Article Text

Abstract
Revascularisation by percutaneous coronary intervention (PCI) in chronic total occlusion (CTO) is often a technically challenging procedure. The manipulation of wires and devices through a CTO during PCI without any means to visually identify vessel-wall boundaries involves an inherent risk of complications such as arterial dissection, perforation and cardiac tamponade. With the tremendous advances in multidetector CT technology and the popularity of utilising coronary CT angiogram (CCTA) for a workup of chest pain patients, an increasing number of CTO cases are being encountered. Therefore, the primary goal of CCTA for imaging in CTOs involves identifying the presence and locations of CTO as well as predicting the potential clinical benefits derived from revascularisation of the occluded segment. The secondary goal includes preprocedural planning to shorten procedure times, visualisation of the procedure in predicting the ease with which a CTO can be crossed and the frequency of procedure-related complications such as contrast nephropathy and radiation skin injury. Apart from these, CCTA also plays a role in postprocedural assessment of the revascularised arterial segments and long-term follow-up on the patency of coronary stents.
- Angina
- cardiac imaging
- coronary stenting
Statistics from Altmetric.com
Introduction
Chronic total occlusion (CTO) is diagnosed when complete obstruction of a coronary artery is present for 3 months or more from the estimated clinical events or proven by previous angiography.1 In a large registry of more than 6000 patients, it has been reported that one CTO was found in 52% of those patients with significant coronary artery disease defined as a diameter stenosis of at least 70% on coronary angiograms.2 Successful treatment of CTO has been shown to be beneficial with improvements in angina symptoms, ventricular ejection fraction and long-term survival.3–5 However, the procedure tends to be time-consuming, and the failure rate remains high6 7 despite various technological advances especially in guidewire technology for crossing the occluded segment. Multidetector-row computed tomography technology has gone through tremendous advances in the last decade. We review the application of a coronary CT angiogram (CCTA) in patients with CTO, especially in better predicting chance of successful revascularisation and guiding the intervention procedure.
Definition of CTO
The literature reveals a number of ways of defining a CTO, with some authors defining chronic total occlusions of the coronary arteries as the obstruction of the native coronary artery with no luminal continuity and interruption of antegrade blood flow diagnosed by coronary angiography with thrombolysis in myocardial infarction (TIMI) grade 0 flow; on the other hand, it also includes TIMI grade 1 flow, showing minimial contrast penetration through the lesion without distal vessel opacification, and an occlusion period of 1–3 months estimated from the clinical events or proven by previous angiography. Since the time of occlusion is not always known, the consensus is to define a CTO as ‘the presence of TIMI 0 flow within the occluded segment with an estimated occlusion duration of ≥3 months.’1
Current therapeutic strategy of CTO
The clinical presentation of a CTO can be very variable. On the one hand, there are patients with new-onset angina and ischaemic heart failure, while on the other hand, there are patients with silent ischaemia or undergoing primary percutaneous coronary intervention (PCI) due to acute occlusion in a different culprit vessel, and the CTO is just an incidental finding.
Despite the availability of better guiding catheters, advancement in guidewire technology and angiographic techniques, PCI of CTO remains a major challenge for interventional cardiologists. The major determining factor of a successful procedure lies on the capability of crossing the CTO lesion with a guidewire.8 9 This most technical challenging procedure was reported to be approximately 60–80% and is much lower than the other lesion subsets.10–12 Furthermore, PCI to CTO is a procedure not without complication risk. In fact, in excess of 5% major in-hospital adverse events were reported previously.10 13 14 On the contrary, conservative therapy to CTO may not always be the best treatment option to these group of patients. Several studies have shown that successful revascularisation of CTOs by PCI has been associated with an improvement in angina, left ventricular systolic function, avoidance of bypass surgery and possibly reduced mortality and complications in case of future acute events.3–5 9–11 Therefore, correct patient selection for these procedures are of utmost important. PCI to CTO is considered warranted when the occluded vessel is responsible for ischaemic symptoms, the likelihood of successful procedure is at least moderately high and the predicted anticipated procedure related risk is low.1 Besides, though the presence of CTO is one of the referral reason for surgical revascularisation procedure in multivessel diseases in the past, it is no longer the case if the patient is free from severe left main disease and the other lesions are amendable by PCI which carries lower procedure risk. The predictors of successfully crossing the wire are therefore essentially helpful for operators to decide on the best revascularisation strategy.
Multidetector CT for coronary arteries
Multidetector-row computed tomography has been shown to have a high sensitivity (>90%) for detection of significant (≥50%) coronary artery luminal stenosis on either an individual patient basis or a named artery basis.15 16 Specificity varies in early studies, while more uniformly good results (∼90%) are seen in recent studies.17 The main technological challenge of cardiac CT is to freeze cardiac motion, which means high temporal resolution. Tube rotation time is the primary determinant of temporal resolution. The G-force generated from spinning a heavy x-ray tube at high speed is enormous. A dual tube (with corresponding detector rings) design is one of the ways to improve the nominal temporal resolution, since each tube has to travel 90° instead of 180° to generate data for one image. The even more recent introduction of 320-detector-row CT practically enables the whole heart to be covered in the detector array (302×0.5 mm) without table movement. Single-heartbeat non-spiral imaging of the whole heart is possible, dramatically reducing artefacts associated with spiral acquisition and step artefacts due to imaging a different part of the heart in different cardiac cycles.18 Dynamic imaging like cardiac perfusion may also find wider application in the near future.
Coronary CT angiogram for CTO
CCTA generates a volumetric data set of the heart, and with present generation of CT scanner using a detector width of ∼0.5 mm, true isotropic voxels make up the whole scanned volume. This means the image can be reconstructed to be viewed in any desired plane with no loss of spatial resolution. This is very important for structures such as coronary arteries, which have a complex 3-D course. Thin slab maximal intensity projection (MIP) images and volume-rendered images can be shown in the same projection angle used for the coronary angiogram and subsequent intervention for direct correlation.
To diagnose occlusion on CCTA, a segment of the coronary artery has to contain no contrast-enhanced lumen (figure 1). As with all CT angiogram examinations, very-high-grade stenosis may not be reliably differentiated from total occlusion. A partial volume effect is commonly cited as the most important reason. CCTA still has a spatial resolution, being only a fraction of the catheter angiogram. The isotropic voxel is ∼0.4–0.5 mm in size and if a contrast-enhancing structure (the patent lumen) is smaller than this, this voxel would have an attenuation in between contrast and the obstructing lesion.19 The blooming effect from calcified plaque can also make visualisation of the residual lumen difficult. That means CCTA tend to make a false-positive diagnosis of occlusion when there is very-high-grade stenosis. However, because segment distal to occlusion can show an enhancement, the unwary interpreter may misdiagnose CTO, especially short ones, as mere high-grade stenosis (figure 2). These limitations would mean that any possible CTO detected on CCTA should be further evaluated by a catheter angiogram.

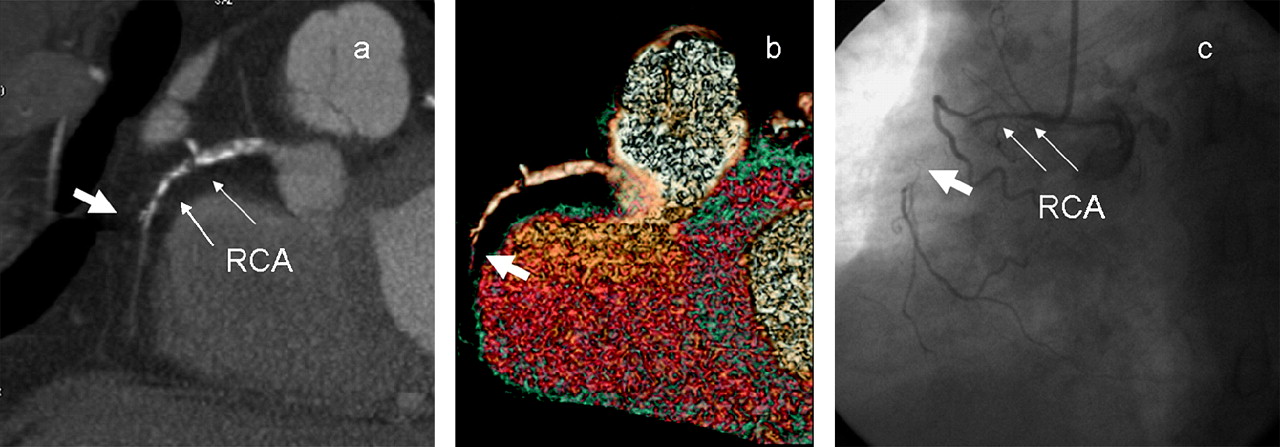
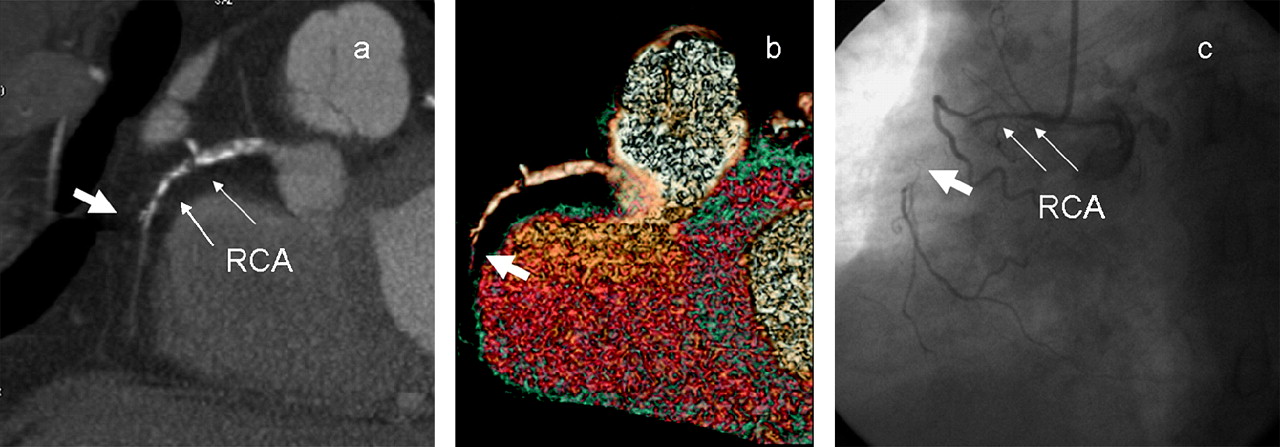
Coronary CT angiogram (CCTA) showing a segment of chronic total occlusion (CTO) in the proximal right coronary artery (RCA). The maximal intensity projection of CCTA (A) shows a segment of CTO as suggested by complete absence of contrast-filled lumen (thick arrow) with eccentric calcified plaques at the proximal margin of the occluded segment of the proximal right coronary artery (thin arrows). The lumen of the artery distal to the occlusion is opacified by contrast due to collateral circulation. The segment of CTO (thick arrow) is easily recognised by three-dimensional volume rendering images (B) of the right coronary artery. The CCTA suggests that PCI is favourable by the presence of a short segment of occlusion and a tapered stump. Conventional coronary angiogram (C) shows the segment of occlusion corresponding to CCTA findings. Percutaneous coronary balloon dilatation was successfully performed, and a drug-eluting stent (Endeavour Resolute 2.5 mm × 18 mm) was implanted to the proximal right coronary artery.

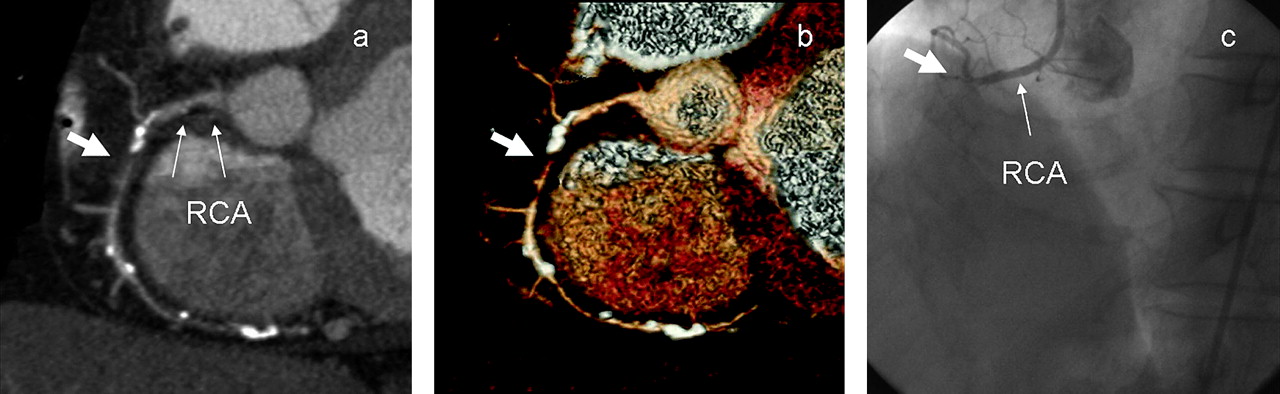
(A)Maximum intensity project: segment of occlusion with calcification at the mid coronary artery. The vessel distal to the occluded segment is opacified with contrast, and a chronic total occlusion is suggested. (B, C) Conventional coronary angiogram showing the presence of a subtotal occlusion (99% stenosis). It demonstrates the difficulty in differentiating between a total or subtotal occlusion by a coronary CT angiogram. RCA, right coronary artery.
It has been shown that the non-enhancing segment is significantly longer in CTO than in high-grade stenosis. A lesion length ≥9 mm was 100% specific for an occlusion. However, a CTO as short as 4 mm has been reported.20 Other parameters assessed including the degree of calcification in the lesion, attenuation of the non-calcified portion of the lesion and the presence of remodelling are not helpful in differentiating between the two conditions. Attenuation of the coronary segment distal to the non-enhancing lesion is generally lower than that proximally in both conditions but shows a greater difference in CTO cases. Further evaluation would be need to determine whether this is significant.
CCTA involves intravenous injection of a tight bolus of contrast material. This is different from the selective arterial injection of catheter coronary angiogram. CCTA offers better visualisation of the occluded segment, since the coronary segment proximal and distal to the occlusion can be easily visualised due to contrast in-flow from collaterals. The length of the occlusion can then be estimated. These are possible in catheter angiograms only when antergrade collaterals are present or with a bilateral coronary injection. The nature of the lesion causing occlusion and morphology of the stump can also be assessed by CCTA, which is intrinsically very sensitive to the presence of calcification.
Predictors to success PCI to CTO by conventional coronary angiography
Angiographic characteristics of CTOs can strongly predict the likelihood of a successful intervention. The adverse factors include a CTO longer than 3 months' duration, a length greater than 15–20 mm, multivessel disease, presence of moderate to severe calcium and absence of a tapered stump.9 21 22 Other features including the presence of bridging collaterals, proximity to a side branch, tortuosity and lack of distal-vessel visibility were suggested to have a predictive value in the success of the procedure.9 22 23 With improvements in intervention devices and new guidewire technology, the main predictors of failure now are calcifications, marked vessel tortuosity and long occlusion length. Although conventional coronary angiography remains the gold reference standard, three-dimensional data are compressed into two-dimensional fluoroscopic projection images. As a result, it is not possible to visualise the true spatial structure from the tremendous overlapping and foreshortening of images. Obviously, no information on plaque characteristics is provided by the coronary angiogram.
Value of CTA on the prediction of successful angioplasty of CTO
A recent study has demonstrated several unfavorable features identified on CCTA in predicting the outcome of PCI on CTO. These include an occlusion length of >15 mm, severe calcification and blunt stump morphology.24 In particular, heavy transluminal calcification (occupying >50% of the cross-sectional area of the lumen) may be highly predictive of procedure failure (figure 3). It was recently reported that CCTA was able to identify the distal vessel and route for PCI in 68%, while the angiogram was able to show a possible coronary route in only 18%.25
{kind=link}
{kind=link}
{kind=link}
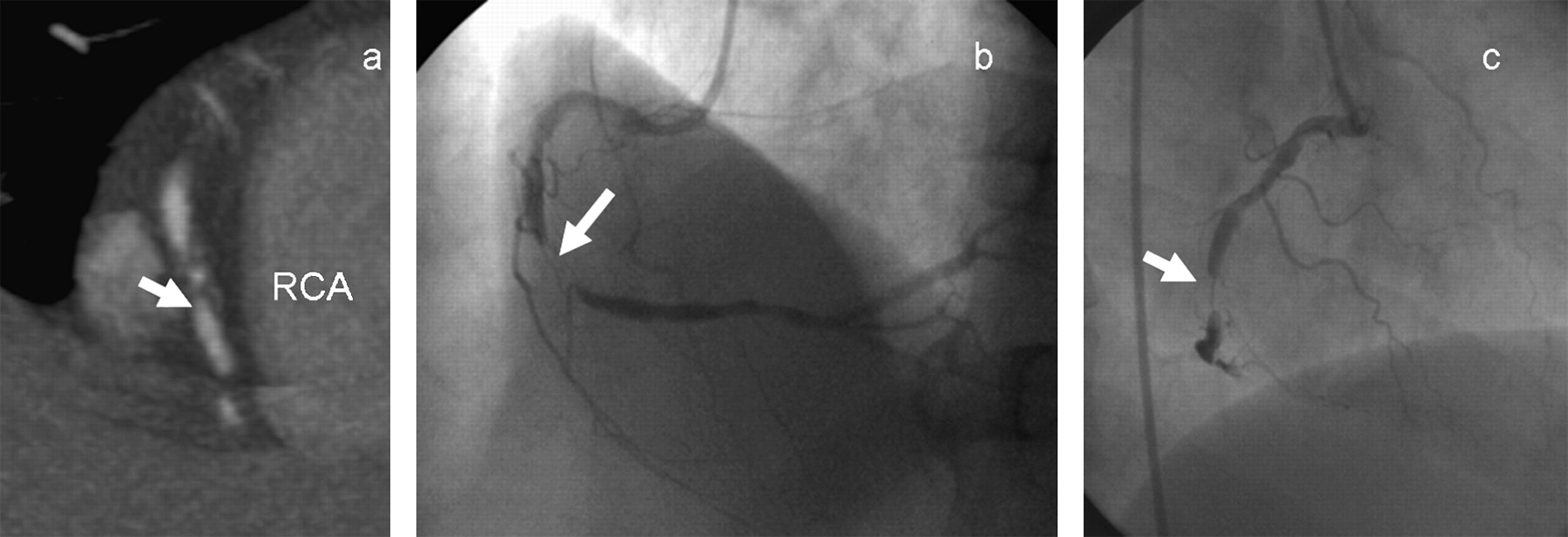
Coronary CT angiogram images showing occlusion of a mid-right coronary artery (RCA) with complete cut-off at the stump of occlusion on the maximum intensity project (A) and three-dimensional volume rendering project images. (B) The distal artery was supplied by the right-to-right and left-to-right collaterals. The occluded segment (thick arrow) is long and with heavy calcification at the proximal margin of the occlusion, which are unfavourable predictors for percutaneous coronary intervention (PCI). A conventional coronary angiogram (C) confirmed the chronic total occlusion at the corresponding position. The PCI was abandoned after the failure of guidewire crossing.
CCTA, as a three-dimensional imaging technique, is most useful in the assessment of the long, tortuous total occlusion and the quality of the distal vessel as well. In addition, the identification of the extent and distribution of calcifications within the occlusion allows interventional cardiologists to carry out more thorough preprocedural planning of interventional strategies, choices of guidewires and devices, and assist the time scheduling of cardiac catherisation laboratory. With advancements the software, some centres have begun to incorporate CCTA images into live fluoroscopic images to create hybrid three-dimensional images.26 The CT scan is used to provide optimal angles from which to approach the CTO by minimising foreshortening and making ‘angiographic-equivalent’ pseudo-projection images to guide the advancement of guidewire.
Viability assessment by CCTA
One of the indications for opening up a CTO is the identification of a viable myocardium in the involved occluded artery. Myocardial viability can be assessed by several imaging modalities in the clinical setting, including stress echocardiography, nuclear imaging such as PET/CT and contrast-enhanced cardiac MRI.27–29 Apart from these, there is increasing awareness of the myocardial perfusion and viability as a one-stop-shop assessment in CCTA. One of the main concerns would be radiation exposure, and this hastened the inclusion of a viability study as part of the routine imaging protocol from majority centres.
Radiation exposure and ways for reduction
As mentioned above, CCTA is a high-dose procedure with retrospective ECG gating. The main reason is the low pitch (∼0.2) that is required to provide the redundant data used to reconstruct images at any time point for any part of the heart and vessels. Scan data from a 180° tube rotation are needed to reconstruct an image. The actual effective radiation dose varies with patient size, heart rate and use of multisegment reconstruction protocol among other factors. It is also higher for the female subjects. An effective dose of 10–15 mSv is typical, which is at least three times higher than for a diagnostic catheter coronary angiogram.30 The more recent introduction of prospectively ECG triggered CCTA using the ‘step and shoot’ approach can dramatically reduce the dose to <5 mSv. The prerequisite for good image quality is a stable and relatively slow heart rate, and the safety margin increases with wider padding, which in turn carries a radiation penalty. Functional information such as ejection fraction is also not available. Before we consider doing CCTA for every patient with CTO, this is a factor to be taken into account.
Conclusion
There is no doubt about the diagnostic performance of CCTA in coronary artery disease.
Furthermore, CCTA is a very useful tool to optimise PCI strategy in CTO, owing to its ability to characterise the length, course and plaque composition at the occluded artery. It also allows a three-dimensional visualisation of the distal run off and the associated side branches. Besides, CCTA could be used as a navigator for the PCI, facilitating best patient population selection, preprocedural planning and better time scheduling of the busy cardiac catherisation laboratories. With the increasing popularity in performing CCTA in patients with atypical chest pain and positive treadmill in the intermediate likelihood group, there will be increasing chances of encountering CTO and its time to equipping ourselves with knowledge on incorporating the usage of CCTA in the management of CTO patients.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; not externally peer reviewed.