Article Text

Abstract
Background Cardiac involvement is a recognised complication in female carriers of Duchenne muscular dystrophy (DMD). Since segmental or global left ventricle (LV) wall motion abnormalities in DMD carriers can arise even without apparent muscle weakness, it is difficult to differentiate cardiac involvement of a DMD carrier from other heart diseases in a non-invasive manner. Cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) enables assessment of regional wall motion abnormality and myocardial damage with high spatial resolution.
Objective To assess the utility of CMR for detection of myocardial damage in female carriers of DMD.
Methods and results Gadolinium-enhanced CMR was performed in seven female DMD carriers. Physical examination, electrocardiography, chest radiograph, measurements of total creatinine kinase and brain natriuretic peptide levels, and two-dimensional echocardiography were also performed. Four (57%) of the seven carriers had LGE, and LGE was frequently observed at the subepicardial layer in the inferolateral segment. Two carriers had a focal LGE at the LV inferolateral wall without LV dilation or wall motion abnormalities.
Conclusion CMR findings of DMD carriers were characterised by subepicardial LGE, which was localised at inferolateral segments. CMR may be a useful modality for detecting cardiac involvement in DMD carriers.
- MRI
- gadolinium
- muscular dystrophies
- cardiomyopathies
Statistics from Altmetric.com
Duchene muscular dystrophy (DMD) is an X linked recessive disorder caused by a deficiency of dystrophin in skeletal and cardiac muscles.1 Many patients with DMD have cardiac involvement including dilated cardiomyopathy, and cardiac involvement is the most important determinant of clinical status and long-term outcome in patients with DMD.1 2 Female carriers of DMD also exhibit cardiac involvement such as left ventricle (LV) dilatation, segmental or global wall motion abnormality, and dilated cardiomyopathy.3–5 Myocardial damage in DMD carriers is characterised by myocardial fibrosis and fatty replacement, and the incidence of cardiac involvement in DMD carriers has been shown to increase with age.6 7 However, segmental or global LV wall motion abnormalities in DMD carriers can arise even without apparent muscle weakness, and it is difficult to differentiate cardiac involvement in a DMD carrier from other heart diseases in a non-invasive manner.
Cardiac magnetic resonance (CMR) is a precise and reproducible method to evaluate regional wall motion abnormality of the left ventricle. Furthermore, recent studies have shown that late gadolinum enhancement (LGE) non-invasively enables detection of myocardial fibrosis in cardiomyopathy of both ischaemic origin and non-ischaemic origin with high spatial resolution.8 9 The localisation and pattern of LGE have been shown to be different among various heart diseases.10
Thus, the aim of the present study was to assess the utility of CMR for detecting myocardial damage in DMD carriers.
Methods
Study population
Seven female carriers of DMD (54±6 years old) underwent a comprehensive cardiological work-up including gadolinium-enhanced cardiac magnetic resonance (CMR) to evaluate cardiac involvement. The diagnosis of carrier was made on the basis of detection of mutations in the dystrophin gene, mosaic staining of dystrophin in muscle cells of skeletal muscle biopsy, highly elevated levels of serum creatine kinase (CK) activity, or genetic confirmation of definite carrier based on the pedigree, as reported previously.11 Investigations included a full medical history, routine physical examination, electrocardiography, echocardiography, CMR and measurements of brain natriuretic peptide (BNP) levels. The study was approved by the Ethics Committee of The University of Tokushima Graduate School. Written informed consent for participation in the study was obtained from all carriers.
Echocardiography
All patients underwent complete two-dimensional echocardiography using a 3.5 MHz transducer. LV end-diastolic diameter (LVDd) and end-systolic diameter (LVDs) were measured in the parasternal long-axis view. Biplane LV ejection fraction (LVEF) was calculated using Simpson's rule. The degree of LV dilatation was defined according to reference limits and partition values of left ventricular size published by the American Society of Echocardiography.12 The wall motion abnormality (WMA) of the left ventricle was assessed blindly by using a standard LV 17-segment model.13 Segmental wall motion was visually assessed as normal, hypokinesis, akinesis and dyskinesis.
Cardiac magnetic resonance (CMR)
CMR (GE Signa Excite 1.5 T, Milwaukee, Wisconsin) was performed using a phased-array coil, according to a previously reported method.14 15 In brief, short-axis images as well as two-chamber, three-chamber and four-chamber long-axis views were obtained by cine-MRI using a steady-state free-precision technique (FIESTA). Intravenous gadolinium-DTPA-BMA (Omniscan, Daiichi Sankyo, Tokyo; 0.1 mmol/kg) was given, and contrast-enhanced images were acquired after 10–15 min in identical short-axis planes by using an inversion-recovery gradient echo sequence. Inversion times were adjusted to null normal myocardium (typically 260–320 ms). Fat-saturated and T2-weighted images were also obtained to allow differentiation among subepicardial LGE, epicardial fat and pericardial effusion.
LV function parameters were measured quantitatively using MASS software (Medis, Leiden, The Netherlands). Two blinded observers, who were unaware of the results of the other modality, evaluated cine and contrast images. Wall motion and localisation of gadolinium enhancement were assessed blindly using a standard LV 17-segment model, as described above. The patterns of LGE were classified as subendocardial, midwall, subepicardial and transmural.10
Statistical analysis
All data are expressed as means±SD.
Results
Characteristics of DMD carriers
Muscle weakness was found in five of the seven DMD carriers, and the duration of muscle weakness was 23±6 years. Five DMD carriers complained of exertional dyspnoea, and ECG abnormalities including high R wave (>4 mm), R/S ratio >1 in V1 or V2 and small Q waves in I, aVL, V5–V6 were noted in five DMD carriers (table 1).
Characteristics of Duchenne muscular dystrophy carriers
Echocardiography showed mild LV dilatation in two of the seven DMD carriers and segmental WMA at inferolateral segments without LV dilatation in one carrier. Only one of the seven carriers had global WMA with markedly impaired LVEF and mild elevation of BNP level.
CMR findings of DMD carriers
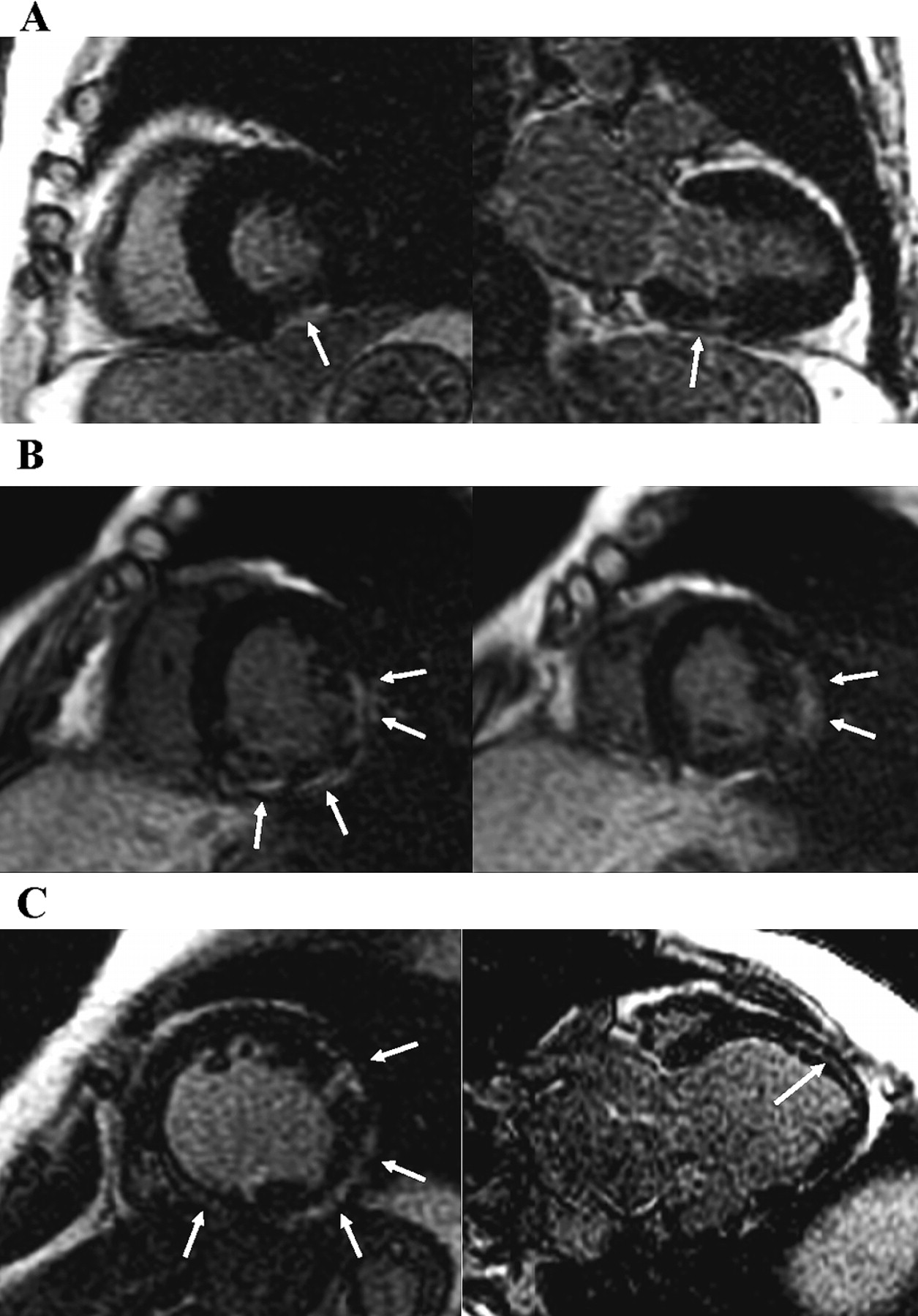
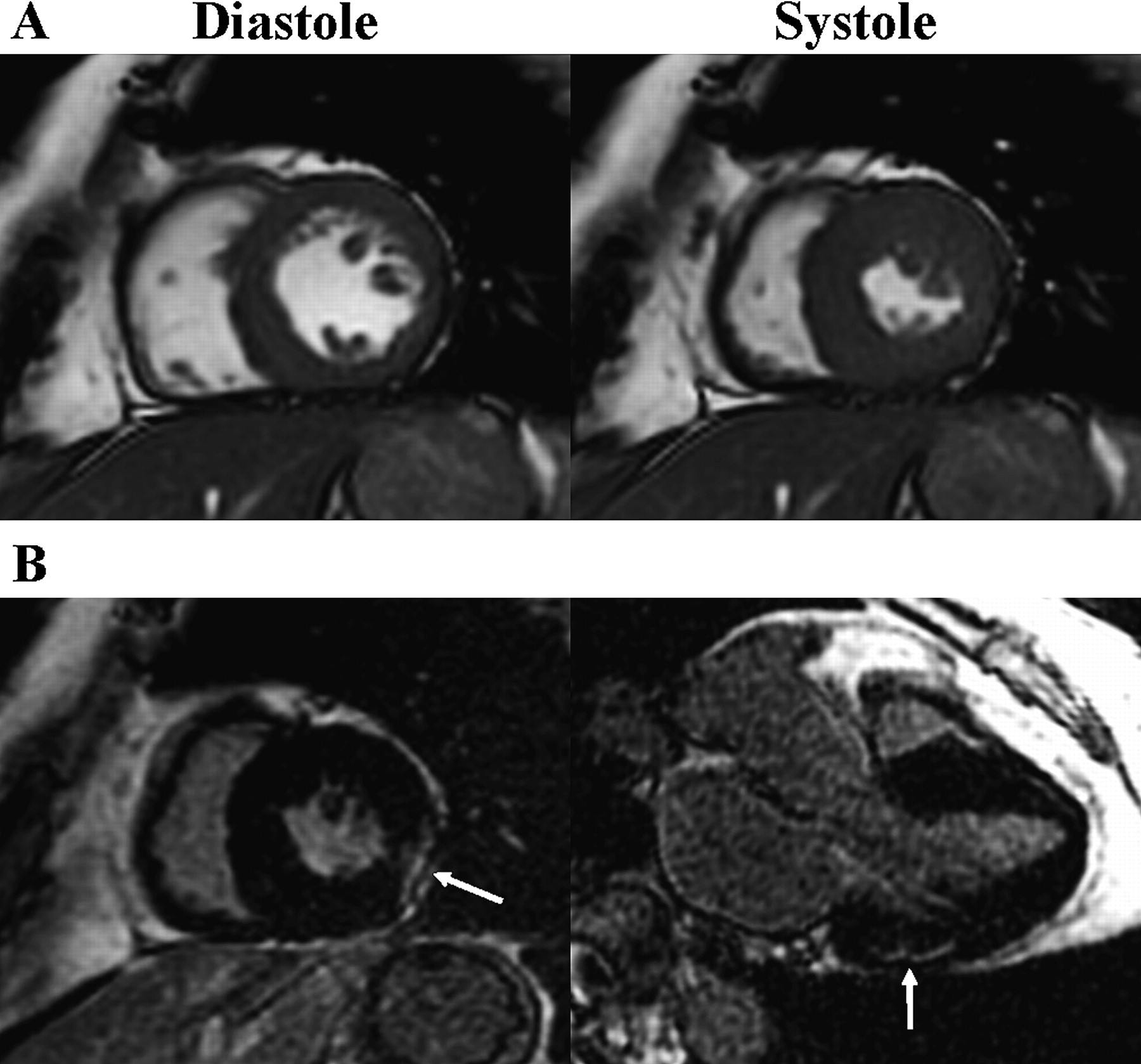
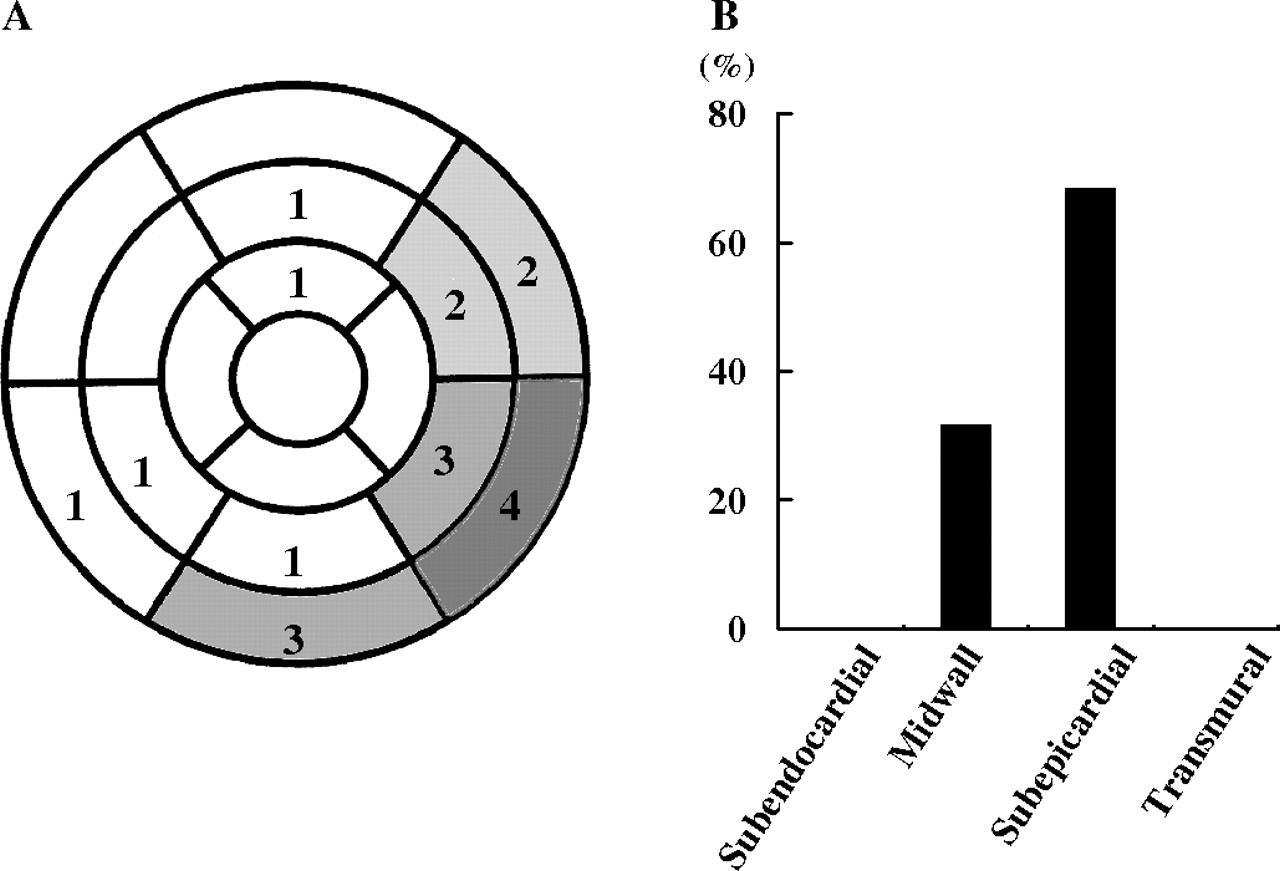
In cardiac magnetic resonance, four of the seven carriers had LGE (figures 1 and 2). LGE was mostly confined to the basal or mid portion of the LV free wall (15 of 19 LGE segments: 79%), particularly the inferolateral segment (figure 3). The most common pattern of LGE was subepicardial followed by midwall. None of the carriers had subendocarrdial or transmural LGE. Despite normal LVEF without WMA and LV dilatation shown by echocardiography, two carriers had focal LGE with a subepicardial pattern (figure 2). One carrier with markedly impaired LVEF had extensive LGE at the LV free wall and interventricular septum. That carrier suffered from severe heart failure and died suddenly 6 months after CMR despite medical treatment.
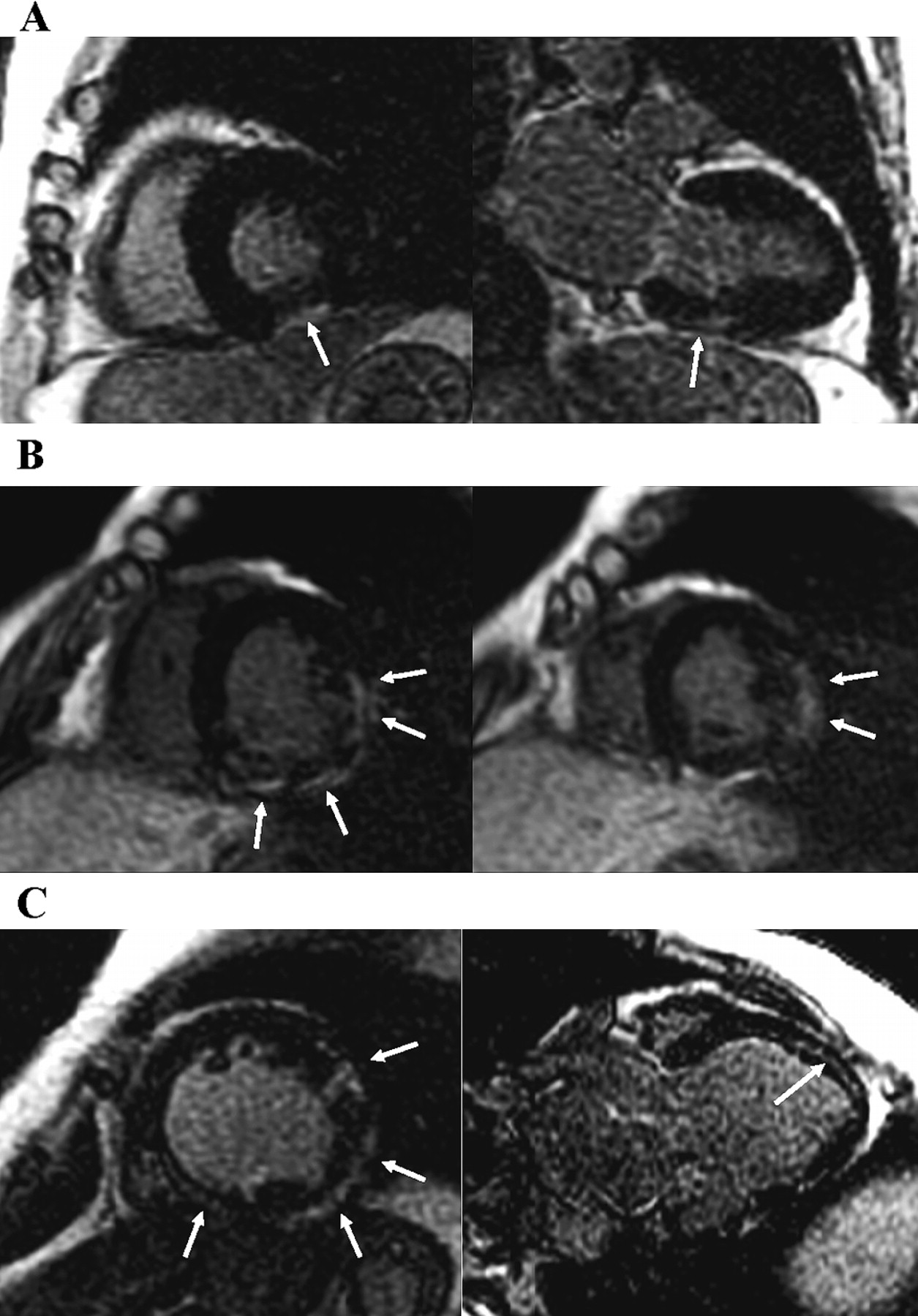
Late gadolinium enhancement (LGE) patterns in Duchenne muscular dystrophy carriers. (A) Focal LGE (white arrows) confined to the subepicardial layer of the basal inferolateral segment (carrier 3). (B) Large area of subepicardial LGE, observed in basal inferolatreral to lateral segments and the midlateral segment (carrier 4). (C) Extensive LGE detected in the midwall layer of the interventricular septum and in the subepicardial layer of the left ventricle free wall (carrier 1).

Cardiac magnetic resonance images of carrier 6. (A) Cine-MRI showing preserved left ventricle contraction without wall motion abnormality (left ventricular ejection fraction: 71%). (B) Small area of late gadolinium enhancement (white arrows) confined to the outer-mid-subepicardial layer of the basal lateral segment.

{kind=link}
{kind=link}
{kind=link}
Distribution and pattern of Late gadolinium enhancement (LGE) in Duchenne muscular dystrophy (DMD) carriers. (A) Distribution of LGE in four DMD carriers using a standard left ventricle 17-segment model. (B) Pattern of LGE.
Discussion
We demonstrated that (1) four of the seven DMD carriers had segmental or global LGE, (2) subepicardial LGE was mainly located in the inferolateral wall, and (3) segmental LGE was observed without LV dilatation and LV systolic dysfunction.
In the present study, most of the LGE was distributed in the subepicardial layer of LV inferorateral walls. On the other hand, one carrier with marked LV systolic dysfunction showed midwall LGE at the interventricular septum as well as subepicardial LGE of LV the free wall. These findings are consistent with results of a previous study showing that myocardial fibrosis begins in the inferolateral portions of the left ventricle, the posterior papillary muscle, and the interventricular septum in DMD carriers.6 McCrohon et al showed that gadolinium-enhanced CMR discerns left ventricular dysfunction-related ischaemic heart disease and dilated cardiomyopathy on the basis of patterns of LGE.9 A subendocardial or transmural pattern is observed in patients with ischaemic heart disease, and LGE at the midwall layer suggests dilated cardiomyopathy. The pattern of LGE in the present study, inferolateral-dominant LGE at the subepicardial layer, was different from the patterns in ischaemic heart disease and dilated cardiomyopathy. These findings suggest that CMR may enable not only non-invasive detection of myocardial damage in DMD carriers but also differentiation of cardiac involvement in DMD carrier from other heart diseases.
Symptoms of cardiac involvement in the carriers are variable, ranging from asymptomatic to severe heart failure, and the impact of cardiac involvement on life expectancy is still under debate.16 However, heart transplantation or implantation of a prophylactic implantable cardioverter/defibrillator was required in some cases.7 17 In the present study, one carrier with extensive LGE in the subepicardial and midwall layers died suddenly, despite medical treatment. Earlier studies have shown that the presence of LGE predicts future cardiovascular events such as cardiovascular hospitalisation and sudden cardiac death in patients with cardiomyopathy of non-ischaemic origin.18 Taking these findings together, it is possible that cardiac magnetic resonance can predict the future cardiovascular events, resulting in better selection of DMD carriers for heart failure treatments.
Previous studies have shown that ECG abnormalities in DMD carriers are characterised by high R waves in right precordial leads, small Q waves in inferolateral leads and bundle branch blocks.4 In the present study, five of the seven DMD carriers had abnormal ECG findings, and four DMD carriers with ECG abnormality were positive for LGE. However, normal ECG findings in DMD carriers with dilated cardiomyopathy have also been reported, suggesting that the sensitivity of ECG for detecting cardiac involvement is still unknown.19 Further study is needed to clarify the relationship between ECG abnormality and LGE for detection of cardiac involvement in DMD carriers.
LV dilatation, segmental wall motion abnormalities and dilated cardiomyopathy are the major findings of cardiac involvement in DMD carriers.4 All DMD carriers are recommended to receive two-dimensional echocardiography periodically for screening of cardiac involvement.20 21 However, in the present study, two carriers had focal LGE at the LV inferolateral wall without LV dilation or wall motion abnormalities, suggesting that myocardial damage in DMD carriers begins before left ventricular morphological changes occur and that CMR is a more sensitive modality for detecting myocardial damage in DMD carriers than conventional two-dimensional echocardiography.
Conclusion
CMR findings of DMD carriers were characterised by subepicardial LGE, which was localised in the inferolateral segments. CMR may be a useful modality for detecting cardiac involvement in DMD carriers.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Ethics Committee of The University of Tokushima Graduate School.
Provenance and peer review Not commissioned; externally peer reviewed.