Article Text

Statistics from Altmetric.com
A 50-year-old female was referred to us for diagnostic and therapeutic inferior vena cava (IVC) gram. She was worked up as a case of secondary Budd–Chiari syndrome with portal hypertension. She had complaints of abdominal distension, decreased appetite and recent-onset rectal bleeding, for which she was subjected to lower GI endoscopy which showed rectal varices. She was diagnosed as a case of Budd–Chiari secondary to IVC obstruction. The patient was worked up for portal hypertension aetiology. Basic investigations were done: Hb was 8 gm%, TLC 7000/mm3, platelet count 160 000/mm3, PT 17 (control –14) and PTT 48 (control –35). BT and CT were normal. Since the patient was planned for percutaneous intervention so it was decided to transfuse her two units of whole blood.
Method
Right femoral artery access was taken by puncturing the same by the Seldinger technique followed by insertion of 8 Fr sheath and 5000 units of conventional heparin was given. A pigtail catheter 6Fr was taken through it and parked in IVC, and a venogram was taken. There was total obstruction of IVC with filling of a collateral channel seen. The IVC membrane was ruptured with the stiffer end of 0.038 guidewire followed by predilatation of the stenosed segment with (OTW, Advance Balloon 8×100) balloon at 6 atm pressure for 10 s. Subsequently a CP stent (14×80 mm, balloon-mounted stent) was deployed at 5 atm for 6 s. A final check shoot revealed patent IVC with good results.

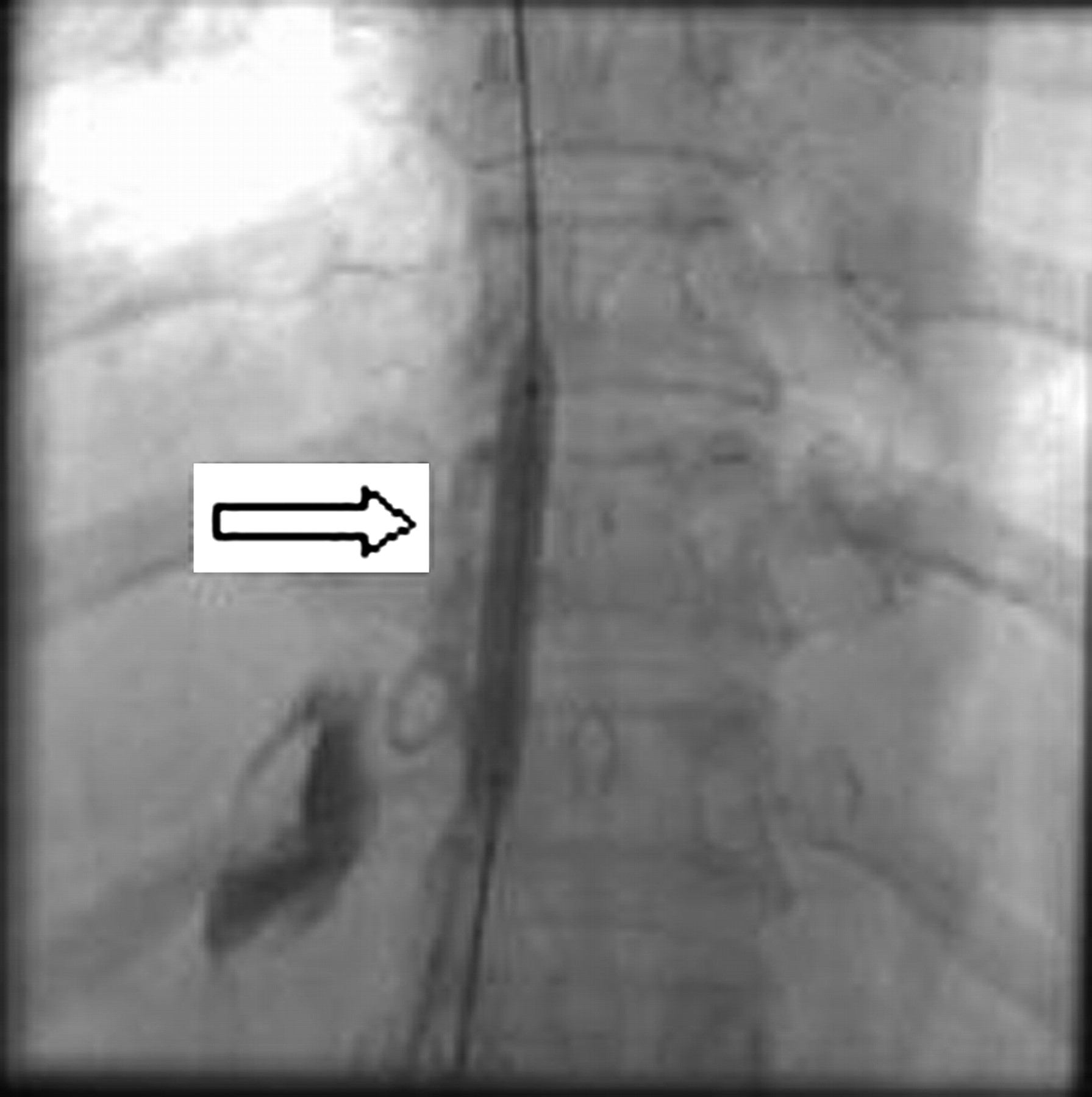
IVC gram showing abrupt interruption of the intrahepatic portion of IVC.
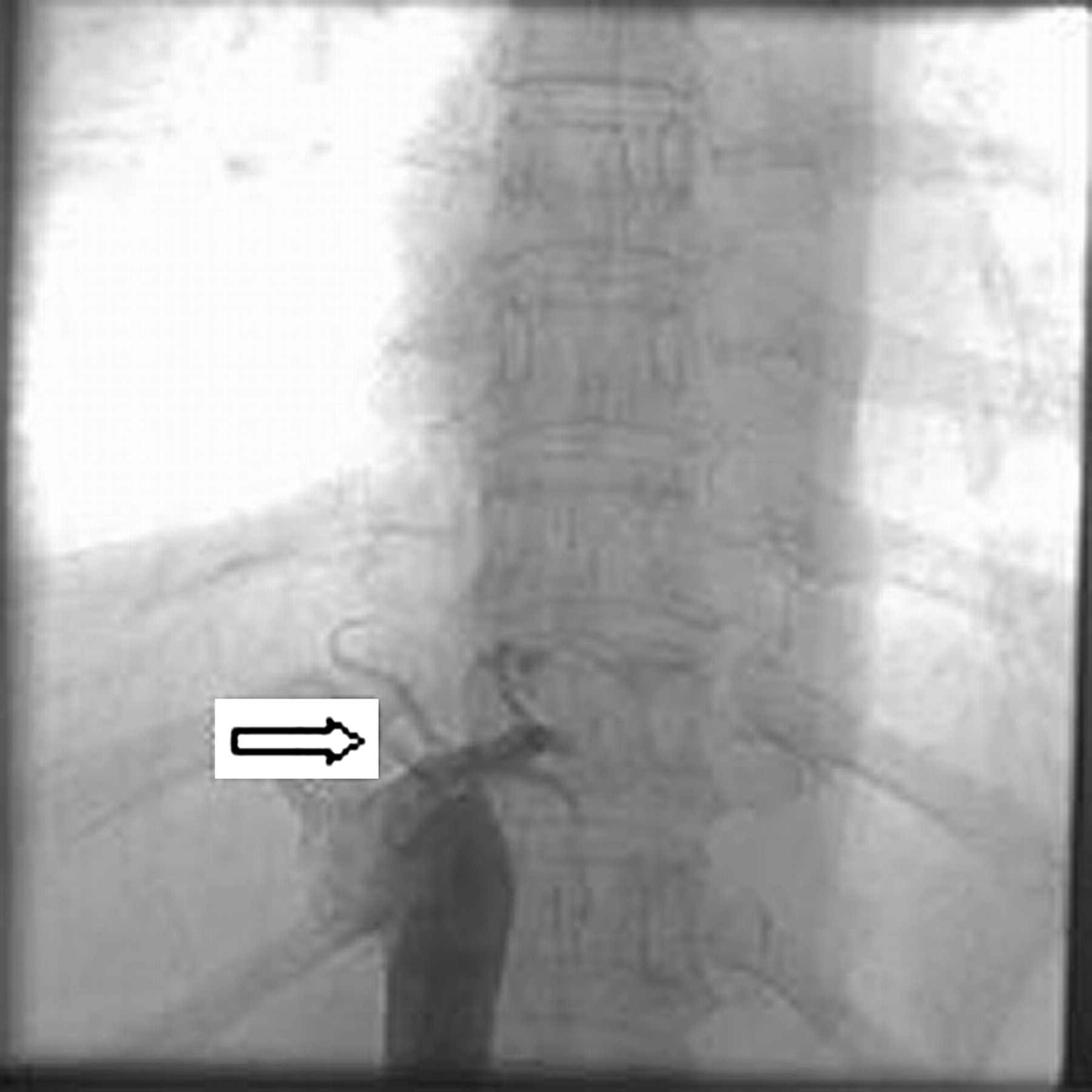
Balloon dilatation of the membrane over the 0.035 guidewire used for perforation of the membrane.
{kind=link}
{kind=link}
{kind=link}
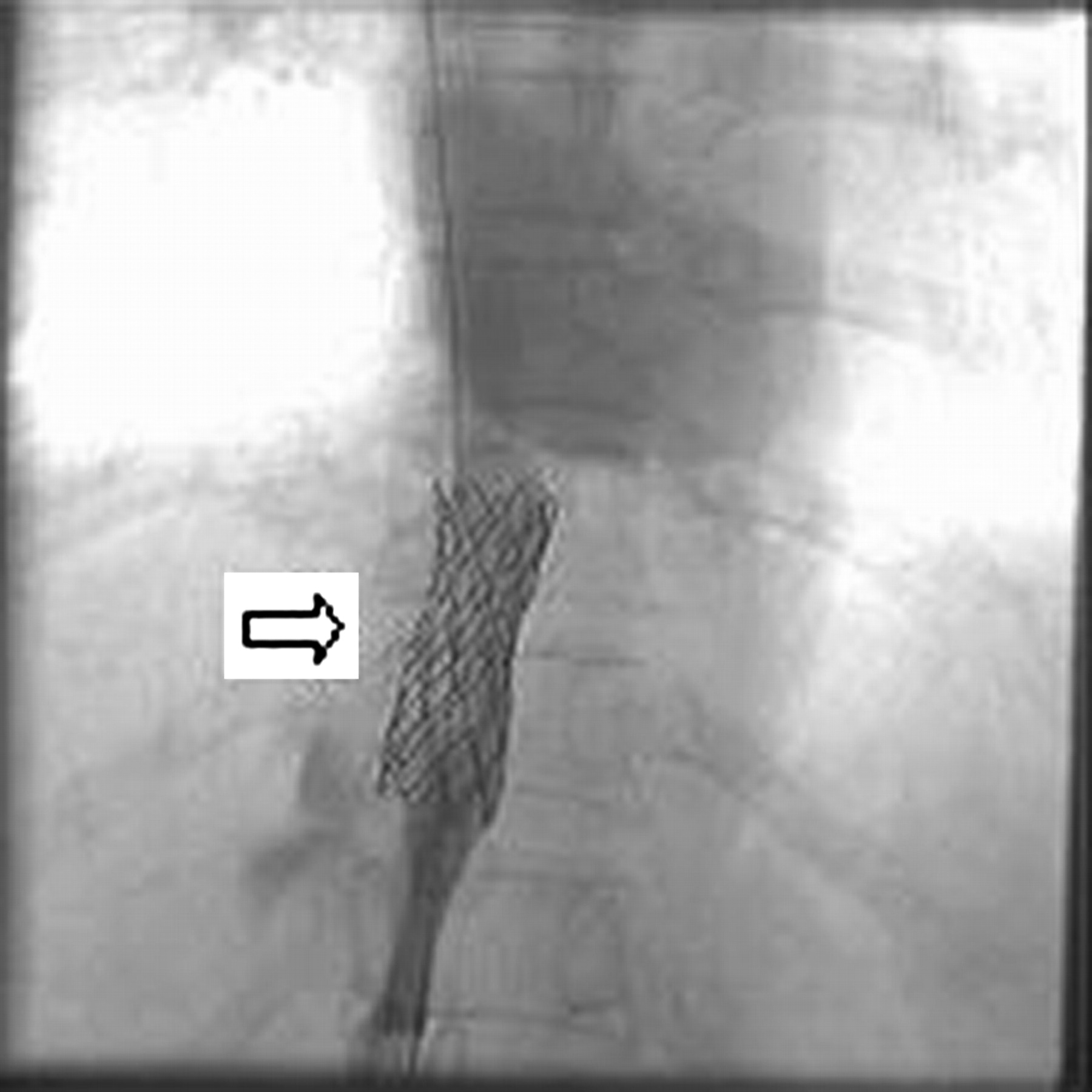
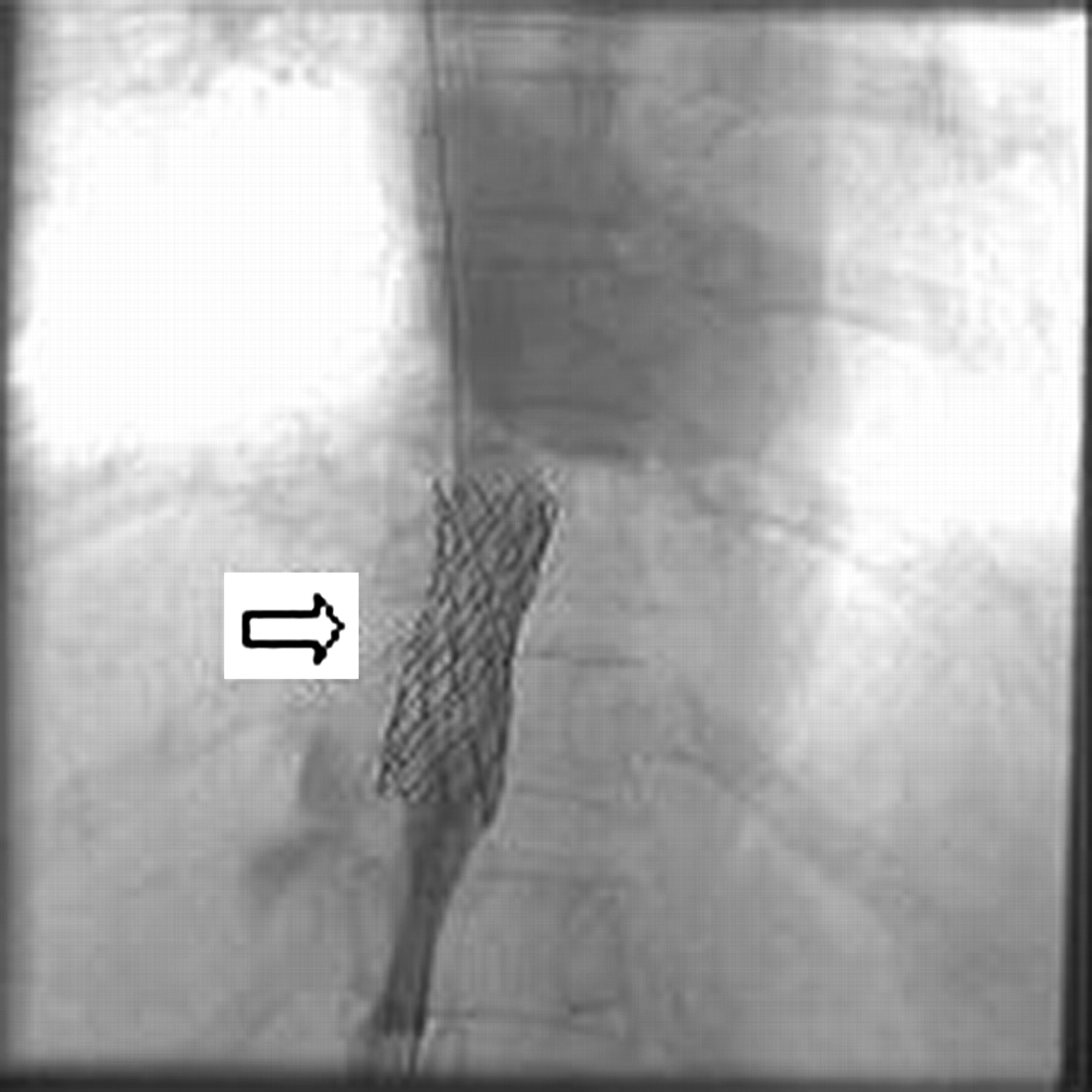
Stented segment of the IVC membrane with normal flow towards the right atrium.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.