is imperative to adjust for varying patient size and procedure type. Such risk adjustment provides an opportunity for fair comparison among centres and purposeful QI initiatives. The C3PO-QI recently showed that DAP indexed to weight (DAP/kg) provides an acceptable adjustment of outcomes, accounting for the variability in dose seen among cases of varying patient sizes.9 Similarly, risk stratification of radiation exposure based on procedural complexity and patient size has been proposed (manuscript in review) in which 90% of procedures performed in nine centres of the C3PO-QI collaborative were categorised into three radiation exposure categories: low (<100 µGy-M2/kg), medium (100–200 µGy-3 M2/kg) and high (>200 µGy-M2/kg). The radiation risk category type (rad type) was chosen for comparison in this manuscript as it incorporates both the procedural and patient size stratification.
Adverse events were broadly classified as problems related to the catheterisation, access, sedation or airway, angioplasty, device, stent, coil, ablation, biopsy or valvuloplasty. The following definitions were used for adverse event severity (online supplementary file 1).5
Supplemental material
he following definitions were used for preventability:
Not preventable: Any event in which the timing of the intervention cannot change the effect.
Possibly preventable: Any event in which timely intervention can change the effect.
Preventable: Any event missed and avoidable by appropriate care.
These data were captured from revised catheterisation reports and the paediatric radiation surrogate register. Data were entered by the senior fellow and internally audited twice by two cardiologists.
Statistical analysis
Simple frequencies were used for categorical data while χ2 test was used for comparison. For continuous variables, median with IQR was used. A p value <0.05 was considered significant.
Results
A total of 106 congenital cardiac catheterisations were performed at AKUH. The median age of catheterisation was 4 (2.0, 12) years. Patent ductus arteriosus (PDA; n=21, 20%) was the most common diagnosis followed by septal lesions (atrial septal defect (ASD) n=19, 18%; ventricular septal defect n=18, 17%) (table 3). The median FT was 10.1 min (7.1, 17.8), median DAP was 163.5 µg/m2 (85.9, 465.3) and median air kerma was 21.5 mGy (11.4, 53.5). There was no mortality during the study period. Out of the 10 (10%) morbidities, 4 (4%) were preventable and an equal number were possibly preventable (table 3).
Demographics of cardiac catheterization cases performed at AKUH
Pre-C3PO-QI versus post-C3PO-QI: KAP survey
Significant improvement in documentation of radiation surrogates (from 0% to 100%, p=0.00) and ideal procedural documentation (35%–95%, p=0.001) were observed. Marked change was observed in staff interest and knowledge (25%–75%, p=0.001) of the case after implementation of precatheterisation discussion. Significant improvement was seen in adequate radiation selection technique (29%–65%, p=0.04) among the technicians while a trend towards improvement in adequate self-radiation protection practices by the staff (41%–59%, p=0.05) was observed.
AKUH versus C3PO-QI catheterisation data comparison
A total of 106 cases were performed at AKUH compared with 2963 cases in the total C3PO-QI collaborative between 1 June and 31 November 2017. There was no difference between AKUH and the C3PO-QI collaborative in age distribution, with the majority of patients falling into the 1–4 years’ age group (39% vs 30%). There was a slight over-representation of diagnostic cases (42% vs 32%) as compared with interventional (58% vs 68%) at AKUH. PDA and ASD device closures (n=19 and 15, respectively) were the predominant interventional procedures at AKUH as compared with PDA closure and pulmonary valve dilation in the C3PO-QI collaborative (n=205 and 131, respectively). Most notably, no TPV procedures were performed at our centre (figure 2).
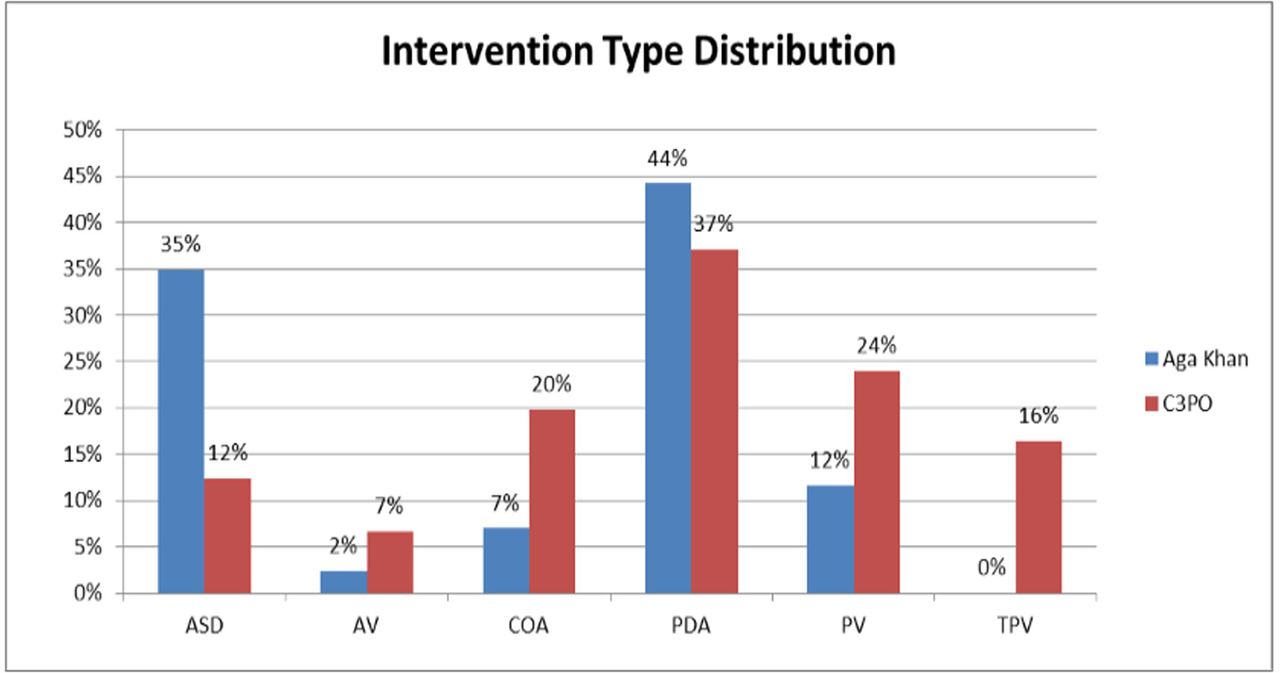
Aga Khan University Hospital (AKUH) versus Congenital Cardiac Catheterization Project on Outcomes-Quality Improvement (C3PO-QI) intervention type distribution comparison. ASD, atrial septal defect; AV, Aortic valvuloplasty; CoA, coarctation of aorta/dilation; PDA, patent ductus arteriosus; PV, Pulmonary valvuloplasty; TPV, Transcatheter pulmonary value replacement.
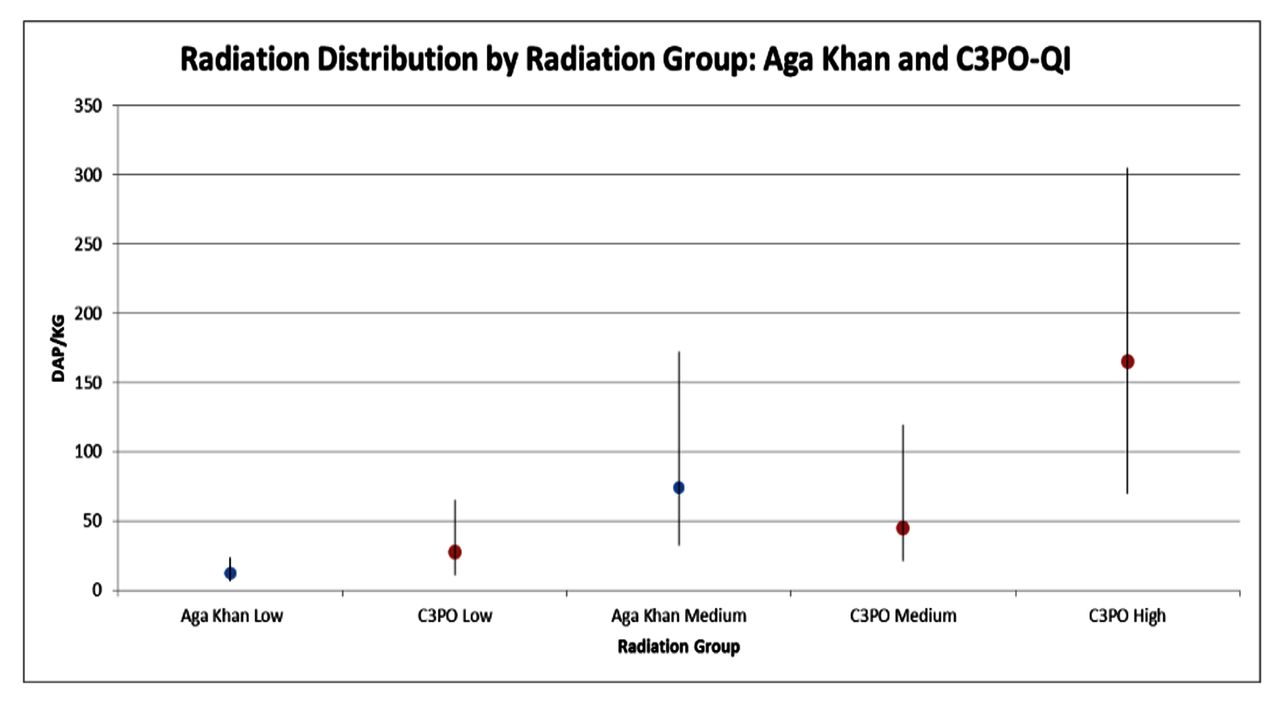
The majority of cases at AKUH fell into the low and medium radiation risk category type with comparable radiation doses (figure 3).
{kind=link}
{kind=link}
{kind=link}
Aga Khan University Hospital (AKUH) versus C3PO-QI radiation distribution by radiation group (low, medium and high). C3PO-QI, Congenital Cardiac Catheterization Project on Outcomes-Quality Improvement; DAP, dose area product.
Though radiation for interventional procedures was lower at AKUH, any conclusive interpretation is limited due to the small number of cases at AKUH (table 4).
AKUH versus C3PO-QI radiation exposure in interventions (DAP/kg)
Overall, AKUH had a lower incidence of adverse events than the collaborative (9% vs 11%) though a higher proportion of high severity adverse events (level 3 and above) was seen at our centre (6% vs 4%) (online supplementary file 2).
Supplemental material
The majority of adverse events were catheterisation-related problems (table 5) including arrhythmias and haemodynamics (table 3).
AKUH versus C3PO-QI adverse event categories
Discussion
We showed that preparing to be a part of an international collaborative helps LMIC CCL programmes in system re-engineering which goes beyond the specific goals of the collaborative. Registries such as C3PO-QI allow for collaboration across institutions, provide large data sets for comparative assessments and improve the ability to generate outcome assessments.1 However, these registries are designed based on the US healthcare system and have, until now, never been implemented anywhere outside of the USA. Hence, the impact of such registries in an LMIC setting, with limited resources and personnel, has never been assessed. To the best of our knowledge, this is the first report on the impact of such a collaborative in an LMIC on improving and maintaining the standards of congenital cardiac catheterisation procedures.
CHD possesses a significant health burden in LMICs like Pakistan, India and Indonesia.3 16 17 This is due to a higher birth rate,18 19 late recognition and presentation of CHD,20–22 comorbidities like malnutrition and infections,17 lack of skills10 and the cost of treatment.10 Outcomes from CHD interventions (surgical or catheter based) in LMICs may differ from outcomes in developed countries due to these factors.23 24 There is a dearth of information regarding CHD interventions and their outcome from LMICs predominantly due to a lack of databases. This precludes LMIC CCL programmes from comparing outcomes, designing contextual risk stratification models and collaborating on QI. Lack of systematic data tracking and procedure standardisation in CCLs may also contribute to system inefficiency and poor outcomes.1 Like other CCLs in LMICs, the experience at AKUH prior to joining the collaborative demonstrated several system-level issues including inadequate documentation, inadequate tracking of procedural outcomes, lack of staff interest in congenital cases and improper radiation safety measures (both for patient and staff).25–28 The success of IQIC in highlighting CHD surgeries in LMICs and significantly improving postoperative morbidity and mortality in patients with CHD is an excellent example of the effectiveness of collaboration between developed and LMIC CHD programmes.9 System-level changes (nurse empowerment, QI teams, systematic data tracking, and so on) and improved practices (surgical checklist, infection control, and so on) were some of the key factors in determining the success of IQIC in our CHD surgical programme.9 We joined C3PO-QI with the intention of not just targeting radiation improvement but to bring about a system-level change in the CCL. This was successfully demonstrated in the improvement and standardisation of documentation, radiation control practices and, most importantly, better staff engagement. Better staff emotional engagement has been demonstrated to be the most important factor in patient experience of care29 and, in turn, is associated with higher quality and safer care.
Though the numbers are limited for any conclusive interpretation, it is interesting to note that the age and case distributions were similar between our centre and the collaborative. Similar adverse outcomes were noticed, with catheterisation-related complications being the highest. Thrombosis of PDA stents contributed to the worse adverse events at AKUH. Our centre did not perform any TPV (due to the cost of the device) and thus did not have any high radiation category procedures. Among the medium and low radiation procedure categories, our results were comparable to the collaborative. Interestingly, ASD, PDA and CoA had much lower radiation exposure in our setting compared with the collaborative. This may be due to use of single plane imaging during the procedure compared with biplane imaging in CCLs of the collaborative.
Limitations
As a single centre study, the generalisability of our results is limited to our locale and similar resource-limited settings. The comparison of preintervention versus postintervention self-proclaimed knowledge acquisition surveys was conducted in the immediate period after intervention. It is well known that this is the greatest period of knowledge retention thus more useful assessment of knowledge retention is planned. Additionally, small number of staff (though all of our CCL staff were interviewed) may impair conclusive interpretation. Though the similarity in case distribution and outcomes and differences in radiation doses were interesting, the small number of cases from our centre may preclude any significant interpretation of these results. It will be interesting to see how these results sustain over time as the number of cases entered increases.
Conclusion
Collaborative efforts between developed and LMIC CCL are helpful in significant improvement among system-level processes. The benefit of such a collaborative, thus, is above and beyond just the specific outcome targeted by the collaborative, that is, improvement in radiation, and in fact participation in the collaborative helps CCLs in LMIC to bring about system-level changes.
References
Footnotes
Contributors FA and BH have contributed equally to the study concept, designing, data collection, analysis and manuscript writing. MQM contributed to the data collection, data analysis and manuscript writing. SA and NA helped in data analysis and manuscript writing. RA, IS, JA, SA and ZN contributed to data collection and data analysis. AG and LB helped in critical designing and revision of the manuscript. All authors have contributed significantly and agree with the content of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.