Article Text

Abstract
A 58-year-old man presented to the chest pain unit with crescendo angina over 24 hours and worsening dyspnoea of 10 hours duration. He was a known diabetic and hypertensive on regular treatment for 10 years and a habitual smoker with over 15 pack-years smoking duration. Examination revealed a profusely diaphoretic and dyspnoeic (respiratory rate of 45/min) individual with a blood pressure of 100/60 mm Hg and heart rate of 124 beats/min. He was hypoxic and his oxygen saturation in the ambient air was 64%. His jugular venous pressure was elevated with a prominent V wave. Cardiovascular examination revealed a harsh grade IV/VI systolic murmur over the lower left parasternal border. There were bilateral extensive crepitations heard over the lung fields. ECG on admission revealed presence of Q wave and ST elevation in leads II and III, aVF with ST depression in I and aVL. X-ray chest showed normal cardiac shadow and features of grade III pulmonary venous hypertension. Transthoracic echocardiography is shown in figure 1.
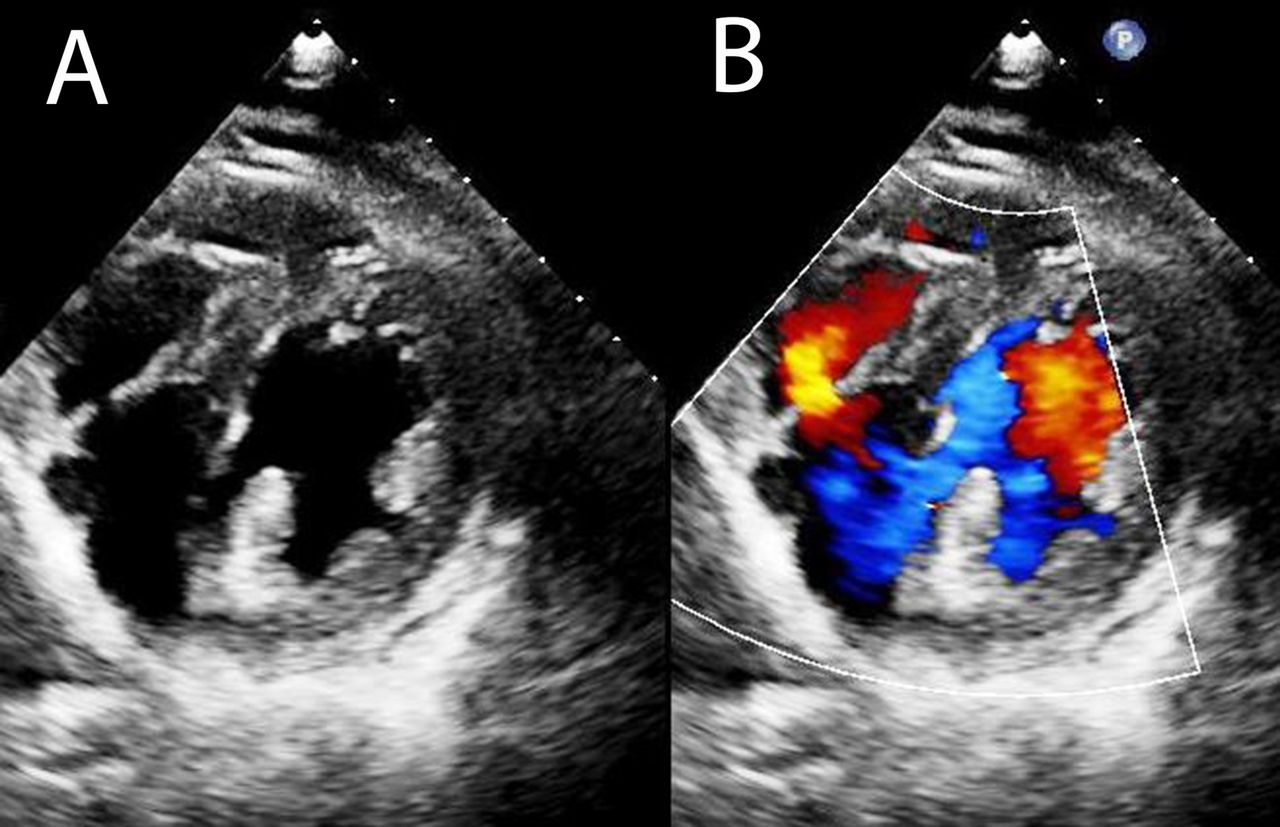
Transthoracic echocardiogram short axis view at mid cavity level, 2D (A) and colour Doppler (B) image.
Question What is the most likely diagnosis?
A. Left ventricular (LV) true aneurysm
B. LV pseudoaneurysm
C. LV pseudo-pseudoaneurysm
D. Ventricular septal rupture (VSR)
E. LV free wall rupture
- transthoracic
- acute coronary syndrome
- STEMI
Statistics from Altmetric.com
Answer: C (LV pseudo-pseudoaneurysm)
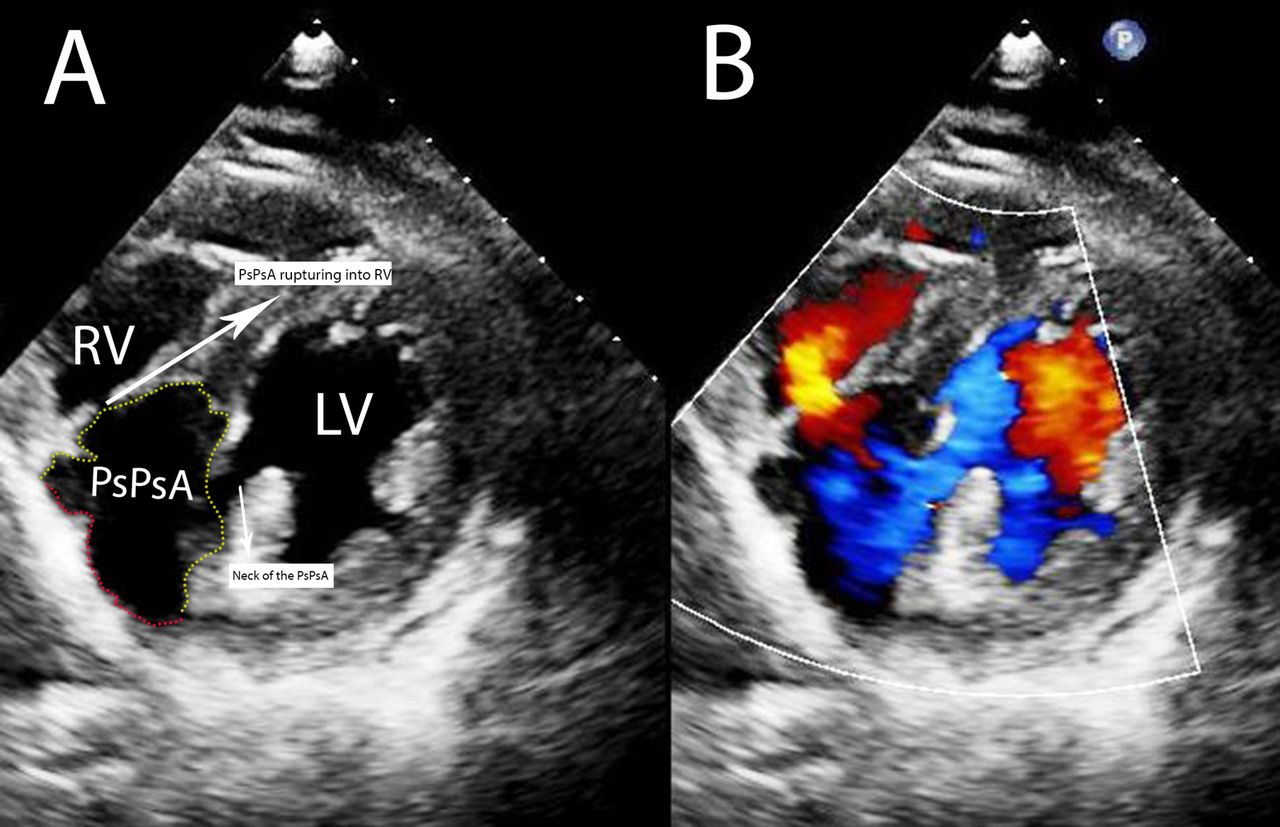
Physical examination and echocardiographic features suggest VSR. However, the echocardiogram (figure 2) clearly demonstrates an aneurysm in the inferoseptal region which communicates with the LV through a narrow neck. The wall of the aneurysm cavity is formed by septal myocardium and pericardium. The cavity finally communicates with the right ventricle (RV) resulting in the VSR (online supplementary videos 1–3).

{kind=link}
{kind=link}
(A) Transthoracic echocardiogram short axis view showing the pseudopseudoaneurysm (PsPsA), LV (Left Ventricle) communicating into the aneurysm through a narrow neck and finally rupturing into the RV (Right Ventricle). Yellow dotted line indicates the aneurysm wall formed by septal myocardium. Red dotted lines indicate the aneurysm wall formed by pericardium and thin layer of myocardium. (B) Colour Doppler image for comparision. LV, left ventricle; RV, right ventricle; PsPsA, pseudo-pseudoneurysm.
Of the mechanical complications, LV free wall rupture is catastrophic. Sometimes the ruptured wall is contained by the pericardium and leads to a pseudoaneurysm. Rarely the rupture is not transmural and is contained within the myocardium itself. Hence, the wall of the aneurysm is formed fully or partly by myocardial layers.1 These entities have been named as pseudo-pseudoaneurysm (PsPsA), pseudofalse aneurysm or subepicardial aneurysm. True aneurysm formation happens because of progressive thinning and scar formation of the myocardium followed by outward pouching of the wall.
PsPsA is extremely a rare clinical entity with only a handful of case reports. The natural course and prognosis of PsPsA is not well known. However, in view of risk of abrupt rupture,2 early surgery is advised. As in our case and the first case report by Stewart et al,3 there is a risk of PsPsA to perforate into the RV.
Supplementary video
Supplementary video
Supplementary video
Footnotes
Contributors PGM was involved in writing and editing of the manuscript, and the management of the patient. GCG was involved in editing and writing of the manuscript. VST was involved in the management of the patient and overall supervision of writing the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.