Article Text

Statistics from Altmetric.com
- Sinus of valsalva
- aneurysm
- complications
- heart failure
- aortic regurgitation
- aortic root disease
- heart failure
An elderly gentleman presents with worsening shortness of breath on exertion and intermittent chest pain. His background includes a recent diagnosis of myocardial infarction, previous deep venous thrombosis, ulcerative colitis and hypertension. His clinical findings were consistent with left ventricular failure with a significant aortic regurgitation murmur. He also has a longstanding abnormal ECG consistent with left ventricular hypertrophy and pulmonary hypertension.
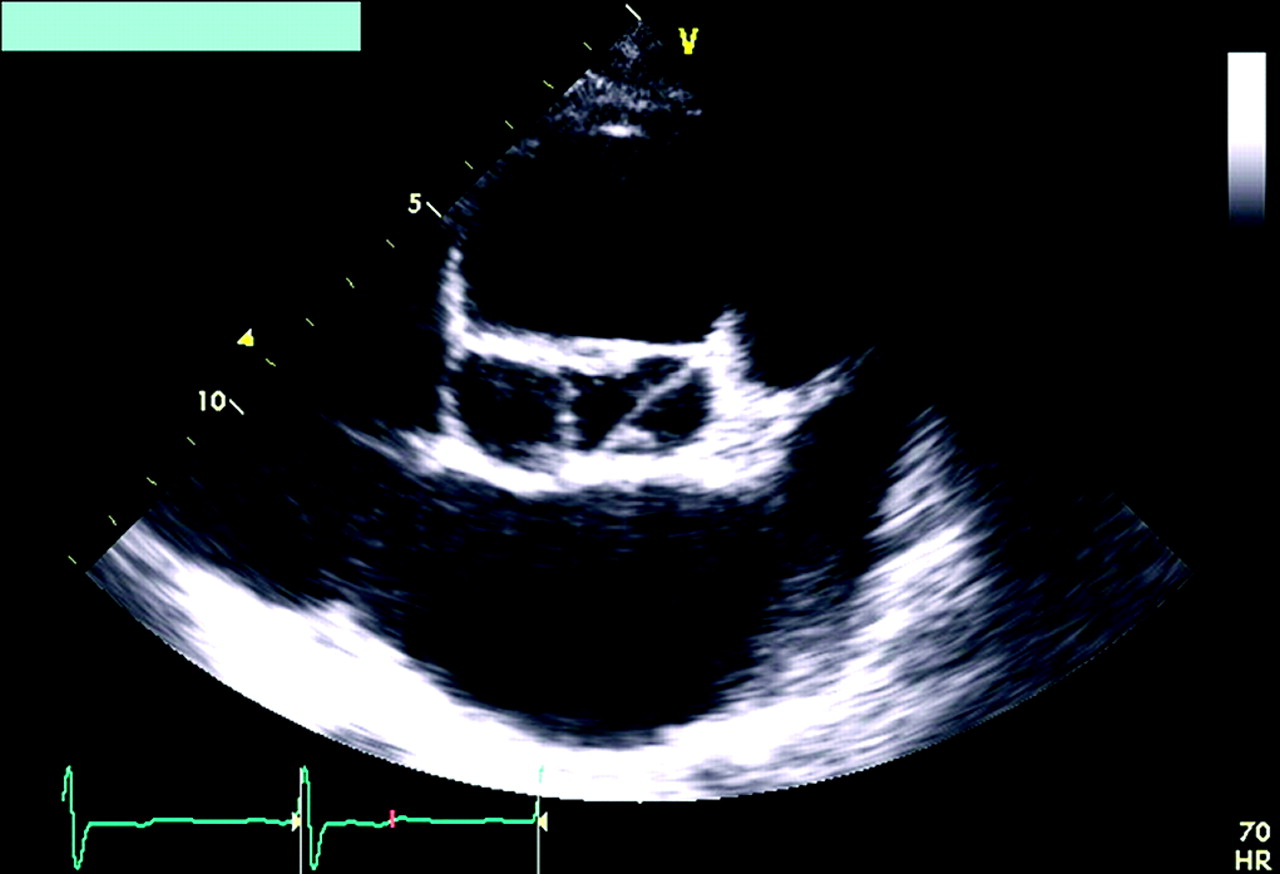
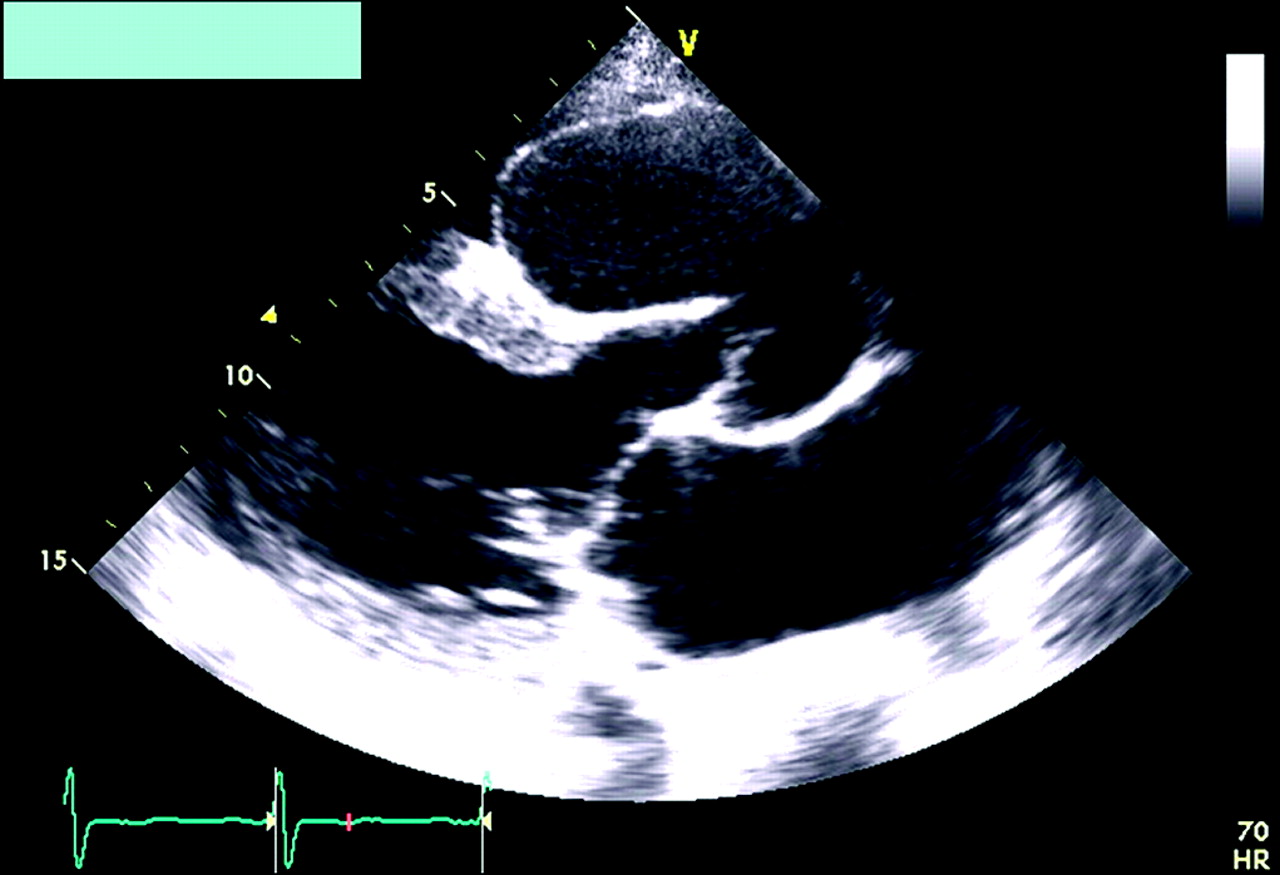
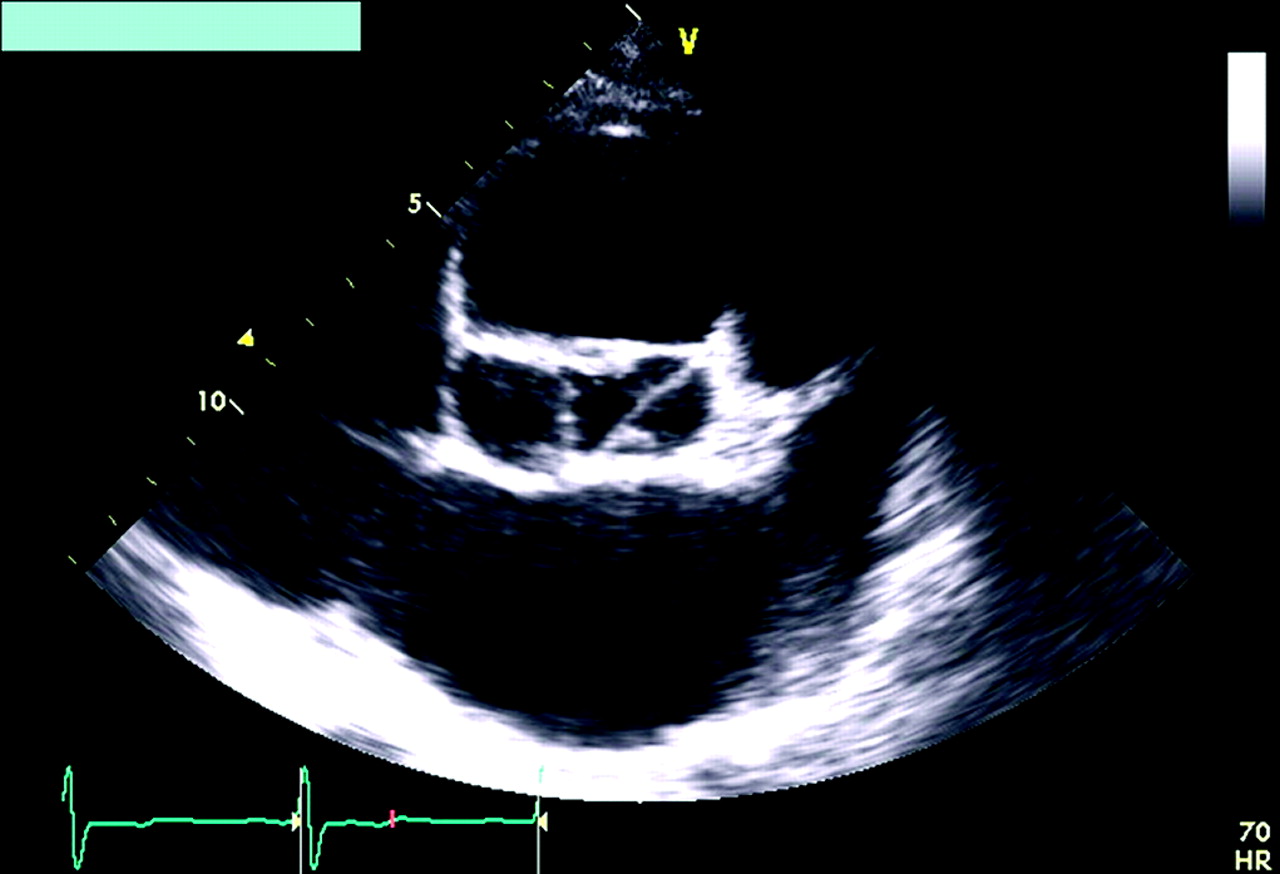
His transthoracic echocardiogram reveals a huge sinus of valsalva aneurysm affecting the right coronary sinus with a dimension of 6.2×5 cm with no fistula or rupture complications(figure 1 2). There was an eccentric moderate to severe aortic regurgitation with a pressure half-time of 286 m/s. Other findings included hypokinesia in the posterior-lateral wall and a mildly dilated impaired left ventricular function.

Parasternal long axis view.
{kind=link}
{kind=link}
Parasternal short axis view at the level of aortic valve
Aneurysm of sinus of valsalva (SVA) is a rare congenital condition with a prevalence of 0.14–0.96% individuals with open heart surgery. It is usually congenital, affecting predominantly the right coronary cusp. Our subject demonstrated multiple complications of sinus of valsalva aneurysm which included heart failure from significant aortic regurgitation,1 obstruction of the right ventricular outflow tract,2 myocardial infarction secondary to coronary artery compromise and thromboembolic phenomena.3 SVA also occurs in ulcerative colitis secondary to Takayashu disease and syphilitic aortitis. With consultation, the decision was for conservative treatment.
Our subject has a late presentation and highlights the importance of echocardiogram for assessing radiological cardiomegaly and abnormal ECGs.
This case also highlights the value of echocardiography as an initial assessment tool in acute coronary syndrome.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.