Article Text

Abstract
Objective The purpose of this study was to elucidate the role of ghrelin after acute myocardial infarction (AMI) in left ventricular (LV) remodelling.
Design Prospective observational study.
Setting Jichi Medical University Hospital.
Patients Fifty consecutive patients experiencing their first AMI.
Interventions Ghrelin was measured on the day of admission, day 7, day 14 and 6 months after AMI. Patients were treated by percutaneous coronary intervention, and successful myocardial reperfusion was accomplished within 12 h after onset. To analyse LV remodelling, the authors performed left ventriculographies on the day of admission and 6 months after AMI.
Main outcome measures Changes in LV volume.
Results Plasma ghrelin increased significantly after AMI (admission: 40.9±7.3; day 7: 89.5±11.0; day 14: 92.6±11.8 fmol/ml, p<0.0001). There was a significant correlation between ghrelin on day 14 and changes in LV volume over 6 months (r=+0.46, p<0.001). Multivariate regression analysis showed that ghrelin on day 14 is a significant predictor of LV remodelling after AMI (β=+0.44, p=0.001).
Conclusion To our knowledge, this is the first report that shows a relation between circulating ghrelin after AMI and the progression of LV remodelling in the chronic phase. The elevation of ghrelin after AMI might be a compensatory mechanism to attenuate LV remodelling.
- Acute coronary syndromes
- Acute coronary syndrome
- Ghrelin
- Metabolism
- Myocardial ischaemia
- Ventricular remodelling
- AMI
- acute myocardial infarction
- BMI
- body mass index
- CPK-AUC
- creatine phosphokinase-area under the curve
- CRP
- C-reactive protein
- GH
- growth hormone
- IGF-1
- insulin-like growth factor-1
- LV
- left ventricular
- LVEDVI
- left ventricular end-diastolic volume index
- LVEF
- left ventricular ejection fraction
- PCI
- percutaneous coronary intervention
Statistics from Altmetric.com
- Acute coronary syndromes
- Acute coronary syndrome
- Ghrelin
- Metabolism
- Myocardial ischaemia
- Ventricular remodelling
- AMI
- acute myocardial infarction
- BMI
- body mass index
- CPK-AUC
- creatine phosphokinase-area under the curve
- CRP
- C-reactive protein
- GH
- growth hormone
- IGF-1
- insulin-like growth factor-1
- LV
- left ventricular
- LVEDVI
- left ventricular end-diastolic volume index
- LVEF
- left ventricular ejection fraction
- PCI
- percutaneous coronary intervention
Introduction
Left ventricular (LV) remodelling after acute myocardial infarction (AMI) is a serious complication that causes thrombosis, chronic heart failure and ventricular arrhythmia, leading to an unfavourable clinical outcome.1 2 In particular, the size of the infarction determined within several hours after the attack is the most critical determinant of subsequent heart failure;3 however, mechanical factors, medical interventions and humoural factors, such as vasoactive substances and cytokines, have been reported to be associated with LV remodelling in the chronic phase after AMI.4–6
Ghrelin is a novel growth hormone (GH)-releasing peptide, originally isolated from the stomach, which has been identified as an endogenous ligand for the GH secretagogue receptor.7 The biological actions of ghrelin are exerted by two mechanisms; GH-dependent and independent pathways. GH and its mediator, insulin-like growth factor-1 (IGF-1), are anabolic hormones that are essential for skeletal and myocardial growth and metabolic homeostasis.8 9 Considering the anabolic effects of GH/IGF-1, ghrelin may have beneficial effects on cardiac function and cardiac cachexia through a GH-dependent mechanism. On the other hand, ghrelin may have direct metabolic effects through GH-independent mechanisms such as anti-inflammatory actions,10 attenuation of cellular apoptosis,11 inhibition of sympathetic nerve activities12 and orexigenic effects.13 These GH-independent effects might be beneficial against serious complications such as cardiac cachexia and the progression of LV remodelling after AMI. Soeki et al recently reported that exogenous ghrelin administration attenuated LV remodelling after myocardial infarction in rats;14 however, the changes in internal ghrelin levels after AMI and its pathological role are still not fully understood. Therefore, we hypothesised that circulating ghrelin after AMI plays an important role in the progression of LV remodelling by its physiological actions. We conducted a prospective study to measure plasma total ghrelin levels after AMI and to investigate the relationships between ghrelin and LV remodelling in the chronic phase.
Subjects and methods
The Ethics Committee of Jichi Medical School approved the protocol of this study. All patients enrolled in this study gave informed consent. This investigation conforms to the principles outlined in the Declaration of Helsinki.15
Patients
We studied consecutive patients experiencing their first AMI (n=50, 41 male and 9 female, aged 62.9±10.2 years, ranging from 36 to 78 years) admitted to Jichi Medical University Hospital from March 2005 to March 2008. All patients had received percutaneous coronary intervention (PCI). Successful coronary recanalisation was accomplished within 12 h after onset. The definition of AMI followed the description by Anderson et al.16 We excluded patients with collagen disease, inflammatory disease, malignancy, old myocardial infarction, renal failure, significant valvular heart disease and those taking immunosuppressive drugs. Hypertension, diabetes mellitus and dyslipidaemia were diagnosed according to the criteria by Ninomiya et al.17
Blood collection and hormone measurements
Peripheral blood was taken from patients on the day of admission, day 7, 14 and 6 months after onset. We collected peripheral blood in the morning on day 7, day 14 and 6 months in the fasting condition. Anticoagulated samples were then centrifuged immediately at 1000g (4°C, 15 min) and stored at −80°C until the assay. We measured the plasma levels of acylated, des-acyl ghrelin and IGF-1 by enzyme-linked immunosorbent assay according to the manufacturer's instructions (Acylated and des-acyl ghrelin; Mitsubishi Kagaku Iatron, Tokyo, IGF-1; R&D Systems, Minneapolis, Minnesota). The lower limits of acylated, des-acyl ghrelin and IGF-1 were 2.5 fmol/ml, 12.5 fmol/ml and 0.026 ng/ml, respectively. We recognised total ghrelin levels as acylated plus des-acyl ghrelin levels. The creatine phosphokinase-area under the curve (CPK-AUC) was computed by numerical integration with a zero-line of 100 IU/l by Prism (Graph Pad Software, San Diego, California).18 Values were calculated in IU/ml×h.
Evaluation of left ventricular remodelling
To analyse LV remodelling, all patients submitted to two serial left ventriculographies carried out on the day of admission and 6 months after onset (mean 204±45 days). Left ventricular ejection fraction (LVEF) and left ventricular end-diastolic volume index (LVEDVI) were calculated by the area-length method (QCA-CMS, Version 5.1, Medis, Nuenen, The Netherlands). Data were evaluated by a single blinded observer.
Statistical analysis
All values are expressed as the mean±SEM unless otherwise indicated. The significance of differences between two groups was determined by unpaired t test. If samples from groups did not follow Gaussian distribution, the significance of differences between the two groups was analysed by Mann–Whitney U test. Changes in plasma hormone levels were evaluated by one-way analysis of variance with repeated measures. Multivariate regression analysis was used to evaluate significant variables contributing to LV remodelling. Candidate variables possibly associated with LV remodelling (p<0.25 after univariate analysis or unpaired t test) were included in the multivariate models. Values of p<0.05 were considered significant.
Results
Basic characteristics of subjects
In 50 patients with AMI enrolled in the study, body mass index (BMI) on admission was 23.8±3.4 kg/m2, and BMI at 6 months was 23.9±3.4 kg/m2. Thirty-four patients were complicated with hypertension (68%), 15 with diabetes (30%), 28 with dyslipidaemia (56%), 34 were current smokers (68%) and 12 had a family history of coronary artery disease (24%). Thirty-two had anterior, and 18 had other sites of infarction. Thirty-one patients had one-vessel disease, and 19 patients had two-vessel disease. Their symptom-onset-to-balloon time was 4.7±2.1 h. Their LVEF ranged from 32 to 73, with a mean of 52.8%. Their CPK-AUC was 98 518±9250 IU*h/l, and the maximum C-reactive protein (CRP) was 7.37±0.79 mg/dl. After PCI, β-blockers were prescribed to 28 patients, calcium-channel blockers to five patients, diuretics to four patients, nitrates to seven patients, rennin–angiotensin system inhibitors to 43 patients and statins to 36 patients. In the acute phase, catecholamine were given intravenously to four patients, nicorandil to 14 patients and nitroglycerine to 14 patients, and intra-aortic balloon pumping was used for 17 patients. All patients had a single culprit lesion in the coronary artery. No patient was lost during the follow-up period. Follow-up coronary angiography revealed that all treated coronary lesions were patent 6 months after AMI. No death, heart failure or readmission occurred during the study period.
Changes in plasma hormone levels
Figure 1 shows the time course of the changes in plasma levels of total ghrelin during 6 months after AMI. As GH is difficult to measure because of instability and large diurnal change, we measured IGF-1, which is secreted from the liver in response to GH. Total ghrelin and IGF-1 levels increased significantly after the onset of AMI (total ghrelin; admission: 40.9±7.3; day 7: 89.5±11.0; day 14: 92.6±11.8 fmol/ml, p <0.0001, IGF-1; admission: 49.5±2.8; day 7: 54.3±2.8; day 14: 66.8±3.9 ng/ml, p<0.001). Total ghrelin and IGF-1 levels decreased after 6 months (total ghrelin on 6 months: 54.8±5.8 fmol/ml, IGF-1 on 6 months: 49.4±2.3 ng/ml). We found a significant positive correlation between maximum leucocyte counts and total ghrelin levels on day 14 (r=+0.30, p=0.03). A positive correlation was also found between CRP levels on day 14 and total ghrelin levels on day 14 with marginal significance (r=+0.28, p=0.07). We did not find any significant correlations between total ghrelin levels and other clinical parameters such as age, gender, BMI, coronary risk factors, the number of diseased vessels, symptom-onset-to-balloon time, LVEF, CPK-AUC and the treatment used.

Time course of plasma total ghrelin levels after acute myocardial infarction. The figure shows the time course of plasma total ghrelin levels after the onset of acute myocardial infarction (admission: 40.9±7.3; day 7: 89.5±11.0; day 14: 92.6±11.8; 6 months: 54.8±5.8 fmol/ml). *p<0.0001 versus day 1, p<0.001 versus 6 months.
Changes in left ventricular volume during the study period
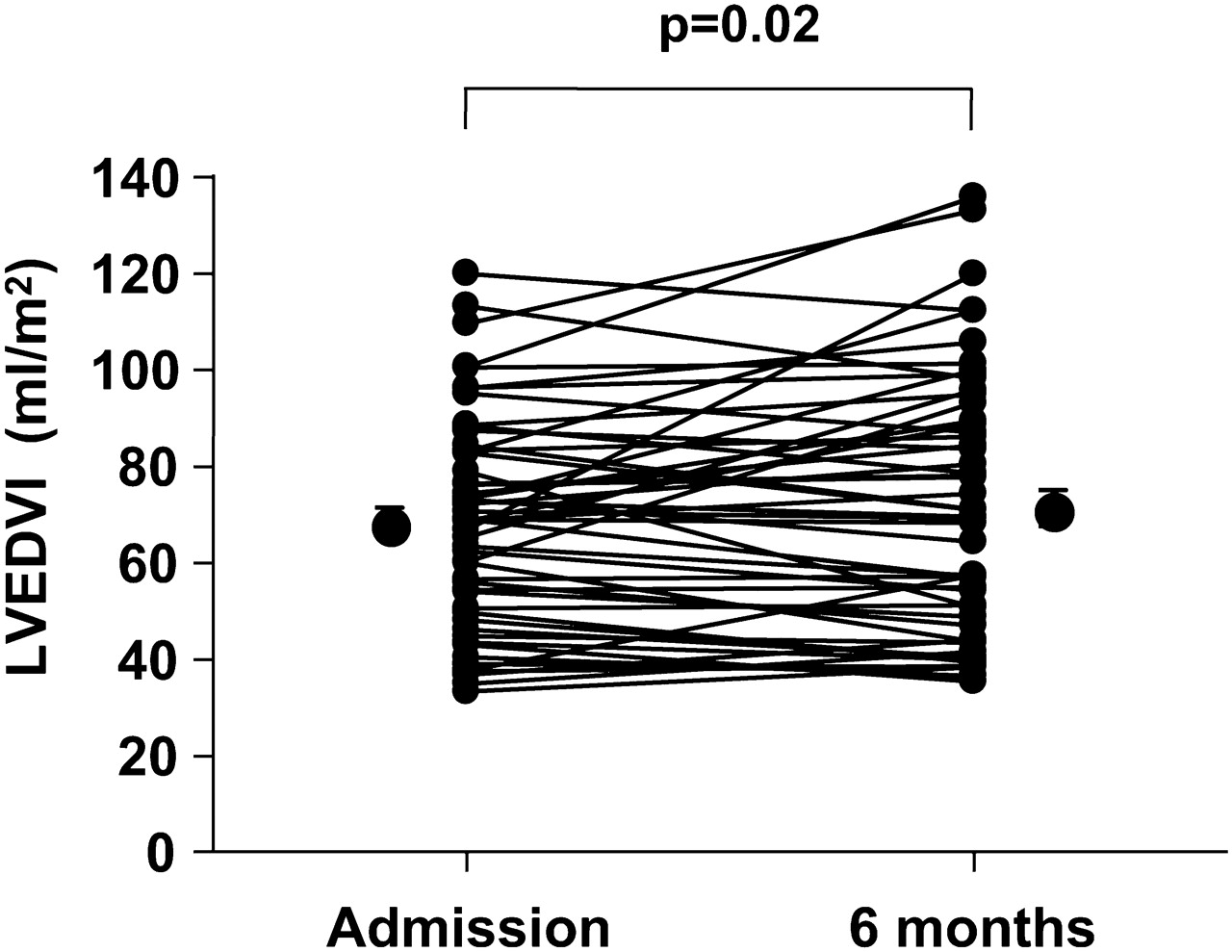
Figure 2 shows changes in LVEDVI during the study period. Overall, LVEDVI increased significantly in the study subjects (admission: 74.4±3.0, 6 months: 79.8±3.6 ml/m2, p=0.02). LVEDVI increased in 29 patients, but did not increase in the remaining 21 patients.
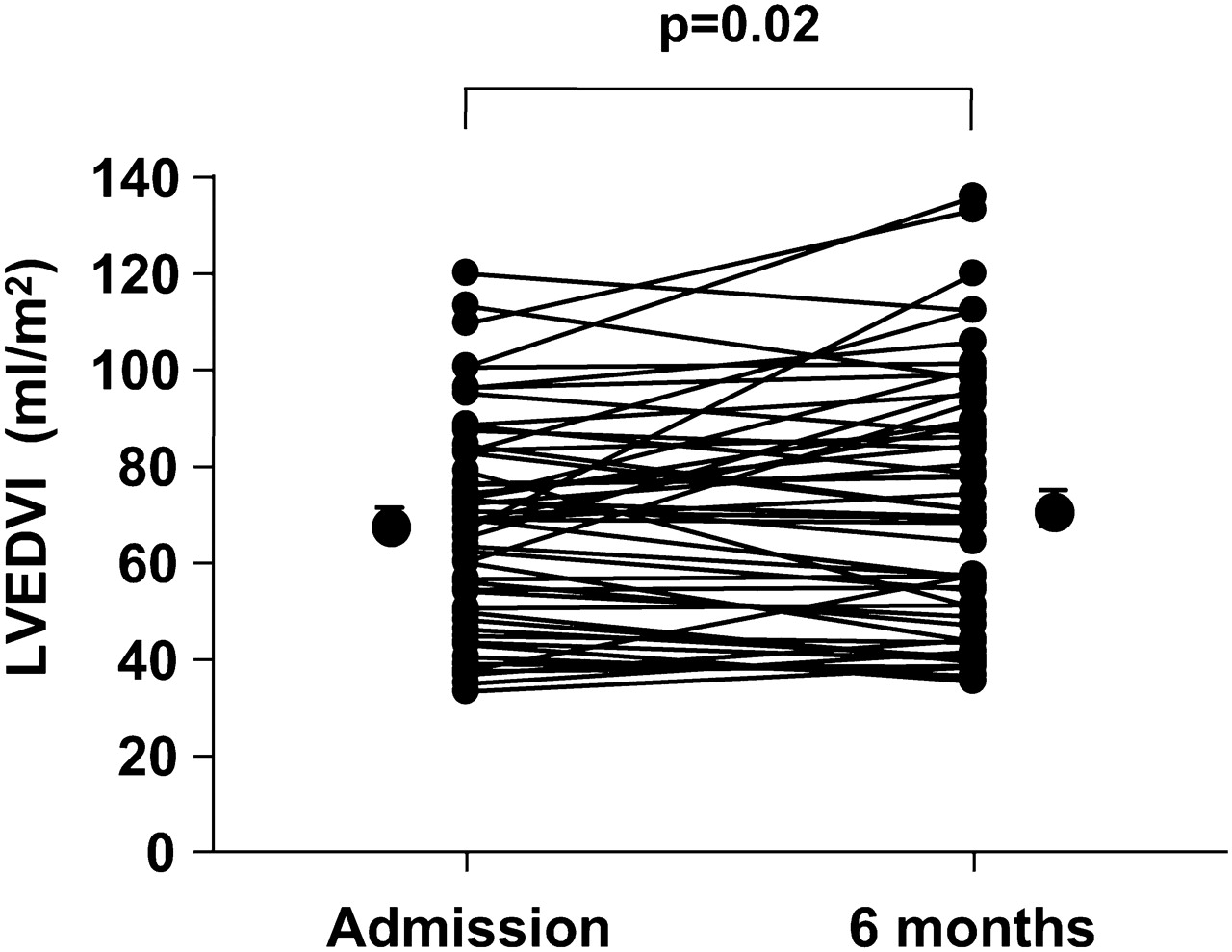
Changes in left ventricular end-diastolic volume index during the study period. The figure shows changes in left ventricular end-diastolic volume index (LVEDVI) in the study subjects. LVEDVI increased significantly during the study period (admission: 74.4±3.0; 6 months: 79.8±3.6 ml/m2, p=0.02).
Predictive value for left ventricular remodelling
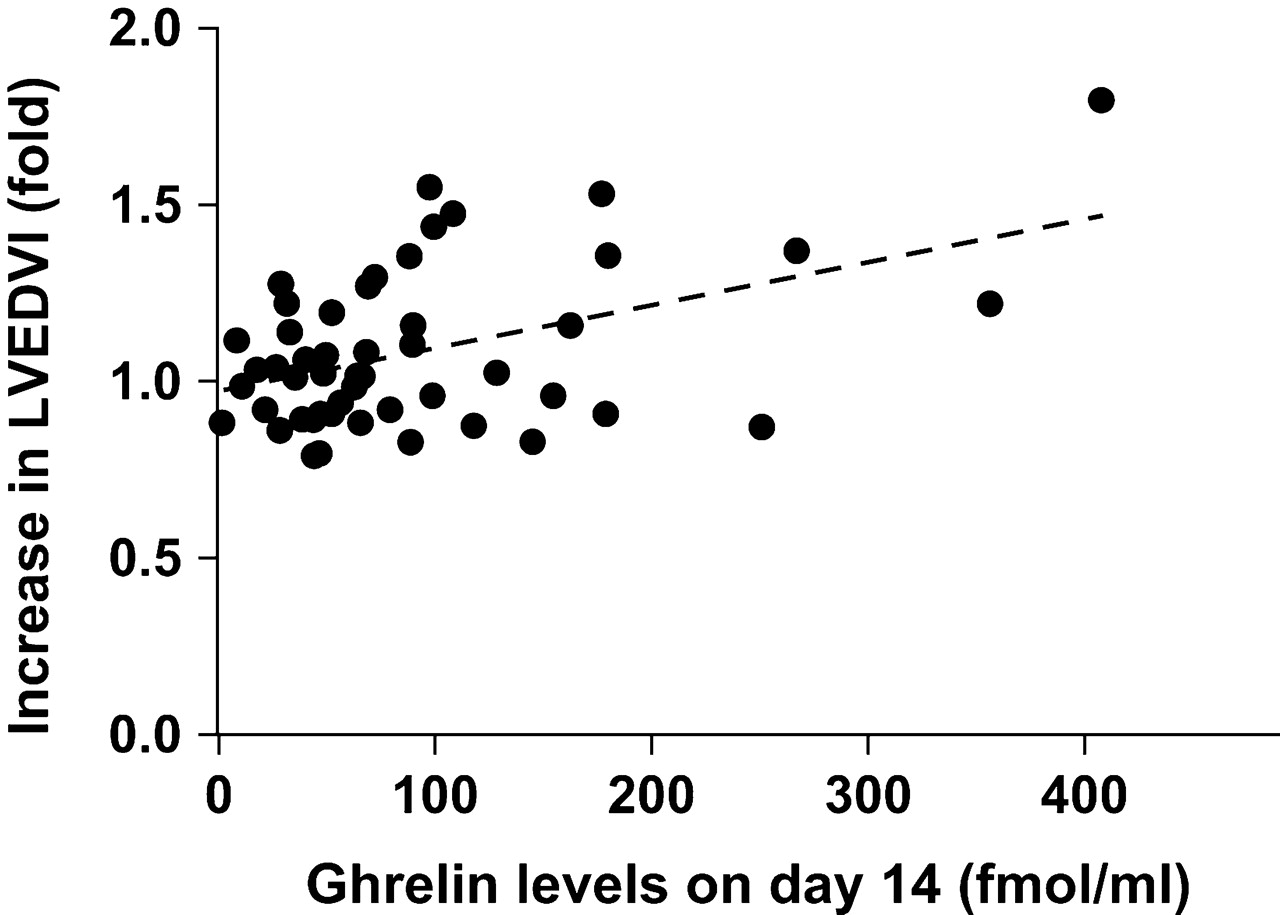
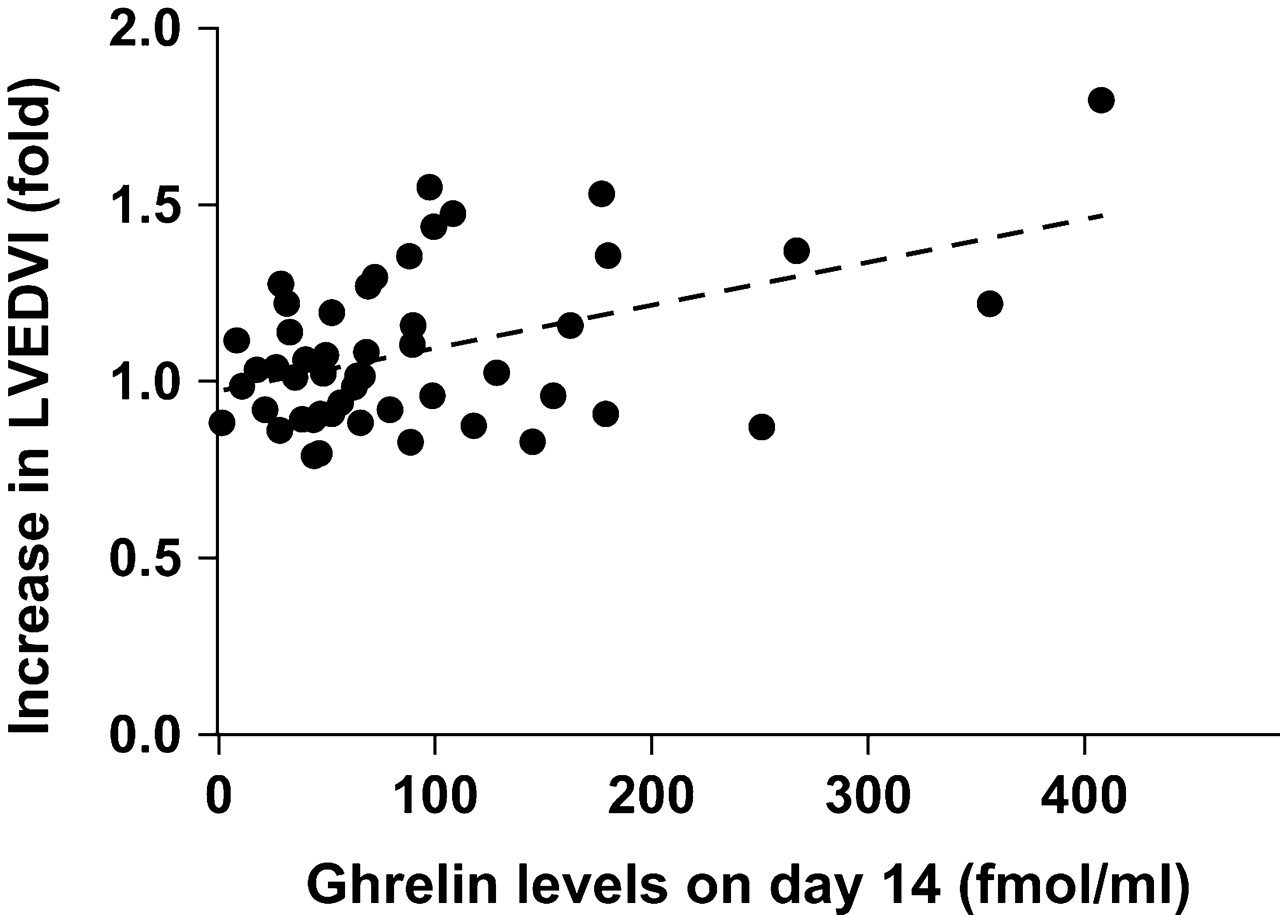
We conducted a regression analysis to determine significant factors that contribute to LV remodelling. We examined the simple correlation between continuous clinical parameters (age, BMI, symptom-onset-to-balloon time, LVEF, maximum leucocyte levels, CPK-AUC and CRP levels on day 14) and fold increase in LVEDVI over 6 months (table 1). We found a significant negative correlation between BMI and the fold increase in LVEDVI. We also found a positive correlation between LVEF and the fold increase in LVEDVI. We divided patients into two groups according to the categorical variables (gender, hypertension, diabetes, site of infarction, the number of diseased vessels, medications and the usage of intra-aortic balloon pumping). We conducted an unpaired t test to compare changes in LVEDVI in the two groups. Ther fold increase in LVEDVI in patients taking diuretics was significantly higher than that in patients not taking diuretics (1.41 in patients taking diuretics versus 1.06 in those not taking diuretics, p=0.01). Next, we examined the correlation between hormone levels and the fold increase in LVEDVI. As shown in table 2 and figure 3, a significant positive correlation was observed between plasma total ghrelin levels on day 14 and the fold increase in LVEDVI (r=+0.46, p<0.001).
Correlation between clinical parameters and fold increase in left-ventricular end-diastolic volume over 6 months
Correlation coefficient between hormone levels and changes in left-ventricular end-diastolic volume
{kind=link}
{kind=link}
{kind=link}
Relationship between plasma total ghrelin levels and left ventricular remodelling after acute myocardial infarction. The figure shows a simple correlation between plasma total ghrelin levels on day 14 and the fold increase in left ventricular end-diastolic volume index (LVEDVI) over 6 months after the onset of acute myocardial infarction. There was a significant positive correlation between plasma total ghrelin levels on day 14 and the fold increase in LVEDVI over 6 months (r=+0.46, p<0.001).
Then, we performed a stepwise multivariate regression analysis with the forward entry method to determine significant independent variables contributing to LV remodelling. In this model, we set the fold increase in LVEDVI as a responsive variable and gender, BMI, symptom-onset-to-balloon time, LVEF, CPK-AUC, CRP levels on day 14, total ghrelin levels on day 14, intravenously administered nitroglycerine and taking medications such as diuretics, rennin-angiotensin system inhibitors and β-blockers as explanatory variables. Because of their clinical relevance and potential importance, symptom-onset-to-balloon time and taking β-blockers were retained in the multivariate models as explanatory variables regardless of statistical significance. Dummy variables were used as categorical variables in the model. By multivariate analysis, CPK-AUC and plasma total ghrelin levels on day 14 were significant predictors for an increase in LVEDVI (F=10.38, p=0.002, table 3).
Results of multivariate stepwise regression analysis
Discussion
The findings from this prospective study can be summarised as follows: (1) plasma ghrelin levels increased significantly by day 14 after the onset of AMI; (2) a significant positive correlation was found between plasma ghrelin levels on day 14 and inflammatory markers; (3) a significant positive correlation was found between plasma ghrelin levels on day 14 and the increase in LVEDVI over 6 months after AMI; (4) multivariate regression analysis revealed that LVEF, CPK-AUC and plasma ghrelin levels on day 14 were significant predicting factors for LV remodelling after AMI. These results indicate that circulating ghrelin after AMI has an important role in the progression of LV remodelling by its physiological actions.
After AMI, inflammation begins to normalise in the subacute phase. It has been reported that large infarction and sustained myocardial stress induce chronic inflammation in the non-infarcted myocardium, contributing to late LV remodelling after AMI.19 In addition, chronic inflammation has been associated with weight loss and cardiac cachexia.20 21 Recent studies showed that low BMI was associated with increased mortality after AMI.22 23 Certainly, these data indicate that patients with low BMI tend to show the progression of LV remodelling. In this study, a positive correlation was found between plasma ghrelin levels and inflammatory markers not only in the acute phase but also in the subacute phase. Our findings suggest that inflammation after AMI might be involved in increased ghrelin production.
In animal models, exogenous ghrelin administration attenuated LV remodelling after AMI.14 In addition, peripheral and intracerebroventricular administration of ghrelin has been shown to stimulate food intake and increase body weight through a GH-independent mechanism.24 In patients with chronic heart failure, administration of ghrelin for 3 weeks tended to increase body weight and significantly increased lean body mass and muscle strength.25 Thus, ghrelin might attenuate the progression of LV remodelling and the development of cardiac cachexia after AMI. Interestingly, we found a positive correlation between an increase in body weight during the study period and plasma total ghrelin levels on day 14 with marginal statistical significance (r=+0.27, p=0.06). Considering this finding, elevated ghrelin might be able to control the development of cardiac cachexia after AMI. These findings suggest that the sustained elevation of plasma ghrelin levels might be one of the compensatory mechanisms against not only cardiac cachexia but also the progression of LV remodelling after AMI. It is possible that adequate supplementation of ghrelin could also attenuate the progression of LV remodelling after AMI.
We did not find a significant relationship between plasma IGF-1 levels and LV remodelling; therefore, GH-independent effects of ghrelin, such as the attenuation of sympathetic nerve activities, vasodilatation, inhibition of cell apoptosis and orexigenic effects might be important compensatory mechanisms to prevent LV remodelling after AMI.10–13 In addition, we did not find any significant relationship between total ghrelin levels on the day of admission and day 7 after AMI and LV remodelling, suggesting that sustained elevation of ghrelin might be an important clinical marker representing the progression of LV remodelling in the chronic phase.
Study limitations
First, the active form of ghrelin, the Ser3 residue, modified by n-octanoid acid, was almost undetectable in all study subjects because of its instability. The active form of ghrelin has a half-life of approximately 10 to 30 min.25 26 In this study, we recognised total ghrelin levels as active plus des-acyl ghrelin levels. Further studies should be conducted to clarify the role of active ghrelin after AMI. Second, it was not possible to control for diet status on admission. Plasma ghrelin levels increased in response to fasting and decreased upon feeding. To avoid changes in plasma ghrelin levels by food intake, we collected the peripheral blood in the fasting state on days 7 and 14, and 6 months after AMI. Third, we could not analyse the association between treatment given after AMI and the changes in plasma ghrelin levels. It is possible that medical treatment affects plasma ghrelin levels. Recently it was reported that rikkunshito, a herbal medicine, alleviated the gastrointestinal disorders through ghrelin release.27 Further studies are needed to reveal the treatment effect on plasma ghrelin levels after AMI. Finally, we should investigate the role of ghrelin in the long-term prognosis of AMI patients.
Conclusions
To the best of our knowledge, this is the first report of circulating ghrelin after AMI associated with the progression of LV remodelling in the chronic phase by its physiological actions. Although the regulatory mechanisms of ghrelin after AMI remain unclear, plasma ghrelin levels provide prognostic information for LV remodelling in the chronic phase. Adequate supplementation of ghrelin after AMI may be a new therapeutic approach to prevent serious complications after AMI.
Acknowledgments
We thank T Takagi, for her excellent technical assistance.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the Ethics Committee of Jichi Medical University.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.