Article Text

Abstract
Case presentation A 59-year-old man with hypertension, dyslipidemia and a current smoking history had presented with bilateral painful finger ulcers (figure 1A). The patient was referred to our hospital for the diagnosis and treatment. On his arrival, his fingers showed the development from ulcer to necrosis during the 3 weeks (figure 1B). Diagnostic angiography at the previous hospital had revealed symmetrical occlusions of the forearm and crural arteries (figure 2). Laboratory blood tests demonstrated an eosinophilia (21 %, 1743 cells/µL) with marked elevation of IgE (4200 mg/dL) as well as inflammatory reaction such as erythrocyte sedimentation rate 84 mm/h and C-reactive protein 0.85 mg/dL. There was no evidence of thrombophilia, and autoantibodies were negative. A skin biopsy from the border of the necrosis demonstrated perivascular considerable infiltration of inflammatory cells including eosinophils (figure 3).

(A) Initial manifestation at the previous hospital. Note the ulcers in the bilateral fingers. (B) Development to finger necrosis on his admission in our hospital.

(A) Upper extremity angiography revealed extensive occlusions in the bilateral radial and ulnar arteries (arrow). (B) Lower extremity angiography revealed multiple occlusions in the right anterior tibial artery, the left anterior tibial artery and the left posterior tibial artery (arrow).
{kind=link}
{kind=link}
{kind=link}
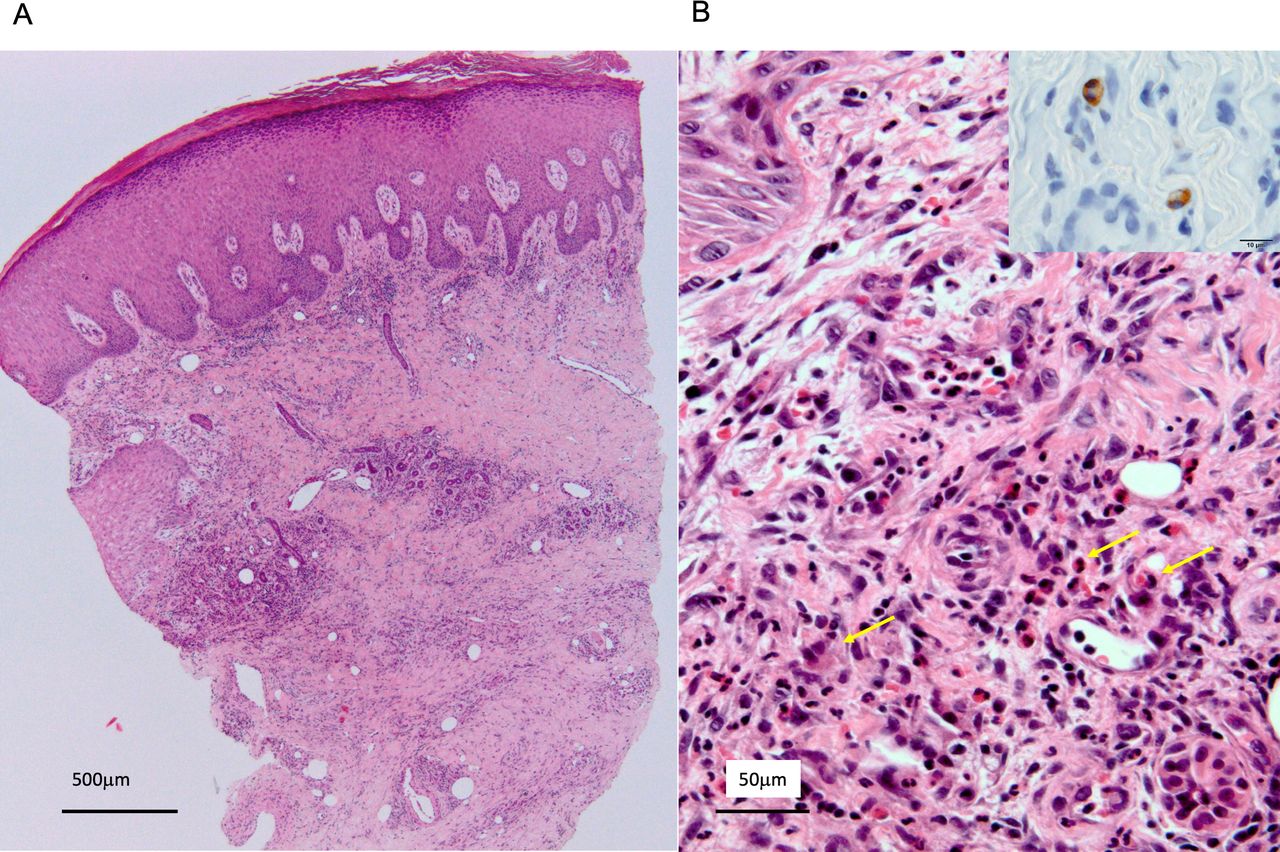
(A) Skin biopsy from the border of the finger necrosis demonstrated nodular inflammatory cell infiltration in dermis and subcutaneous tissue (H&E stain). (B) Magnified histopathological examination of the skin biopsy found eosinophilic infiltration (arrows) in granulomatous inflammation of upper dermis (H&E stain). Immunohistochemistry (inset) showing major basic protein of eosinophils (immunostaining).
Question What is the most likely diagnosis?
Buerger’s disease
Eosinophilic vasculitis
Drug abuse
Cholesterol embolisation syndrome
Paraneoplastic syndrome
- peripheral artery disease
- vasculitis
- eosinophilia
Statistics from Altmetric.com
Footnotes
Collaborators Shinobu Ayabe; Takeshi Yagyu; Hatsue Ishibashi-Ueda.
Contributors RN, TH and OK were involved in the clinical management of the patient. RN drafted and OK revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.