Article Text

Abstract
Case presentation A 59-year-old man with hypertension, dyslipidemia and a current smoking history had presented with bilateral painful finger ulcers (figure 1A). The patient was referred to our hospital for the diagnosis and treatment. On his arrival, his fingers showed the development from ulcer to necrosis during the 3 weeks (figure 1B). Diagnostic angiography at the previous hospital had revealed symmetrical occlusions of the forearm and crural arteries (figure 2). Laboratory blood tests demonstrated an eosinophilia (21 %, 1743 cells/µL) with marked elevation of IgE (4200 mg/dL) as well as inflammatory reaction such as erythrocyte sedimentation rate 84 mm/h and C-reactive protein 0.85 mg/dL. There was no evidence of thrombophilia, and autoantibodies were negative. A skin biopsy from the border of the necrosis demonstrated perivascular considerable infiltration of inflammatory cells including eosinophils (figure 3).

(A) Initial manifestation at the previous hospital. Note the ulcers in the bilateral fingers. (B) Development to finger necrosis on his admission in our hospital.

(A) Upper extremity angiography revealed extensive occlusions in the bilateral radial and ulnar arteries (arrow). (B) Lower extremity angiography revealed multiple occlusions in the right anterior tibial artery, the left anterior tibial artery and the left posterior tibial artery (arrow).
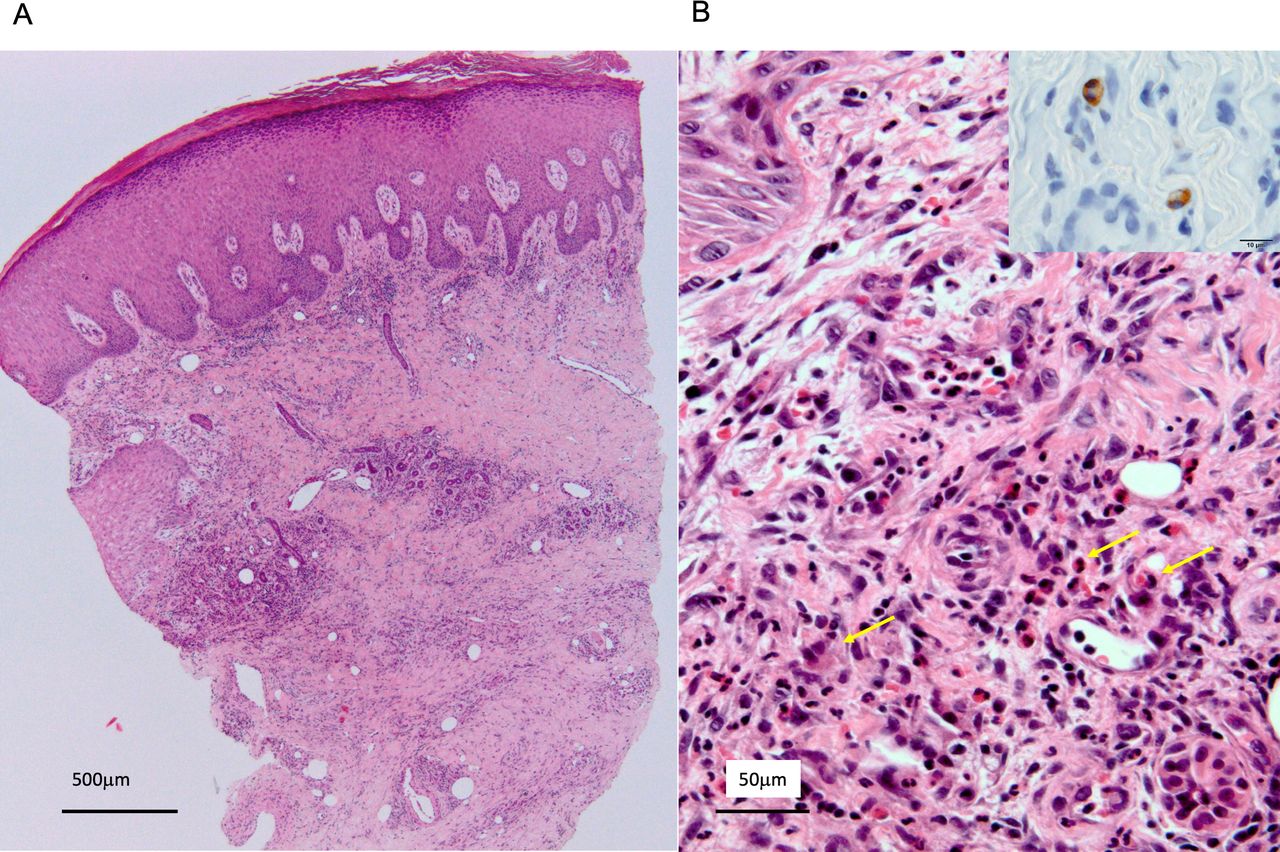
(A) Skin biopsy from the border of the finger necrosis demonstrated nodular inflammatory cell infiltration in dermis and subcutaneous tissue (H&E stain). (B) Magnified histopathological examination of the skin biopsy found eosinophilic infiltration (arrows) in granulomatous inflammation of upper dermis (H&E stain). Immunohistochemistry (inset) showing major basic protein of eosinophils (immunostaining).
Question What is the most likely diagnosis?
Buerger’s disease
Eosinophilic vasculitis
Drug abuse
Cholesterol embolisation syndrome
Paraneoplastic syndrome
- peripheral artery disease
- vasculitis
- eosinophilia
Statistics from Altmetric.com
Answer: B
Finger necrosis and symmetrical occlusion of the peripheral artery can be caused by a wide range of vascular disorders.1 In this case, an evidence of peripheral blood eosinophilia (>10% of total white blood cell) with elevated IgE and perivascular infiltration of eosinophils were the clue to diagnosis.
Eosinophilic vasculitis typically can be caused by two forms; one is idiopathic eosinophilic vasculitis characterised by recurrent episodes of pruritic papules, urticaria and angioedema without immunoserological findings, and another is due to connective tissue disease, eosinophilic granulomatosis with polyangiitis (EGPA).2 In this case, medical history of asthma and lung involvement that are documented in the American College of Rheumatology classification criteria and the Chapel Hill consensus conference definition for EGPA were lacking.3 4 However, given the evidence of eosinophilia with elevated IgE and perivascular eosinophilic infiltration in granulomatous inflammation of dermis on biopsy, multidisciplinary discussion led to the diagnosis of EGPA or a rare entity of eosinophilic vasculitis with thrombotic complication.5 It is recognised that eosinophilic vasculitis is responsive to corticosteroid therapy. Indeed, a high-dose glucocorticoid (prednisone, 0.8 mg/kg/day) was initiated, and no further development of finger necrosis or systemic disorders was observed. His hand skin perfusion pressure was 97/68 mm Hg (palmar/dorsal) in the right and 49/45 mm Hg in the left, suggesting a high likelihood of wound healing. With a tapering prednisone dose, his eosinophilia and inflammation normalised, and medical management facilitated complete wound healing following autoamputation 5 months later (figure 4). No recurrence has been observed during the last 2 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Complete wound healing 5 months later following the initiation of prednisone.
Footnotes
Collaborators Shinobu Ayabe; Takeshi Yagyu; Hatsue Ishibashi-Ueda.
Contributors RN, TH and OK were involved in the clinical management of the patient. RN drafted and OK revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.