Article Text

Statistics from Altmetric.com
- Plasmaphaeresis
- multivessel myocardial infarction
- post partum vasculitis
- proposed anti-inflammatory therapy for myocardial infarction
- acute coronary syndrome
- inflammation
- pregnancy
- therapeutics
Introduction
During the last 50 years, the treatment of myocardial infarction has evolved. Monitoring of arrhythmias,1 defibrillation of the detected arrhythmias and the eventual implantation of defibrillators have decreased the risk of sudden death.2 Anticoagulation, antiplatelets and thrombolytics attacked the initiating event of thrombosis within the artery.3–8 This event, easily accepted today, required visualisation of the thrombus in live patients, since the clot was often absent in pathological examination.9–12 A great deal of effort has been spent in refining antithrombotic drugs and the development of protocols that would reduce thrombosis with the least risk of bleeding. The observation of clot in a vessel enabled cardiology to decrease the mortality of myocardial infarction from 50% to less than 5%. Although many agents have been added to the patient to reduce thrombosis, there has never been a consideration to remove offending agents from the patient.
A new paradigm in the aetiology of myocardial infarction has been growing in our clinical trials. This new concept is the role of inflammation.13–15 Inflammation of blood vessels is one explanation for the onset of the clinical syndrome. Coronary atherosclerosis is present in 75% of individuals over the age of 21. This fact has been known since the Korean War.16 17 Inflammation weakens the lipid-filled plaque wall. The thinned plaque ruptures, exposing the blood vessel to thrombogenic factors, and attracts clumping platelets to initiate clots. Inflammation occurs in a smaller percentage of individuals explaining why acute events are less frequent than the prevalence of disease.18 Inflammation can be helpful by signalling for repair progenitors, but may also impede the healing of the myocardium by destroying the progenitor cells or disrupting differentiation that would replace the damaged myocardium. Inflammation of the vessel wall is more difficult to visualise than clots, but appears to the initiating culprit prior to a thrombosis. Recent studies demonstrate that attacking inflammation can be a preventive strategy.19 Many of our therapies that have been shown to decrease mortality after myocardial infarction also have anti-inflammatory properties.
An unusual case of inflamed coronary blood vessel may point to a new approach in the treatment of myocardial infarction. The case, still considered an unknown clinical event, is thought to represent a primary inflammation of the coronary arteries. A recent pregnancy in the case is thought to be the aetiology of the inflammation that somehow targeted the heart vessels as a foreign invader. It has similar findings to acute myocardial infarction with chest pain, EKG findings of acute myocardial infarction, ischaemic ventricular fibrillation cardiac arrest, enzyme rise and wall motion abnormalities. It is different from acute myocardial infarction in that it involved all three coronary distributions. This case will be used to illustrate successful removal of inflammatory cytokines and coagulants. Additional anti-inflammatory therapies will be presented that may prepare the infracted heart for recovery.
Inflammatory myocardial infarction
The patient is a 31-year-old female approximately 12 weeks postpartum. She presented to her primary care physician with the complaint of chest discomfort, radiation to the left shoulder which occurred while eating. The rest of the day she had recurrence with eating, but the next day she had discomfort not associated with eating and not relieved with antiacid. These events prompted a visit to the emergency room. Past medical history was remarkable for G2 P2 by C-section 12 weeks prior, previous obesity status post gastric bypass surgery with a 45 kg weight loss and pregnancy-induced hypertension. Her medications consisted of Propanolol LA 80 mg daily, Ibuprofen 800 mg twice daily, Ortho Tri-Cyclen and a multivitamin. She had no known drug allergies and no significant family history. The physical examination (postventricular fibrillation arrest) was normal with the exception of S4.
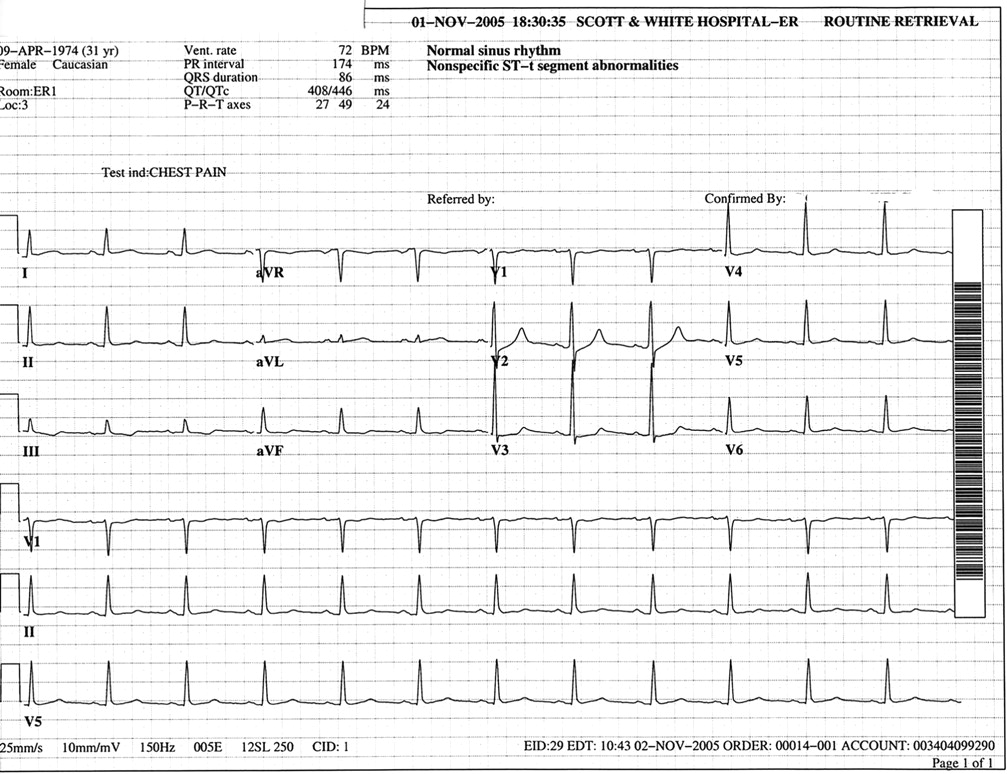
In the Emergency Room, the patient initially was triaged to non-cardiac chest pain and was in the process of being given 0.5 mg of Dilaudid when the monitor displayed ventricular fibrillation (figure 1). Post defibrillation, her pain resolved, and she spontaneously converted to sinus rhythm with normalised ST segments (figures 2, 3). Echocardiogram at the bedside demonstrated posterior-lateral hypokinesis with left ventricular hypertrophy. The assessment at that time was ischaemic ventricular fibrillation. The aetiology of the ischaemia could be secondary to ruptured atherosclerotic plaque or coronary artery spasm. The patient was then treated with intravenous lidocaine, heparin, IIb IIIa inhibitors and intravenous nitroglycerine. She remained pain-free overnight on this therapy and went to cardiac catheterisation the next day.

R on T ventricular fibrillation.

Postventricular fibrillation conversion to atrial fibrillation.

Spontaneous conversion from atrial fibrillation to normal sinus rhythm.
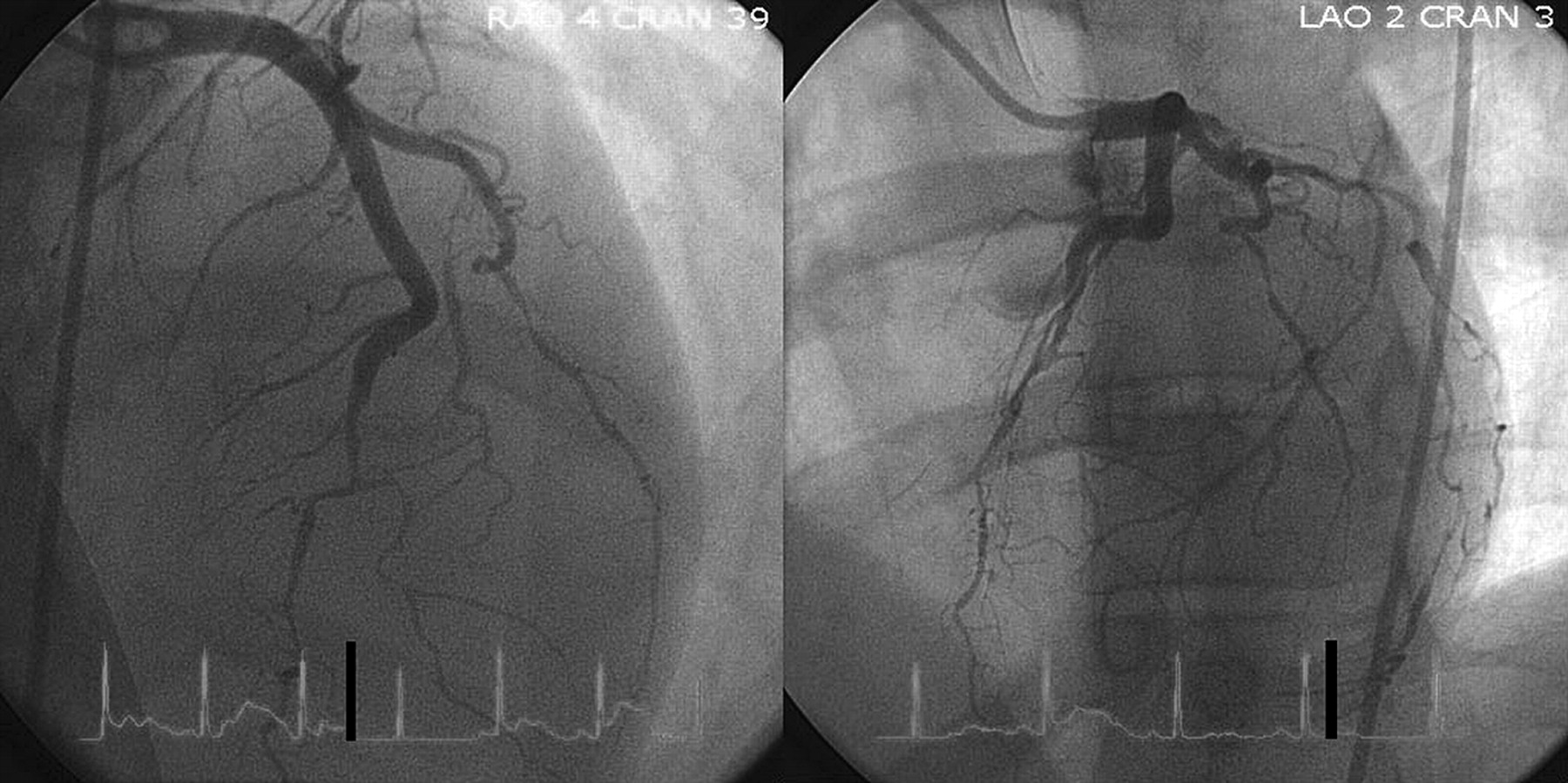
Coronary angiography was performed on intravenous nitroglycerine and is best described as severe pruning of her coronary tree in all three distributions with TIMI flow being worse in the circumflex distribution (figures 4, 5). The appearance was consistent with transplant vasculopathy. No intervention was possible, and the patient was assigned medical therapy. She promptly demonstrated acute injury pattern during the anticoagulation-free period of sheath removal.
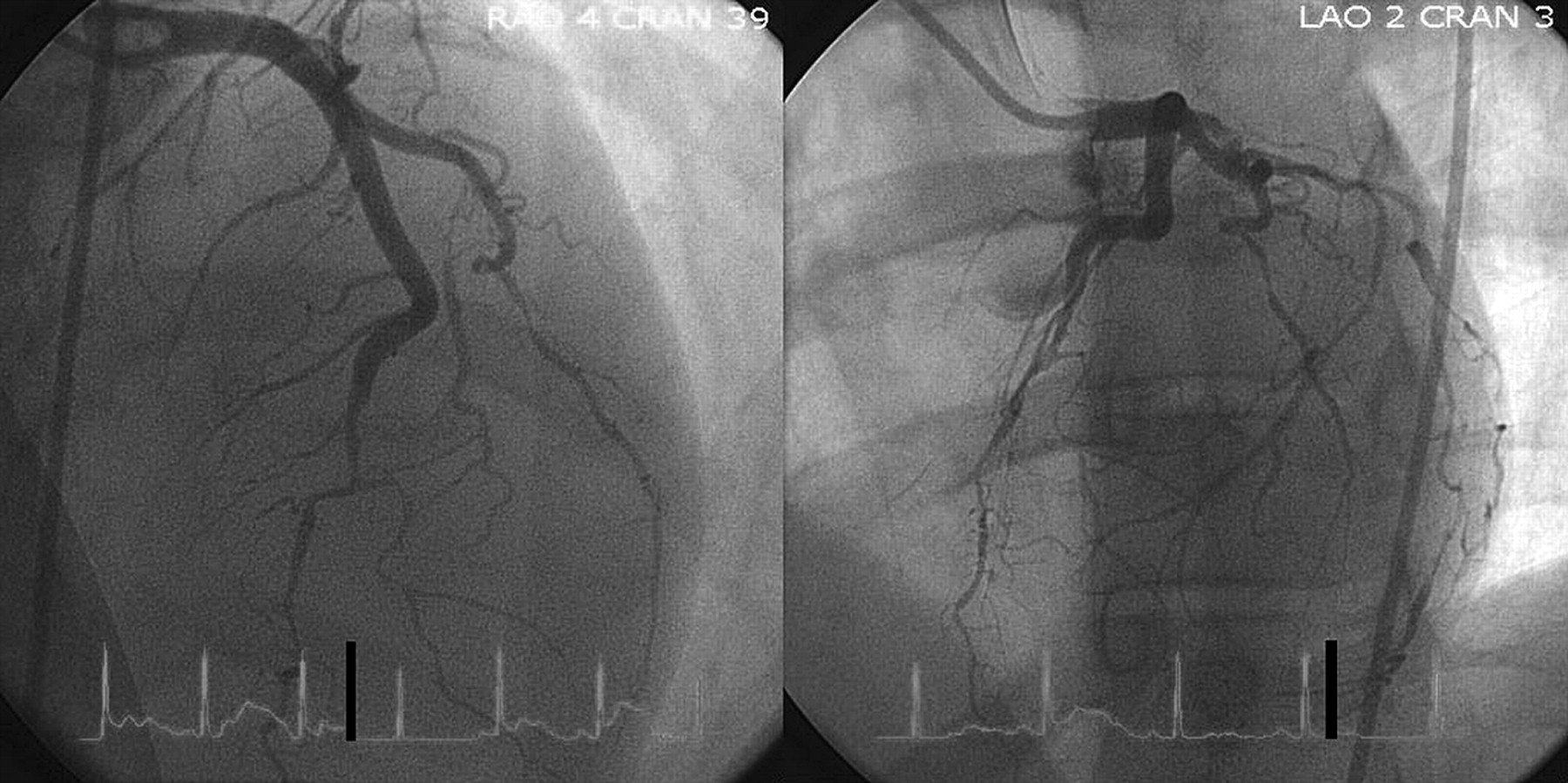
Left coronary artery two views.

Right coronary artery.
The differential diagnosis includes typical coronary disease, but this is unlikely due to the acute onset with an angiogram demonstrating diffuse native disease in an individual who had recently carried a full-term pregnancy. Some form of coronary vasculitis seemed more plausible, but associated symptoms were lacking. The only other vascular distribution that may have been clinically implicated was the mesenteric vessels manifested by pain with eating. The differential as listed by Waller et al includes tuberculosis, polyarteritis nodosa, giant cell arteritis, rheumatic fever, systemic lupus erythematosus, thrombo-angitis obliterans, Wegner granulomatosis, salmonella, leprosy, Kawasaki disease, Takayasu disease, typhus, infective endocarditis, rheumatoid arthritis, ankylosing spondylitis and syphilis.20 The patient had no other associated finding, and 4 years of follow-up has not revealed any diagnosis listed.
In a flurry of calls to transplant centres, there were rumoured cases of postpartum severe coronary disease that may have been similar to transplant coronary vasculitis. The literature review for documentation of these cases was however empty. It was felt that pregnancy and fetal cells stimulated the immune system to react in an adverse manner. A similar process occurs in transplant vasculopathy where the vessels are foreign and attacked by the immune system. Plasmaphaeresis has been reported to be beneficial in treatment of transplant vasculopathy which the angiogram most resembled. This reasoning prompted the additional therapies of immune suppression and plasmaphaeresis.
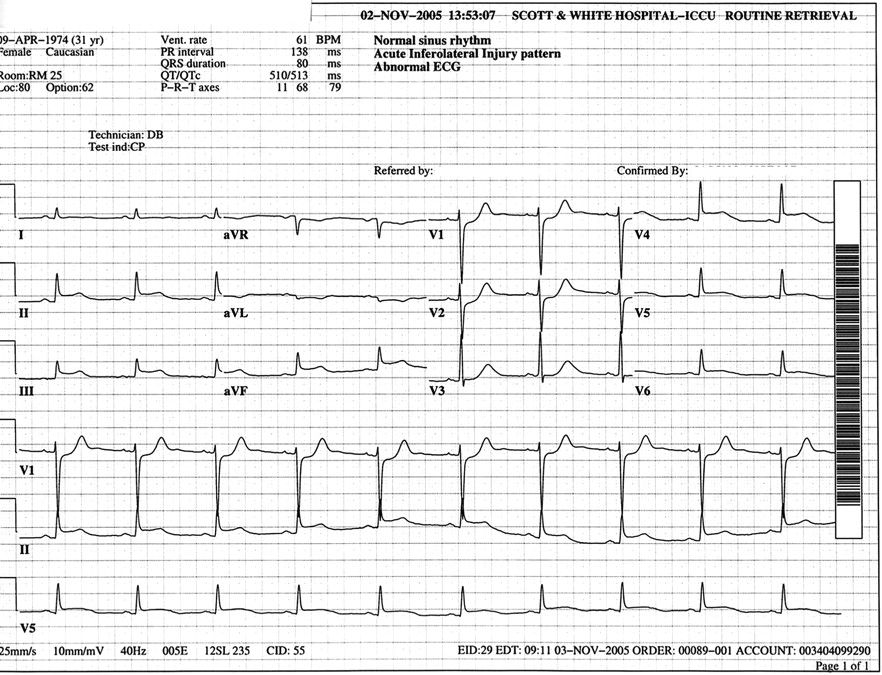
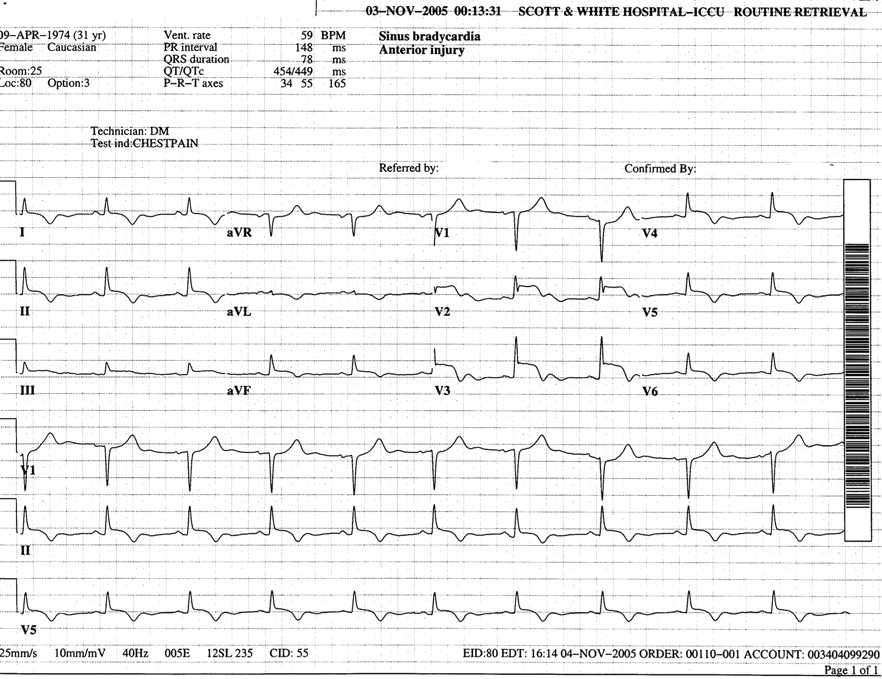
The hospital course over the next several days continued to demonstrate EKG changes and recurrent pain with infarct pattern in all three distributions (figures 6–9) and troponin rise (figure 10). The dips in the troponin graph represent the affect of plasmaphaeresis. Echocardiograms demonstrated a decline in left ventricular function. She was treated with standard therapy for myocardial infarction: aspirin, clopidigrel, warfarin, proton-pump inhibitor, β blockers, ACEI, Spironolactone, Amiodarone and an internal defibrillator. Additional non-standard therapy was initiated on the day of her catheterisation, day 2.

Posterior lateral injury.
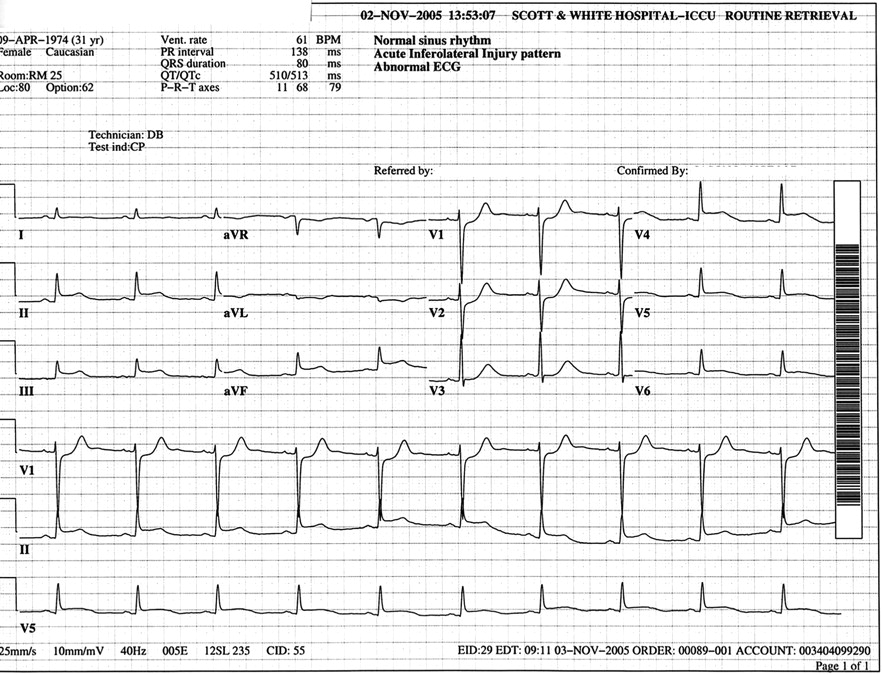
Inferior lateral injury.

Anterior and inferior injury.
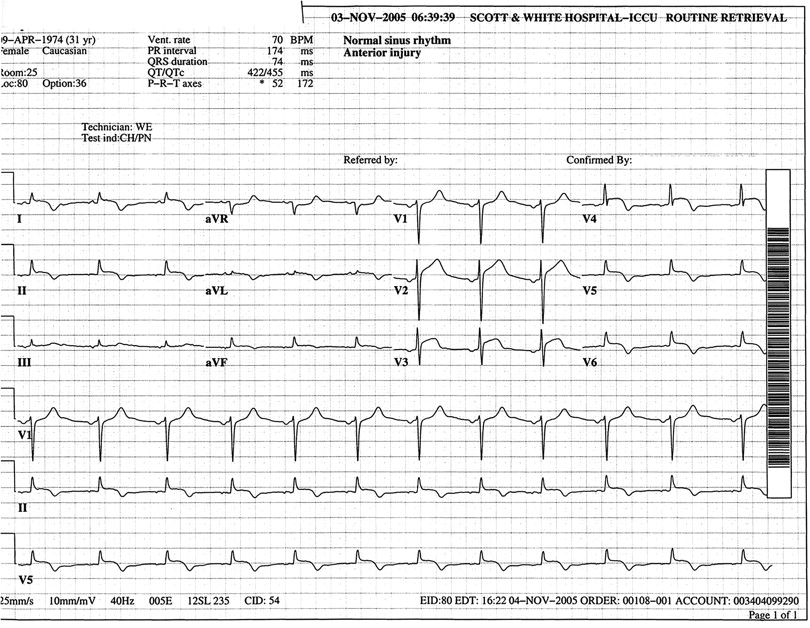
Anterior injury.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph of troponin.
Since vasculitis was the working diagnosis, plasmaphaeresis was initiated: days 2, 3, 4, 7, out patient for 3 weeks, intravenous immunoglobulin between plasmaphaeresis 3 and 4, and steroids. Her steroids were tapered after being boosted during one readmission for recurrent pain and minor injury, and plasmaphaeresis completed. She remained on warfarin for apical aneurysm for 3 months. Six months after her admission, a CT angiogram was performed that demonstrated healing of her vasculitis. Plavix was discontinued at this time. Her left ventricular function was normal. She remained on aspirin, β blocker, ACE inhibitor and statin. She has remained well without heart failure or angina for the last 4 years. No other collagen vascular or vasculitic symptoms have occurred.
Review of anti-inflammatory therapies
Inflammation and immunity is a fundamental law of biology. Self needs to be protected from the environment. It is a complex process that has evolved multiple pathways with multiple checks and balances. Regeneration and replacement of senescent cells utilises this system to process the dying cells. Inflammation utilises cellular components (endothelium, T cells, B cells, dendritic cells, leucocytes, eosinophils, basophils, monocytes, macrophages, mast cells, plasma cells and platelets), humeral elements (immunoglobulin IgG, IgM, IgA, IgE, natural antibodies and immune antibodies) and signalling proteins (compliment cascade, tumour necrosis factor, intercellular adhesion molecule, monocyte chemoattractant protein, bradykinin, histamine, interleukin, platelet-activating factor, prostaglandins, leucotrienes, selectins (L, E, P) and other ctyokines. Reactive oxygen species produced through inflammatory pathways are deadly molecules that can cause direct injury.21 The inflammatory pathways are more complicated than the coagulation pathways and have proven to be far more difficult to target in therapeutics. Inflammatory and coagulation pathways are intertwined with inflammation, resulting in thrombosis and anticoagulation reducing inflammation. Trials targeting a single pathway such as anti-CD 18 to target the complement cascade have demonstrated promise in animal experiments but have fallen short in humans.22 Many of the pathways have self regulation, so disturbing one pathway may enhance other pathways. The inflammatory pathways are also instrumental in repair and regeneration. Senescent cells are labelled by natural autoantibodies and reprocessed by macrophages. Disruption of one pathway may have deleterious effects when other pathways compensate for the disruption. The review that follows is certainly not inclusive of all mechanisms involved in treatment of myocardial infarction inflammation but reflects the rationale in this case. This case illustrates that multiple attacks on the inflammatory system including the cytokines, cellular and humeral pathways may be necessary to achieve success. It would suggest that removal of cytokines and procoagulants is a safe and effective window to new therapies of myocardial infarction.
Plasmaphaeresis
Therapeutic plasmaphaeresis results in the non-selective removal of proteins and other soluble constituents from the plasma portion of whole blood. The relative reduction of any given plasma fraction after a one-volume plasma exchange with albumin as replacement is a function of the relative distribution of that fraction between the intravascular and extravascular compartment, the rate of equilibration between the compartments and the rate of synthesis of the constituent after removal. As an example, for a large protein such as fibrinogen located primarily in the intravascular space, approximately 60% will be removed after a one-volume exchange. The percentage decrease for smaller proteins such as clotting factors ranges from 25% to 50%. Any constituent in the plasma fraction will be at least transiently reduced. In this case, Hs-CRP was reduced to zero with the first exchange.
For approximately four decades, the principle of non-selective removal of odious plasma proteins and substances by therapeutic plasmaphaeresis has been utilised to treat a variety of conditions.23–25 Examples include removal of the IgG plasma fraction to treat such diseases as Goodpastures syndrome, myasthyenia gravis and Guillain–Barré. Removal of the IgM plasma fraction treats cold agglutinin disease and cryoglobulinemia. Removal of the lipid fraction treats primary hypercholesterolaemia. Finally, removal of an aberrant phytanic acid metabolite treats Refsum disease. It is now increasingly recognised that therapeutic plasmaphaeresis also has an effect on immunomodulation and affects the rheological properties of blood by making it less viscous.26 In the cardiac transplant study, nine patients with 3–7-year survival periods after heart transplantations underwent plasmaphaeresis twice a year with 2100–2700 ml of plasma removed. In this group with transplant vasculopathy, there was a significant improvement in the coronary perfusion of the myocardium by radionuclide scintigraphy of the myocardium and coronary angiography.27
Plasmaphaeresis can be performed through central access of the femoral or jugular vein or even the antecubital vein. Preload sensitive patients may be managed by albumin infusion during the initiation of plasmaphaeresis. During plasma exchange, the extracorporeal volume of most circuits is approximately 200 ml of whole blood.
Plasmaphaeresis, in this case, is unique in the treatment of myocardial infarction. Instead of adding things to the patient to prevent further thrombosis, inflammation and clotting factors are removed. It is the fastest method of reducing inflammation and a shotgun approach in that multiple constituents in the inflammatory pathway can be removed. Plasmaphaeresis may reboot the immune system when it has gone astray.
Intravenous immunoglobulin
The source of intravenous immunoglobulin comes from as many as 10 000 blood donors. The half life of an administration of immunoglobulin is 3 weeks. It is used as replacement therapy in immunodeficient states and is used in autoimmune conditions such as myasthenia gravis, idiopathic thrombocytopaenia purpura, Guillian-Barre, Kawasaki coronary vasculitis and transplant rejection.28 The mechanism of action in these autoimmune conditions is not well understood, and the actions are multiple. Immunoglobulins act on B cells and can control their proliferation, production of antibodies and cytokines. Immunoglobulins can act directly on autoantibodies and disrupt feedback loops and prevent activation of T cells. These interactions can halt or delay apoptosis, and neutralise inflammation. Removing autoantibodies to myocardial cells that had been targeted for destruction may allow these cells to recover.
Steroids
Corticosteroids, since 1976, have been considered deleterious in the treatment of acute myocardial infarction.29 30 Initial animal experiments in dogs demonstrated infarct reduction.31 The controversy is certainly not resolved and is fuelled by animal models not reflecting the human condition, the studies performed in non-reperfused arteries and not having the ability to measure infarct recovery over an extended length of time. Corticosteroids have multiple actions and are responsible for white cell infiltration, and inhibit formation of thromboxane, prostaglandins, and leucotrienes.32 They are a dominate factor in inflammation. Steroids can cause apoptosis of haematopoietic cells and protect other glandular cells.33 Glucocorticoids have a direct activation of endothelial nitric oxide synthase.34 Steroids likely have a role in myocardial recovery. Trials with steroids usually have low numbers; however, meta-analysis of these trials is favourable.35 Preventive data exist in the population of COPD patients who take inhaled and oral steroids. These individuals appeared to be protected.36 Trials performed in the reperfusion era need to be separated from those performed prior to reperfusion to determine if the adverse healing in myocardial infarction may be offset by increased regeneration.
Antiplatelets: aspirin, clopidigril, intravenous IIb IIIa inhibitors
These agents have been accepted into the treatment of acute coronary syndromes because of their antithrombotic properties. The first of these drugs, aspirin, was invented by Felix Hoffman in 1897 to relieve his father's arthritis pain. The anti-inflammatory mechanisms of these drugs are complex. They include antiplatelet effects, which modify the reaction of leucocytes, monocytes and endothelium. Inflammatory mediators such as P-selectin, CD40L, NF-kB, CRP, platelet-activating factor, platelet factor 4, thrombospondin and platelet-derived growth factor are produced by platelets and have a profound affect upon inflammation.37 Both aspirin and Clopidigril38 39 have had clinical benefits when administered to high-risk patients who have been stratified by inflammatory markers such as HS-CRP. Bare metal stents require dual platelet therapy for at least 1 month to lessen the thrombogenic potential until normal endothelium covers the metal struts. However, these patients still derive benefit from this therapy a year later, far longer than their risk of thrombosis from the stent. Therefore, the platelet is targeted as a therapeutic goal for both antithrombosis and anti-inflammation.
Heparin
Heparin has long been established as an antithrombotic and has been used in myocardial infarction and acute coronary syndromes for over 50 years. It also has anti-inflammatory properties by blocking adhesion receptors of P-selectin and L-selectin.40 By accomplishing this task, leucocyte movement into tissues is blocked with a reduction in inflammation.
Wafarin
The anticoagulant warfarin acts on vitamin k to reduce coagulation factors. It has been shown in rat inflammation models that warfarin decreased inflammation. One mechanism is inhibition of signal transduction.41 Another method demonstrated that the by-products of coagulation such as the d-dimer were proinflammatory. In a study of patients with atrial fibrillation, they were able to show a reduction in d-dimer and subsequent reduction in CRP and IL-6.42
ACE-inhibitors, angiotensin receptor blockers and β blockers
By inhibiting the effects of angiotensin II, ACE-inhibitors and angiotensin receptor blockers mediate inflammation. Angiotensin II is proinflammatory and exerts those effects through an NF-kB dependent pathway. During drug therapy, Hs-CRP, IL-6 and TNF-α have been shown to be reduced. Both β blockers and ACE-inhibitors exert effects through prostaglandin-dependent vasodilation and have anti-inflammatory affects through this pathway.43
Statins
The JUPITER trial has reinforced the importance of reducing inflammation to prevent primary events.19 Statins were developed to lower cholesterol but their interaction with the endothelium has given them pleotrophic properties which include a reduction in inflammation, improvement in endothelial function and an improvement in repair by increasing circulating progenitor cells. The benefits of statin have been seen in reducing operative risk, survival of systemic inflammation from sepsis, bone fracture, and have a very early affect on reducing morbidity from myocardial infarction and angioplasty.43–46 The mechanism of anti-inflammation includes a reduction of adherence molecules, and thus the recruitment of mononuclear cells into the vessel walls. Cytokines and proteins involved in inflammation are also reduced, and these include the COX-2.
Hypothermia
Hypothermia was not utilised in this case but is included as an inflammatory therapy. Cooling the body after ventricular fibrillation cardiac arrest has survival benefit, improved central nervous system function and improved cardiac function. Cooling the body slows chemical reaction and in particular slows the inflammatory response associated with apoptosis.47
Exercise/cardiac rehabilitation
Exercise continues to be underutilised despite multiple studies proving good outcomes. Heberden in 1772 first described the exercise of sawing wood as a benefit in the control of angina, which he also described. Exercise lowers Hs-CRP, increases circulating stem cells, improves endothelial function and has additional benefits in improving lipid profile, blood pressure, diabetes and obesity. There is no population that has not demonstrated benefit from exercise. The improvement in all of these areas is difficult to determine, since the benefits cross many risk factors. The probable common pathway is the increase in progenitor cells that will affect the other risk factors.
Conclusion
The lack of a textbook diagnosis in the presented case allows speculation as to the aetiology and the response to therapy. The patient's given diagnosis was coronary vasculitis secondary to immunological sensitisation during the pregnancy. The only clinical identified manifestation of vasculitis was found in the coronary tree. The mesenteric vessels were also possibly involved due to the symptoms of abdominal angina. Coronary spasm was an early consideration in this patient. She did not respond to nitrate therapy, and her clinical course was not consistent with coronary spasm. Using the presumed diagnosis of an immunological reaction to the coronary vessels, multiple therapies for vasculitis were initiated. The clinical response included improvement in the electrocardiogram, echocardiogram and coronaries demonstrated by 6-month imaging of the coronary arteries by CT angiography. Acute myocardial infarction has many of the same features with both isolated and multiple localised areas of inflammation that eventually leads to an acute event.48 49 After the infarction, the necrotic myocardium also becomes inflammatory and impedes healing. New therapies that attempt to regenerate the heart with progenitor cells will need to deal with those barriers to healing. Plasmaphaeresis, in this case, is unique in the treatment of myocardial infarction. Instead of adding things to the patient to prevent further thrombosis, inflammation and clotting factors are removed. This technique of removing inflammatory milieu from the body may be the necessary step to allow regeneration of the damaged organ. Successful therapies of myocardial infarction (ASA, heparin, wafarin, antiplatelets, plavix, β blockers, ACE inhibitors, hypothermia and cardiac rehabilitation) are all anti-inflammatory therapies. This case suggests that a more robust study of inflammation in aetiology and recovery of myocardial infarction should be studied as intensely as antithrombotics.50–52
References
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.