Article Text

Abstract
Objective ECG markers of heart failure (HF) with preserved ejection fraction (HFpEF) are lacking. We hypothesised that the Cornell product (CP) is a risk marker of HFpEF and has prognostic utility in HFpEF.
Methods CP =[(amplitude of R wave in aVL+depth of S wave in V3)×QRS] was measured on baseline 12-lead ECG in a prospective Asian population-based study of 606 healthy controls (aged 55±10 years, 45% men), 221 hypertensive controls (62±9 years, 58% men) and 242 HFpEF (68±12 years, 49% men); all with EF ≥50% and followed for 2 years for all-cause mortality and HF hospitalisations.
Results CP increased across groups from healthy controls to hypertensive controls to HFpEF, and distinguished between HFpEF and hypertension with an optimal cut-off of ≥1800 mm*ms (sensitivity 40%, specificity 85%). Age, male sex, systolic blood pressure (SBP) and heart rate were independent predictors of CP ≥1800 mm*ms, and CP was associated with echocardiographic E/e′ (r=0.27, p<0.01) and left ventricular mass index (r=0.46, p<0.01). Adjusting for clinical and echocardiographic variables and log N-terminal pro B-type natriuretic peptide (NT-proBNP), CP ≥1800 mm*ms was significantly associated with HFpEF (adjusted OR 2.7, 95% CI 1.0 to 7.0). At 2-year follow-up, there were 29 deaths and 61 HF hospitalisations, all within the HFpEF group. Even after adjusting for log NT-proBNP, clinical and echocardiographic variables, CP ≥1800 mm*ms remained strongly associated with a higher composite endpoint of all-cause mortality and HF hospitalisations (adjusted HR 2.1, 95% CI 1.2 to 3.5).
Conclusion The Cornell product is an easily applicable ECG marker of HFpEF and predicts poor prognosis by reflecting the severity of diastolic dysfunction and LV hypertrophy.
- electrocardiography
- heart failure with normal ejection fraction
- hypertensive heart disease
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Heart failure (HF) with preserved ejection fraction (HFpEF) is associated with significant morbidity and mortality and remains a major burden to healthcare systems globally.
Diagnosis of HFpEF requires comprehensive transthoracic echocardiograms and may be aided by adjunctive serum biomarkers such as N-terminal pro B-type natriuretic peptide. ECG markers of HFpEF are lacking.
What does this study add?
The ECG marker, Cornell product, at a cut-off of greater than or equal to 1800 mm*ms distinguishes HFpEF from hypertension, with threefold increased odds of HFpEF. In patients with HFpEF, a Cornell product of ≥1800 mm*ms is also associated with two times higher likelihood of all-cause mortality and HF hospitalisations.
How might this impact on clinical practice?
The ECG Cornell product is an easily derived and applicable marker of HFpEF and is associated with poorer outcomes above a cut-off of ≥1800 mm*ms.
Introduction
Heart failure with preserved ejection fraction (HFpEF) has been studied with great interest in recent times. In addition to increased systemic afterload, ventricular stiffness and impaired diastolic function have also been suggested in the pathophysiology of HFpEF.1–3 The assessment of HFpEF involves objective evidence of diastolic dysfunction in the presence of normal systolic function on transthoracic echocardiography. Left ventricular hypertrophy (LVH), determined by left ventricular mass, has been widely used as a surrogate of diastolic function in the diagnosis of HFpEF.4–6
A quick and simple way to screen for LVH without the use of echocardiography would be through the widely available 12-lead ECG. Several ECG voltage criteria have been developed in the assessment of LVH, including the Sokolow-Lyon and Cornell voltage criteria.7 8 The Cornell product (CP),9 an ECG voltage-duration product, was found to have greater sensitivity for LVH9 10 and has been shown to be associated with diastolic dysfunction.11
We hypothesised that CP would be an alternate way of identifying patients at high risk of HFpEF and sought to determine the implications of CP in patients with HFpEF.
Methods
Study population
The study population included participants from the Singapore Heart Failure Outcomes and Phenotypes (SHOP) Study,12 a prospective study of consecutive in-patients and outpatients identified with heart failure (HF) from six centres in Singapore followed up over 2 years, as well as healthy controls without HF from the community-based Singapore Longitudinal Ageing Study (SLAS).13 Participants in SLAS were adults randomly sampled from the community via door-to-door census of residents in contiguous precincts within five districts in Southeastern Singapore. All participants underwent detailed clinical profiling with prospective 12-lead resting ECG, comprehensive Doppler echocardiography, phlebotomy for biomarker measurements and were followed up for all-cause death and HF hospitalisations. In compliance with the Declaration of Helsinki, informed consent was obtained from all participants. As this was a prospective study, there was no recall bias and only participants with HF were recruited in the HFpEF group, hence avoiding selection bias. There were minimal missing data, and hence imputation was not performed. Loss to follow-up was minimal at <1%.
In this study with 2087 subjects (1100 with HF), participants with reduced EF <50% or left bundle branch block were excluded. The remaining 1069 participants were split into three groups (827 participants from SLAS in both groups I and II and 242 participants from SHOP in group III).
Group I: healthy controls (no hypertension and no HF).
Group II: participants with hypertension only without HF.
Group III: participants with HFpEF.
Importantly, the diagnosis of HFpEF was based on the validated clinical diagnosis of HF (the presence of typical symptoms and signs, established by cardiologists and validated by investigators) and the presence of LVEF ≥50% (independently verified in an echocardiography core laboratory). As previously published,14 49 out of 50 HFpEF cases in a substudy satisfied the detailed 2007 European diagnostic criteria for HFpEF.4
Electrocardiography
Resting baseline standard 12-lead ECGs were done at recruitment. ECGs were performed in a standardised fashion across all participating centres. To minimise intercentre and interobserver variability, the same ECG machine (Mortara ELI 250, Milwaukee, Wisconsin, USA) was used across all centres and ECGs calibrated at 25 mm/s and 1 mV/cm were read by a single, independent, trained reader. ECG variables of interest including R wave amplitude in aVL (RaVL), S wave depth in V3 (SV3) and QRS duration were recorded. ECG CP was defined as: CP=((RaVL+SV3)*QRS duration).9
Echocardiography
Comprehensive two-dimensional echocardiograms, including M-mode, pulse wave Doppler and tissue Doppler imaging, were performed by experienced sonographers. Commercially available ultrasound systems (Vivid seven and E9, General Electric, Milwaukee, Wisconsin, USA) equipped with broadband transducers were used across all centres. Measurements of ejection fraction, mitral inflow E and A velocities, septal and LV lateral annular early diastolic velocities (e′), LV dimensions including interventricular septum thickness, LV internal diameter and inferolateral wall thickness were made by trained echocardiographers blinded to ECG data. As all patients included in this study had preserved LVEF, average E/e′>14 was used as the definitive marker of diastolic dysfunction in our study as per American Society of Echocardiography recommendations.15 LV mass was calculated using the Cube formula16 and LV mass index (LVMI) obtained by indexing LV mass to body surface area.
Statistical analysis
Baseline characteristics were reported as percentages (%) for categorical variables and mean±SD or median with IQR for continuous variables. Bivariate analyses were carried out with the χ2 (categorical) or Kruskal-Wallis test (continuous). Pairwise correlations were made between CP and echocardiographic markers of LVMI and E/e′ ratio. An optimal CP cut-off to distinguish between HFpEF and hypertension without HF was identified using receiver operating characteristics (ROC) curves. Kaplan-Meier curves were generated to compare time to all-cause mortality, time to first recurrent HF hospitalisation and time to composite event (all-cause mortality and first recurrent HF hospitalisation) according to the optimal CP cut-off.
To ascertain the association of CP with clinical covariates and its prognostic significance at the identified cut-off, a generalised structural equation model (gSEM) was constructed.17 The association between CP and clinical and echocardiographic variables (age, gender, ethnicity, blood pressure, heart rate, E/e′ and LVMI) were determined, and time to events (all-cause mortality, first recurrent HF hospitalisation and composite event) was estimated in patients with HFpEF only. Two-sided statistical tests were performed at 5% level of significance. All data analyses were carried out with Stata MP V.14.
Results
Baseline characteristics
Baseline characteristics of the study population by group are shown in table 1. A total of 1069 adults (median CP 1065 mm*ms (IQR 736–1517)) were included in this study, with 606 healthy controls (55±10 years, 45% men), 221 controls with hypertension but without HF (62±9 years, 58% men) and 242 with HFpEF (68±12 years, 49% men). In the HFpEF group, 86% of participants had hypertension. Median CP increased across groups from 924 mm*ms in healthy controls to 1210 mm*ms in hypertension without HF to 1523 mm*ms in HFpEF (p<0.001) (figure 1). Similarly, there was an increasing trend in age, body mass index, QRS duration (ms), R wave amplitude in aVL, depth of S wave in V3, E/e′, LVMI and N-terminal pro B-type natriuretic peptide (NT-proBNP) across all three groups (table 1).
Baseline characteristics of study population (n=1069)

Distribution of Cornell product across study population.
The optimal CP cut-off for predicting HFpEF from hypertension without HF (Group II and III only) was identified to be greater than or equal to 1800mm*ms, with sensitivity and specificity of 40% and 85%, respectively (area under ROC curve 0.62; 95% CI 0.56 to 0.67). Sex-specific cut-offs were also tested but they did not significantly improve diagnostic accuracy. Age, gender, SBP and heart rate were significant independent predictors of a CP ≥1800 mm*ms (table 2). The associations between the optimal CP cut-off and ethnicity were not significant when compared with the reference Chinese group (table 2).
Association of clinical covariates with CP ≥1800 mm*ms
Association of CP with HFpEF
CP ≥1800 mm*ms was significantly associated with sixfold increased odds of HFpEF after adjusting for clinical variables of age, sex, ethnicity, SBP and heart rate (table 3) among patients from Groups II and III. When adjusted for clinical variables and echocardiographic variables of LVMI and mitral E/e′, CP ≥1800 mm*ms was associated with twofold increased odds of HFpEF (table 3). CP correlated positively with NT-proBNP, which was also a significant predictor of HFpEF (adjusted OR (AOR) of logNT-proBNP 6.03, 95% CI 3.76 to 9.69) (r=0.27, p<0.001). However, after adjusting for both clinical and echocardiographic variables, as well as logNT-proBNP, CP remained strongly predictive of HFpEF with threefold increased odds (table 3). Even when analysed as a continuous variable, CP remained strongly predictive with 10% increased odds of HFpEF for every 100 mm*ms increase in CP after adjusting for clinical variables.
Association of CP≥1800 mm*ms with HFpEF
CP was also significantly associated with the echocardiographic markers of diastolic dysfunction, E/e′ (r=0.27, p<0.001) and LVMI (r=0.46, p<0.01). Stratifying by gender, CP maintained its correlation with LVMI (r=0.42, p<0.001 in males and r=0.43, p<0.001 in females).
Association of CP with outcomes
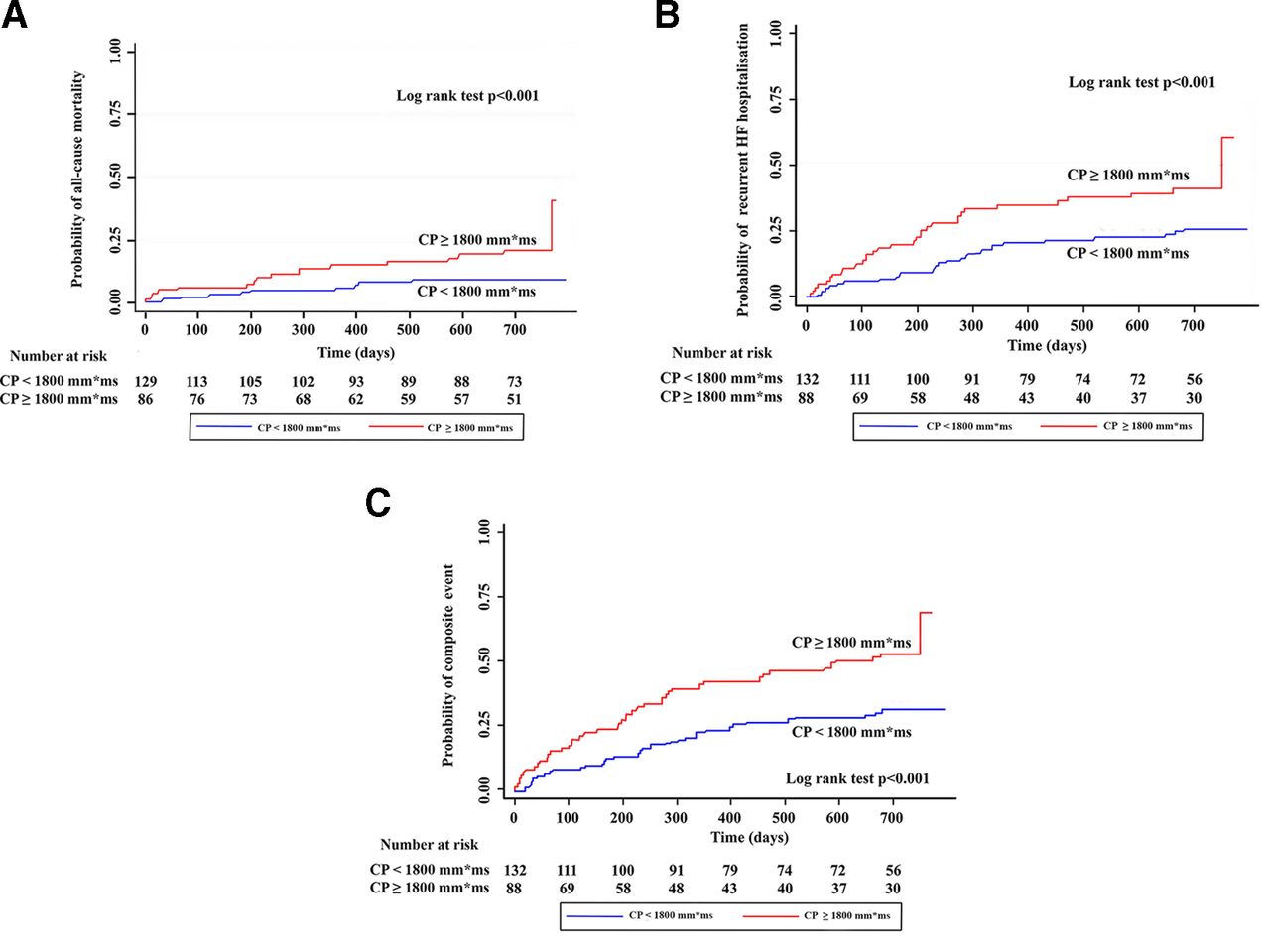
During follow-up of 2 years, there were 29 deaths and 61 first HF admissions from enrolment, all of which occurred in the HFpEF group. The relationships of CP ≥1800 mm*ms to time to events are depicted in table 4. In patients with HFpEF (Group III only), those with CP ≥1800 mm*ms were associated with a twofold increased risk of earlier composite outcomes of all-cause death and recurrent HF hospitalisation after adjustment for age, sex, ethnicity, SBP, heart rate, E/e′, LVMI as well as logNT-proBNP (table 4, figure 2). There was no significant interaction between logNT-proBNP and CP 1800 (pinteraction=0.81) on their association with outcomes. The increased association was noted when all-cause death and HF hospitalisation were accessed individually (table 4).
Association of CP ≥1800 mm*ms with time to events in patients with heart failure with preserved ejection fraction
{kind=link}
{kind=link}
(A) CP ≥1800 mm*ms and all-cause mortality in HFpEF. (B) CP ≥1800 mm*ms and recurrent HF hospitalisation in HFpEF. (C) CP ≥1800 mm*ms and composite of all-cause mortality and recurrent HF hospitalisation. (A–C) Kaplan-Meier curves of the association of CP at the optimal cut-off of 1800 mm*ms with composite of all-cause mortality and first recurrent HF hospitalisation in patients with HFpEF. CP, Cornell product; HF, heart failure; HFpEF, HF with preserved ejection fraction.
Discussion
We demonstrate that the CP is an important risk ECG marker of HFpEF, and at a cut-off greater or equal to 1800 mm*ms, CP is a strong marker of HFpEF and poorer prognosis. Moreover, its prognostic value is independent of NT-proBNP and age.
Association of CP and clinical covariates
The CP was developed as an extension of the ECG Cornell voltage criteria for better sensitivity in detecting LVH.9 10 Casale et al found significant sex differences in SV3, while age did not influence ECG detection of LVH.7 Similarly, we found that females were less likely to have a CP ≥1800 mm*ms than men, which may be accounted for by their lower LV mass. Apart from gender, we observed that age, heart rate and SBP were independently associated with CP. The association of ECG parameters with age, sex and ethnicity has been previously described, with men having wider QRS and deeper SV3, while age was associated with wider QRS and taller RaVL and Malays with wider QRS duration.18 We observed no inter-ethnic differences in CP, likely due to the small number of Malays and Indians as compared with Chinese. The effect of heart rate on CP is more uncertain, although recent studies have shown reductions in QRS duration with increased heart rates.19 20 The effect of heart rate on RaVL and SV3 remains unknown.
Association of CP and HFpEF
Even though Molloy et al 10 had previously found sex-specific values for ECG Cornell voltage criteria, we did not find significant differences in the association between CP and HFpEF when sex-specific cut-offs were used. Sex-specific cut-offs in the association between CP and HFpEF were therefore not applied, and a cut-off of CP ≥1800 mm*ms was used in both sexes.
The CP has higher sensitivity in patients with more severe LVH.10 Okin et al showed that above a median LVMI of 153 g/m2, CP had a sensitivity of 41% compared with 33% in LVMI <153 g/m2.9 Our study reiterates these findings, showing an increase in CP across the three groups from healthy controls to hypertension to HFpEF, corresponding with higher LVMI in the same rank order. The moderate to strong correlation with LVMI indicates a direct influence of LVH on the constituent ECG components of CP, arising from prolonged impulse conduction in hypertrophied myocardium and velocity changes secondary to intramural fibrosis.10 21 Previous studies have found a diagnostic threshold for LVH at CP of 2440 mm*ms9 10 and 2370 mm*ms more recently in a Japanese study.22 Median CP levels in patients with HFpEF from our study were however lower, suggesting a risk of HF at even lower CP levels.
Krepp et al demonstrated that CP was a strong predictor of diastolic dysfunction, with fivefold increased odds when CP was ≥1595 mm*ms.11 Although our study was not intended to determine the relationship between CP and diastolic dysfunction, the correlation between CP and E/e′ (r=0.27, p<0.001) and trend towards HF with higher CP values supports such an association. Our patients with HFpEF had a mean E/e′ ratio of 14.5 and a corresponding median CP of 1523 mm*ms, suggesting that even at lower CP values 1595 mm*ms, patients may already have diastolic dysfunction and be at risk of progression to HF. In contrast, hypertensive participants without HF had a mean E/e′ of 9.6 and a corresponding median CP of 1210 mm*ms.
Results from the Dallas Heart Study showed that compared with ECG alone, NT-proBNP had higher sensitivity and lower specificity for LVH, but the combination of NT-proBNP and ECG LVH criteria significantly improved the discrimination of LVH.23 The positive correlation of NT-proBNP with CP and their independent associations with HFpEF further demonstrate that both are complementary markers in screening for LVH,23 Even after accounting for NT-proBNP, CP at the cut-off value of greater than or equal to 1800 mm*ms was still predictive of HFpEF from hypertensive heart disease without HF.
The association of CP with HFpEF is likely a reflection of the severity of LVH as well as diastolic dysfunction. Although HFpEF remains a clinical diagnosis requiring history, physical examination and echocardiographic findings, ECGs are widely available, affordable and commonly used to screen symptomatic patients. In this context, the recognition of CP as a marker of increased risk of HFpEF may be useful.
Prognostic utility of CP
Data on the prognostic utility of CP in HFpEF are scarce. The associations of CP with death and HF rehospitalisations in chronic HF was demonstrated by Otaki et al,22 and the incremental value of CP in predicting HF when combined with echocardiographic LVH criteria by Gerdts et al.24 However, both studies included patients with reduced LVEF. Other studies have also shown that CP is a useful predictor of adverse cardiac events and stroke25 26 but did not take LVEF into account. However, in our study of only patients with LVEF ≥50%, we showed that in addition to predicting increased HFpEF hospitalisations, CP ≥1800 also predicts for earlier HF hospitalisations.
The association of CP with mortality had previously been established by Sundström et al. At the LVH diagnostic threshold of 2440 mm*ms, CP conferred HRs of 3.56 and 3.82 for cardiovascular and total mortality, respectively, after adjusting for cardiovascular risk factors.27 The Losartan Intervention for Endpoint reduction in hypertension study demonstrated a reduction in HF hospitalisations28 and lower risks of cardiovascular mortality, myocardial infarctions and stroke with CP regression during antihypertensive therapy.29 Our study extends these findings to patients with HFpEF, some of whom were not hypertensive. We report the ability of CP ≥1800 mm*ms to predict worse outcomes in these patients, which was independent of multiple factors known to impact outcomes. Thus, patients may already be at higher risk of HF and mortality, even before florid expression of ECG LVH.27
BNPs have been shown to predict worse outcomes in HFpEF and HFrEF—for a given BNP level, the risk of all-cause mortality and HF hospitalisation is similar in both HFpEF and HFrEF.30 In our study, NT-proBNP was similarly a significant predictor of HF readmissions and all-cause mortality. However, despite the presence of NT-proBNP as a strong predictor of poorer outcomes, CP ≥1800 mm*ms remained independently associated with increased composite events. Our study suggests that in addition to BNP or NT-proBNP, CP may be an inexpensive and readily available prognostic marker among patients with HFpEF.
Limitations
The small number of mortality events limited the survival analyses and reflected brief follow-up. We analysed CP at a single time point but acknowledge that time trends of CP and their relationship to outcomes would be of interest. Participants in our study were all Asians, in particular, a predominantly ethnic Chinese population. Given ethnic variations in the prevalence of hypertension and ECG parameters, this may potentially limit the generalisability of our findings, in particular the cut-off point of greater than or equal to 1800 mm*ms across all populations. Differences between body and heart size, as well as ECG differences between Caucasian and Asian populations are well recognised, and comparative future studies are warranted.
Conclusion
The ECG CP is an important risk marker of HFpEF and is independently related to poorer outcomes in HFpEF. It is a useful and easily measured alternative to identify patients at high risk of HFpEF.
Acknowledgments
The authors thank the sonographers, technicians, nurses and staff at the Cardiovascular Research Institute, National University Heart Centre, Singapore, for their technical and clinical support.
References
Footnotes
CSL and TWL contributed equally.
Contributors ET and SPC contributed to data analysis and writing of the manuscript. CFX, JY, AMR, LHL, DS, FJ, DY, SYL, HYO, KTGL, TPN, SZN and LF contributed to the conduction of the study. CFX, SZN and LF contributed to the data acquisition. ET, JY, AMR, LHL, DS, FJ, DY, SYL, HYO, KTGL and TPN contributed to the reporting. ET, AMR, PO, CL and TWL contributed to the planning. ET, SPC, AMR, PO, CL and TWl contributed to the interpretation of data. CFX, JY, AMR, LHL, DS, FJ, DY, SYL, HYO, KTGL, TPN, SZN, LF, PO, CL and TWL contributed to the review of the manuscript.
Funding This work (SHOP study) was supported by the National Medical Research Council, Singapore (grant no. R-172-003-219-511); the A*STAR-NZ HRC (grant no. JGC 10_027); and the Clinician Scientist Award (CL) to CL, and Singapore Longitudinal Aging Study supported by National Medical Research Council, Singapore (NMRC/CIRG/1348/2012)
; National Medical Research Council (CIRG14may017); and Ministry of Health, Health Services Research - (HSRG0016/2010) to TPN The study sponsors had no role in the design, collection, analysis, interpretation of data, writing of report and decision to submit for publication.Competing interests CL reports grants from National Medical Research Council of Singapore, non-financial support from Boston Scientific, non-financial support from Bayer, non-financial support from Thermofisher, non-financial support from Medtronic, non-financial support from Vifor Pharma, other from Bayer, other from Novartis, other from Takeda, other from Merck, other from Astra Zeneca, other from Janssen Research and Development, other from LLC, other from Menarini, other from Boehringer Ingelheim, other from Abbott Diagnostics, other from Corvia, other from Stealth BioTherapeutics, other from Roche, other from Amgen, outside the submitted work. In addition, CL has a patent PCT/SG2016/050217 pending. CL reports grants from National Medical Research Council, Singapore (grant no. R-172-003-219-511), grants from A*STAR-NZ HRC (grant no. JGC 10_027), grants from Clinician Scientist Award (CL) to CL, TPN reports grants from Singapore Longitudinal Aging Study supported by National Medical Research Council, Singapore (NMRC/CIRG/1348/2012).
Patient consent for publication Not required.
Ethics approval Ethics approval was obtained from the National Healthcare Group Domain Specific Review Board (reference number 2010/00114) and Singhealth Centralised Institutional Review Board (reference number 2010/196/C). Informed consent was obtained from all patients prior to participation.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note All the co-authors listed in this manuscript fulfill criteria of authorship.